
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Idiopathic hypoparathyroidism induced fahr’s syndrome
Ryan Stuart 1 ; Harold Duarte 1 ; Zachary Gilbert 1 ; Damian Valencia 2 *; Juan David Linares 2 ; Satish Sarvepalli 3 ; Robert Barker 4
1 Department of Internal Medicine, Kettering Medical Center, Kettering, OH, USA.
2 Department of Cardiovascular Disease, Kettering Medical Center, Kettering, OH, USA.
3 Department of Infectious Diseases, Kettering Medical Center, Kettering, OH, USA.
4 Department of Neurocritical Care, Kettering Medical Center, Kettering, OH, USA.
*Corresponding Author : Damian Valencia
Department of Cardiovascular Disease, Kettering
Medical Center, Kettering, OH, USA.
Email: damian.valencia@ketteringhealth.org
Received : Apr 19, 2021
Accepted : May 21, 2021
Published : May 25, 2021
Archived : www.jcimcr.org
Copyright : © Valencia D (2021).
Abstract
Fahr’s Syndrome (FS) is a rare neurological disorder of abnormal calcium deposition. FS is most notably characterized by deterioration of motor function, neuropsychiatric impairment and seizures. These symptoms are primarily due to calcification of the basal ganglia and cerebral cortex. Although there are currently no curative therapies, treatments are available which can significantly improve quality of life, making early diagnosis and identification of etiology essential. Hypoparathyroidism with intracranial calcification is extremely rare clinically. Here we present a case of idiopathic hypoparathyroidism induced Fahr’s syndrome with classic symptomatology, imaging of examination findings and extensive cerebral calcifications.
Keywords: Fahr’s Syndrome; idiopathic hypoparathyroidism.
Citation: Stuart R, Duarte H, Gilbert Z, Valencia D, David J, et al. Idiopathic hypoparathyroidism induced fahr’s syndrome. J Clin Images Med Case Rep. 2021; 2(3): 1162.
Introduction
First described in 1930 by the German pathologist, Karl Theodor Fahr, Fahr’s Syndrome (FS) is a rare neurological disorder of abnormal calcium deposition. FS is characterized by deterioration of motor function, neuropsychiatric impairment and seizures [1]. These symptoms are due to calcifications of the basal ganglia and cerebral cortex. Although there are currently no curative therapies, treatments are available which can significantly improve quality of life, making early diagnosis and identification of etiology essential. Here we present a case of idiopathic hypoparathyroidism induced Fahr’s syndrome with classic symptomatology, imaging of examination findings and extensive cerebral calcifications.
Case report
A 29-year-old male with a past medical history of epilepsy presented with progressive abdominal pain, nausea, vomiting, diarrhea, fever and chills. Vomitus and diarrhea were non bloody and non-bilious. Symptoms reportedly began one week prior to presentation. On review of systems, it was revealed that the patient was also experiencing frequent falls. The patient’s mother reported that he had also been having visual hallucinations the day of presentation.
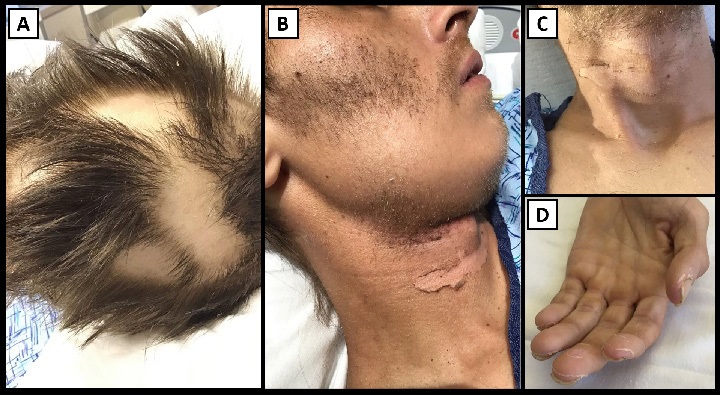
On evaluation, the patient was found to be febrile (103.8°F), hypoxic with pulse oximeter reading of 58% on room air, tachypneic (43 respirations/minute), tachycardic (146 beats/minute), and hypotensive (90/60 mmHg). Pertinent physical examination findings included bilateral rales, alopecia areata, alopecia barbae, skin desquamation around the neck and hyperkeratosis of the hands (Figure 1). Initial serologic studies were significant for sodium 128 mmol/L, potassium 2.9 mmol/L, BUN 40 mg/ dL, creatinine 1.5 mg/dL, GFR 55 mL/min, calcium 6.5 mg/dL, ionized calcium 0.79 mmol/L, total bilirubin 2.2 mg/dL, lactate 3.5 mmol/L, AST 625 U/L, and ALT 246 U/L. Chest x-ray showed a right lower lobe infiltrate and consolidation.
