
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
COVID-19 patient with elevated D-dimer. Is anticoagulation the answer? A case report
David El-Qutob*; Patricia García-Sidro; María Nieto; Francisco J Carrera- Hueso
Allergy, Pneumology and Pharmacy Departments, Hospital Universitario de La Plana, Vila-Real, Spain.
*Corresponding Author : David El-Qutob
Unit of Allergy, Universitary Hospital of La Plana,
Vila-Real, Carretera Vila-Real-Burriana km 0.5,
Vila-Real (Castellon) 12540, Spain.
Email: elqutob@comv.es
Received : Apr 20, 2021
Accepted : May 21, 2021
Published : May 25, 2021
Archived : www.jcimcr.org
Copyright : © El-Qutob D (2021).
Abstract
Context: We are progressively learning about COVID-19 every day. An aspect that we would like to highlight and that is becoming increasingly clear is that patients develop a hypercoagulable state that causes microthrombi and becomes life threatening. We are considering starting the use of early anticoagulation in these cohort of patients who become critically ill to halt and prevent progression of the disease.
Case report: We present a case report of a SARS-CoV-2 infected patient admitted in a hospital in Vila-real, Spain. We present the characteristics and evolution of laboratory parameters of our patient during the admission in our hospital. The patient needed intubation and was transferred to the Intensive Care Unit (ICU) where the patient continues evolution.
Conclusions: Probably these patients must be anticoagulated earlier and for a longer duration along the duration of the disease.
Keywords: D-dimer; SARS-CoV-2; Hypercoagulability
Citation: El-Qutob D, García-Sidro P, Nieto M, Carrera- Hueso FJ. COVID-19 patient with elevated D-dimer. Is anticoagulation the answer? A case report. J Clin Images Med Case Rep. 2021; 2(3): 1163.
Introduction
On 11 March, the World Health Organization declared a global pandemic caused by a new virus of the family Coronaviridae that has later been called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1].
It has been postulated that there are three phases of the disease; the first characterized by an incubation period associated with mild symptoms affecting the upper respiratory tract, dry cough and fever; a second phase when the virus replicates and affects lungs; and the third phase of systemic hyperinflammation with extra pulmonary systemic syndrome affecting the heart, intestine, liver, kidney and central nervous system, that could cause Acute Respiratory Distress Syndrome (ARDS) by a cytokine storm [2]. COVID-19 does not have specific antiviral drug treatment currently, so the treatment of the disease is mainly focused on symptomatic treatment and oxygen therapy, although hundreds of clinical trials are being conducted (www.clinicaltrials.org). Therefore, the therapeutic attitude is empirical. The treatment to be performed is also different in the three phases: in the former phase, anti-pyretic therapy, in the second phase, antivirals or drugs that inhibit viral replication, and in the third, it is addressed to decrease hyperinflammation and cytokines effect with drugs such as corticosteroids, anti-interleukin 6 (IL6) or anti-interleukin 1 (IL-1), among others [3]. It has taking especial relevance the use of low-weight molecular heparins (LWMH) in the treatment of COVID-19 patients [4].
Objective
We present a clinical case diagnosed with COVID-19 ARDS, with a typical clinical presentation but with an important alteration of the coagulation function. The study of the COVID patients admitted in our hospital was evaluated and approved by the ethics committee.
Case report
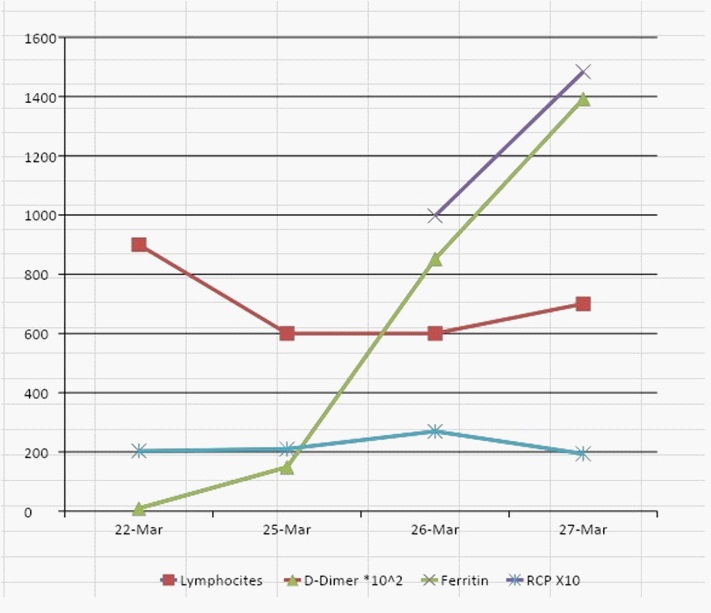
We present the case of a 61-year-old man with dry-cough, fever up to 38.5o C, dysnea to minimal efforts and diarrhea. No relevant medical history and chronic intake of medication. Chest x-ray showed bilateral lung involvement with a consolidative pattern and a predominantly ground-glass pattern. Laboratory analysis showed lymphocytes 0.9 x 10 3 /L, D-dimer 923 g/mL, fibrinogen 1113 mg/dL, Aspartate Aminotransferase (AST) 66 U/L, Glutamic-Pyruvic Transaminase (GPT) 67 U/L, Lactate Dehydrogenase (LDH) 457 U/L, C-Reactive Protein (CRP) 20.33 mg/ dL. Hypoxemia was not observed at beginning of hospitalization. Polymerase Chain Reaction (PCR) was positive to SARS-CoV-2 (COVID-19). Initially, patient was treated with azithromycin (500 mg each day), lopinavir/ritonavir (400/100 mg each 12 hours) and hydroxychloroquine (200 mg each 12 hours) empirically following literature recommendations [3]. In addition, ceftriaxone (2 g each day), enoxaparin (40 mg each day), n-acetylcysteine (600 mg each 12 hours) was initiated. At third day (eighth day with symptoms), the patient presented respiratory deterioration and fever again (not presented the first two days of hospitalization) with more bilateral lung opacities in chest x-ray, and lymphocytes 0,6 x 103 /μL, D-dimer 14851 μg/mL, and CRP 20.9 mg/dL. Dose of enoxaparin was augmented until therapeutic dose (60 mg each 12 hours) of Venous Thromboembolism (VTE) and lopinavir/ritonavir was removed. Next day, 9th onset of symptoms, the patient maintains fever of up to 38o C and the hypoxemia increased. Laboratory data showed lymphopenia 0.6 x 103 /L (equal to previous), D-dimer 85,225 µg/mL, ferritin 997 ng/mL and CRP 26.92 mg/dL. A dose of tocilizumab 400 mg intravenous was administered and 3 bolus of methylprednisolone intravenous 125 mg/day. Patient did not recover, and treatment with Bilevel Positive Pressure Airway (BiPAP) (IPAP/EPAP 17/14 cm H2 O) associated with 15 lpm by total face mask showed immediate improvement of clinical and gasometrical values. On the fifth day (10th onset of symptoms), there was not fever but respiratory work is increased. Laboratory analysis showed pO2 87.5 mmHg with PaFi 174 mmHg (pO2 /FiO2 ), lymphopenia 0.7 x 103 /L, D 139.202, g/mL, prothrombin time 15 seconds, CRP 19.38 mg/dL and ferritin 1484 ng/mL. See in Figure 1 the evolution of laboratory data.
A local general university hospital ethics committee of approved this study (approved May 25, 2020) and waived the need of informed consent.
Given the absence of improvement despite the onset of noninvasive ventilation, the patient is intubated and transferred to the Intensive Care Unit (ICU) of another Hospital Center where the patient continued evolution.
Discussion
Plasma D-dimer is a circulating peptide degradation product of fibrin. Higher levels of D-dimer indicate hyper-fibrinolysis and a risk of thrombosis [5]. There are multiple causes of D-dimer elevated, physiological (age and pregnancy) or pathological. In the last there are acute coronary syndromes, connective tissue disease, thromboembolism, infection, liver disease, renal disease, stroke, surgery, trauma, heart failure, malignancy or systemic inflammatory response syndrome [6].
Elevated levels of D-dimer are associated with disease activity and inflammation in patients with granulomatosis with polyangiitis [7]. These patients are in hypercoagulable stage risk factor for Venous Thromboembolism (VTE) and a longer duration of anticoagulation in this group of patients have been recommended.
Systemic microthrombi in the circulatory system and hemorrhage in the affected organs result from non-coordinated responses between the coagulation and fibrinolysis systems in severe COVID-19 patients [8]. Some authors have suggested that LWMH therapy may also alleviate the hypercoagulable state in patients [9].
The progression of the level of D-dimer in our patient should alert us that a VTE process had initiated. Probably, VTE is responsible for irreversible damage to internal organs and final death of the patient. Therefore, daily monitoring along with the other prognostic factors is mandatory.
In our opinion, like other authors, [4] any patient without any associated risk factor but with a moderate COVID-19 infection requiring hospitalization, a cause of interstitial bilateral pneumonia and D-dimer level above 600 mg/dL, should receive prophylactic doses with LMWH, for example enoxaparin at dose 1 mg/kg/day subcutaneous or equivalent. The duration of treatment should last until the end of the disease, which is estimated at least three weeks. Articles relating to COVID-19 and D-Dimer that were found through searching the medical literature databases (June 30, 2020) are summarized in Table 1. Case reports on SARS-CoV-2 infected patients with elevated D-dimer in the literature are showed in Table 2.