Given the preliminary diagnosis of severe sepsis secondary to community-acquired pneumonia, the patient was given a 3 L normal saline bolus, started on norepinephrine infusion, supplemental oxygen (3 L via nasal cannula), and antibiotics (ceftriaxone 2g IV and azithromycin 500 mg IV every 24 hours). Antibiotics were later changed to levofloxacin 750 mg IV every 24 hours for a planned 14 day course for coverage of Legionella, as the urine antigen returned positive.
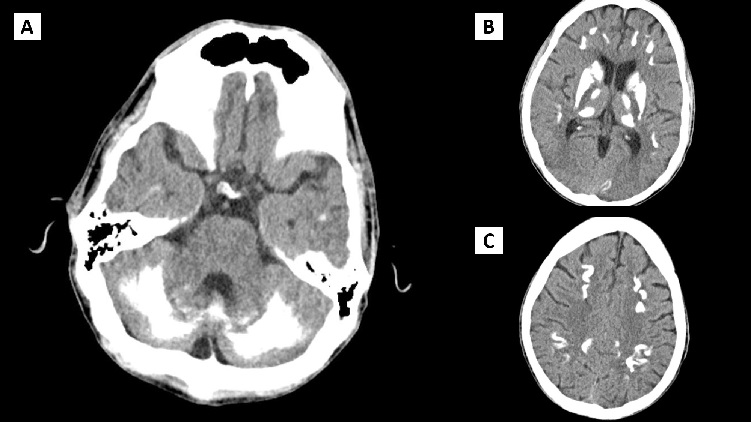
Unfortunately, the patient’s respiratory status continued to decline and he was eventually intubated, sedated and mechanically ventilated. Renal function also declined (creatinine 4.3 mg/dL), likely as a consequence of Acute Tubular Necrosis (ATN) from severe sepsis with shock. After several days of antibiotics, aggressive hydration and vasopressor support, the patient was extubated. Although the patient experienced some improvements, his agitation, impulsive behavior, confusion and severe anxiety remained unchanged. The patient subsequently experienced a fall with resulting head trauma. Computed Tomography (CT) of the head was obtained showing extensive symmetric calcifications in the subcortical and cerebral hemispheres, basal ganglia, dentate nuclei and cerebellum (Figure 2). Further serologic testing revealed a PTH of <3 pg/mL and 1,25-Dihydroxycholecalciferol of 38.5 ng/mL.
A diagnosis of idiopathic hypoparathyroidism with resultant Fahr’s syndrome was established. The patient was started on calcitriol 0.5 mcg daily, carbamazepine 200 mg twice daily, and risperidone 1 mg twice daily. After clinical stabilization and near return to baseline functional status, the patient was discharged home.
Discussion
Fahr’s Syndrome (FS) is a rare neurological disorder of abnormal symmetric calcium deposition, primarily in the basal ganglia, cerebellum dentate nuclei, thalami, cerebellum, hippocampus, and cerebral hemisphere white matter [1]. The calcifications are calcium carbonate and calcium phosphate [2]. Prevalence of this disorder is thought to be less than 1 in 1,000,000 [3]. Symptoms include deterioration of motor function, dysphagia, dysarthria, slurred speech, ataxia, athetosis, headache, seizures, dementia, concentration, spasticity, alopecia and ocular impairments [2].
It is common for laboratory abnormalities to be absent; typically with no infectious, traumatic, or toxic etiology identified. Magnetic Resonance Imaging (MRI) is typically the modality of choice for detecting most intracranial abnormalities, although in cases of calcified lesions, it is less helpful. Susceptibility Weighted Imaging (SWI) is a novel MRI technique that has been shown to detect intracranial calcifications similar to CT imaging [4]. The current gold standard for imaging intracranial calcifications is CT scan of the brain without contrast [5].
There are many predisposing conditions for FS including hyperparathyroidism, hypoparathyroidism, pseudohypoparathyroidism, hypoxia at birth, toxin exposure (lead, carbon monoxide, chemotherapy medications), radiation therapy, infectious etiology, congenital TORCH infections (toxoplasmosis, rubella, cytomegalovirus, herpes simplex, syphilis, parvovirus, zika, and varicella zoster), Human Immunodeficiency Virus, tuberculosis, astrocytoma, sarcoidosis, and inherited neurodegenerative disorders [6-9].
The mechanism behind idiopathic hypoparathyroidism, as in the case presented above, is not completely understood currently. Parathyroid hormone is a key calcium-regulatory hormone for calcium homeostasis. As a result of hypoparathyroidism, serum calcium decreases as serum phosphorus increases. This elevated phosphorus consequently creates elevated levels of calcium-phosphorus binding resulting in ectopic soft tissue calcifications [10]. These calcifications, when occurring in the brain, are suspected of causing Fahr’s disease. Idiopathic hypoparathyroidism induced FS is diagnosed based on findings of hypocalcemia, hyperphosphatemia, and hypoparathyroid hormone with additional findings of calcium deposition in the basal ganglia seen most commonly on CT imaging. As previously mentioned, these effects on the basal ganglia result in abnormal neuropsychiatric motor activity [11].
Management is currently aimed at symptom control and treating the etiology of FS. Various pharmacological therapies are available for the treatment of psychiatric sequelae, and will not be covered here in detail. Specifically pertaining to FS, clonazepam and atypical antipsychotics were found to be particularly efficacious [12]. Treatment of seizure disorders has been well established, and society recommendations do not change while treating FS. Antipsychotics and mood stabilizers such as haloperidol or lithium carbonate have been linked with improvement in psychotic symptom management [13]. Oxybutynin has been proven efficacious in the treatment of urinary incontinence [14]. In regards to hypoparathyroidism related FS, treatment with 1-alpha-hydroxyvitamin D3 and corticosteroids has been found to reverse some neurological deficits, including seizures and movement disorders [15,16]. Treatment can result in profound clinical improvement, as evidenced by a reported case of a 3 year old with reversal of mental retardation after correction of hypoparathyroidism [17]. Unfortunately, patient’s with FS have a variable prognosis that is independent of the extent of intracranial calcification [18].
Conclusion
Early diagnosis and appropriate evaluation of possible etiologies, provides opportunity to treat the underlying processes. Although treatment is unfortunately not curative, it can still significantly improve quality of life and prevent further morbidity and mortality associated with late diagnosis.
References
- Toscano M, Canevelli M, Giacomelli E, et al. Transcranial sonography of basal ganglia calcifications in fahr disease. J Ultrasound Med. 2011; 30: 1032-1033.
- Saleem S, Aslam HM, Anwar M, et al. Fahr’s syndrome: Literature review of current evidence. Orphanet J Rare Dis. 2013; 8.
- Manyam B V., Walters AS, Narla KR. Bilateral Striopallidodentate calcinosis: Clinical characteristics of patients seen in a registry. Mov Disord. 2001; 16: 258-264.
- Wu Z, Mittal S, Kish K, Yu Y, Hu J, et al. Identification of calcification with MRI using susceptibility-weighted imaging: A case study. J Magn Reson Imaging. 2009; 29:177-182.
- Shahidi GA, Safdarian M. Fahr disease: Idiopathic basal ganglia calcification. Iran J Neurol. 2017; 16: 53-54.
- Mehrjardi MZ. Is Zika Virus an Emerging TORCH Agent? An Invited Commentary. Virology (Auckl). 2017; 8: 1178122X17708993.
- TORCH Syndrome - NORD (National Organization for Rare Disorders). Accessed April 16, 2021.
- Abdelrahman M. Radaideh DMJFHH. Prevalence of incidental basal ganglia calcification on routine brain computed tomography -. Rawal Med J. 2012; 37: 6-8.
- Donaldson I, Marsden CD, Schneider S, Bhatia K. Marsden’s Book of Movement Disorders. Oxford University Press. 2012.
- Marques Mendes E, Meireles-Brandão L, Meira C, Morais N, Ribeiro C, Guerra D. Primary Hypoparathyroidism Presenting as Basal Ganglia Calcification Secondary to Extreme Hypocalcemia. Clin Pract. 2018; 8: 5-7.
- Zhou YY, Yang Y, Qiu HM. Hypoparathyroidism with Fahr’s syndrome: A case report and review of the literature. World J Clin Cases. 2019; 7: 3662-3670.
- Chow KS, Lu DN. Primary hypoparathyroidism with basal ganglia calcification: report of a case. Acta Paediatr Sin. 1989; 30: 129- 133.
- Munir KM. The treatment of psychotic symptoms in Fahr’s disease with lithium carbonate. J Clin Psychopharmacol. 1986; 6: 36-38.
- Ramos EM, Oliveira J, Sobrido MJ, Coppola G. Primary Familial Brain Calcification. University of Washington, Seattle; 1993. Accessed April 16, 2021.
- El Maghraoui A, Birouk N, Zaim A, Slassi I, Yahyaoui M, Chkili T. SYNDROME DE Fahr Et Dysparathyroidie. 3 Observations. Press Medicale. 1995; 24: 1301-1304.
- Abe S, Tojo K, Ichida K, et al. A Rare Case of Idiopathic Hypoparathyroidism with Varied Neurological Manifestations. Intern Med. 1996; 35: 129-134.
- Lauterbach EC, ed. Psychiatric Management in Neurological Disease. First. American Psychiatric Press, Inc; 2000.
- Rastogi R, Singh AK, Rastogi UC, Mohan C, Rastogi V. Fahr’s syndrome: A rare clinico-radiologic entity. Med J Armed Forces India. 2011; 67: 159-161.