Table 1: Articles relating to COVID-19 and D-Dimer that were found through searching the medical literature databases (June 30, 2020)
Database |
Search strategies |
Papers found |
Related papers |
Web of Science |
COVID-19 AND Heparin AND Blood coagulation |
15 |
2 |
PubMed |
COVID-19 AND Heparin AND Blood coagulation |
14 |
1 |
Scielo |
COVID-19 AND Heparin AND Blood coagulation |
0 |
0 |
Table 2: Case reports on SARS-CoV-2 infected patients with elevated D-dimer in the literature
Author |
Publication year |
Escher et al15 |
2020 |
Ma et al16 |
2020 |
Our patient had a similar profile than other severe or deceased cases with fever, cough, and dyspnea, presenting progressive lymphopenia, and elevated lactate dehydrogenase, C-reactive protein, ferritin, and D-dimer [10,11]. Gao et al observed that IL-6 and D-dimer were closely related to the occurrence of severe COVID-19 in the adult patients, and their combined detection had the highest specificity and sensitivity for early prediction of the severity of COVID-19 [12]. Zhang et al presented six patients who received LMWH treatment, after which their D-dimer and Fibrinogen Degradation Product (FDP) decreased, but there was no significant improvement in clinical symptoms, and five patients died finally [13]. However, Tang et al observed better prognosis in severe COVID-19 patients with anticoagulant with LMWH [14]. But probably, the use of LWMH must be earlier as Lin et al recommended [4].
Conclusion
D-dimer is a clear prognostic marker of severity. The existence of hypercoagulation status in critical COVID-19 patients should be monitored closely, and probably these patients must be anticoagulated earlier and for a longer duration along the duration of the disease, estimated usually in three weeks.
Authors’ contributions: El-Qutob D, García-Sidro P, Nieto Mand Carrera FJH contributed in conceptualization (equal), writing-original draft (equal) and writing-review and editing (equal).
References
- World Health Organization. WHO Statement Regarding Cluster of Pneumonia Cases in Wuhan, China. 2020.
- Siddiqi HK, Mehra MR. COVID-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal. J Heart Lung Transplant. 2020; 39: 405-407.
- Zhai P, Ding Y, Wu X, et al. The epidemiology, diagnosis and treatment of COVID-19. Int J Antimicrob Agents. 2020; 55: 105955.
- Lin L, Lu L, Cao W, Li T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection − a review of immune changes in patients with viral pneumonia. Emerg Microbes Infect. 2020; 9: 727-732.
- Zhang J, Song Y, Shan B, et al. Elevated level of D-dimer increases the risk of stroke. Oncotarget. 2017; 9: 2208-2219.
- Kabrhel C, Mark Courtney D, Camargo CA Jr, et al. Factors associated with positive D-dimer results in patients evaluated for pulmonary embolism. Acad Emerg Med. 2010; 17: 589-597.
- Borowiec A, Dabrowski R, Kowalik I, et al. Elevated levels of ddimer are associated with inflammation and disease activity rather than risk of venous thromboembolism in patients with granulomatosis with polyangiitis in long term observation. Adv Med Sci. 2020; 65: 97-101.
- Ji HL, Zhao R, Matalon S, Matthay MA. Elevated plasmin(ogen) as a common risk factor for COVID-19 susceptibility. Physiol Rev. 2020; 100: 1065-1075.
- Li T, Lu H, Zhang W. Clinical observation and management of COVID-19 patients. Emerg Microbes Infect. 2020; 9: 687-90.
- Chen G, Wu D, Guo W, et al. Clinical and immunologic features of severe and moderate Coronavirus Disease 2019. J Clin Invest. 2020; 130: 2620-2629.
- Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020; 368: m1091.
- Gao Y, Li T, Han M, et al. Diagnostic Utility of Clinical Laboratory Data Determinations for Patients with the Severe COVID-19. J Med Virol. 2020; 92: 791-796.
- Zhang Y, Cao W, Xiao M, et al. [Clinical and coagulation characteristics of 7 patients with critical COVID-2019 pneumonia and acro-ischemia]. Zhonghua Xue Yye Xue Za Zhi. 2020; 41: E006.
- Tang N, Bai H, Chen X, et al. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020; 18: 1094-1099.
- Escher R, Breakey N, Lämmle B. Severe COVID-19 infection associated with endothelial activation. Thromb Res. 2020; 190: 62.
- Ma J, Xia P, Zhou Y, et al. Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19. Clin Immunol. 2020; 214: 108408.