
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Renal biopsy teaching case: A patient with scleroderma, hypertension, acute kidney injury and PR3 ANCA positivity
Sam Kant*; Avi Rosenberg; Fred Wigley; Duvuru Geetha D
Johns Hopkins University Hospital, Baltimore, MD, United States.
*Corresponding Author : Sam Kant
Johns Hopkins University Hospital, Baltimore, MD,
United States.
Email: skant1@jhmi.edu
Received : Apr 20, 2021
Accepted : May 24, 2021
Published : May 27, 2021
Archived : www.jcimcr.org
Copyright : © Kant S (2021).
Citation: Kant S, Rosenberg A, Wigley F, Geetha DF. Renal biopsy teaching case: A patient with scleroderma, hypertension, acute kidney injury and PR3 ANCA positivity. J Clin Images Med Case Rep. 2021; 2(3): 1168.
Introduction
Scleroderma Renal Crisis (SRC) is the most common cause of Acute Kidney Injury (AKI) in scleroderma and occurs early during the disease course while ANCA Associated Vasculitis (AAV) is a rare cause of acute kidney injury occurring late in the disease course. We report a case of AKI with positive PR3 ANCA serology late in the disease course with a renal biopsy revealing findings of SRC.
Case report
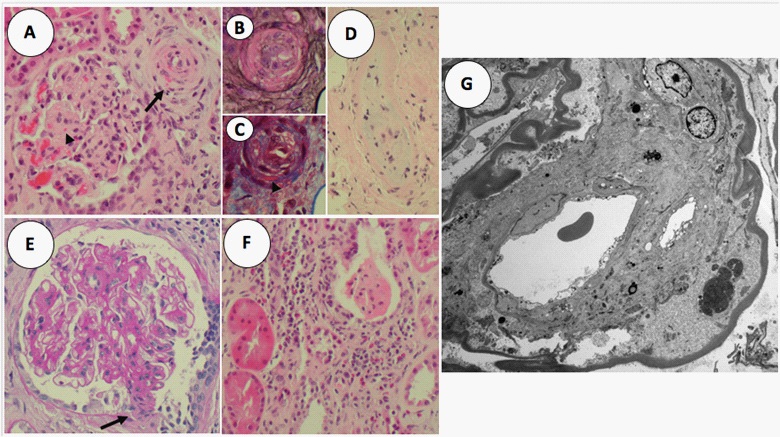
A 65-year-old African-American male, with a history of limited scleroderma (SSc) for 16 years, complicated by severe gastrointestinal dysmotility and interstitial lung disease, presented to the clinic with elevated blood pressure of 190/100 mmHg, on a background of previously well-controlled blood pressure. He was found to have an acute kidney injury with a serum creatinine of 2.5 mg/dL, compared to his baseline of 1.3 mg/dL. Urine studies demonstrated microscopic hematuria, with 3.4 grams of proteinuria. Hemoglobin was 7.4 g/L with no evidence of hemolysis and normal platelet count. Serologies revealed a positive c-ANCA serology with PR3 positivity at 97.4 IU/mL with negative ANA, ds-DNA, Scl-70, anti-smith, anti-Ro, Anti-La, and RNP. A renal biopsy was performed which demonstrated arteriolar microangiopathy with fibrinoid necrosis and concentric lamellation with no evidence of ANCA GN (Figure 1A-G). He was treated with ACE inhibitor with improvement in blood pressure and serum creatinine (1.7 mg/dl).
Discussion
We report the first case of late onset SRC associated with PR3 ANCA positivity. Overlap syndrome of scleroderma and ANCA vasculitis is a well-recognized but rare phenotype. Majority of these overlap cases are MPO ANCA positive and vasculitic manifestation is universal in these cases [1,2]. Our case is unique in being PR3 ANCA positive without any vasculitic manifestation but with presentation as late onset SRC.
Derret-Smith and colleagues, demonstrated a possibility of shared HLA haplotypes with SSc/AAV, especially in the HLA-DQ region [2]. Further research in this area may reveal common immunogenetic factors involved in patients with Ssc/AAV overalap. Alternatively, PR3 ANCA in our patient could belong to a repertoire of natural antibodies [3].
This case of late onset scleroderma renal crisis highlights that atypical presentations of scleroderma renal crisis can exist, and concomitant ANCA positivity can be misleading in such situations. Therefore, it is imperative that if a scleroderma patient demonstrates atypical features- an expedient renal biopsy should be pursued.
References
- Arad U, Balbir-Gurman A, Doenyas-Barak K, et al. Anti-neutrophil antibody associated vasculitis in systemic sclerosis. Semin Arthritis Rheum. 2011; 41: 223-229.
- Derrett-Smith EC, Nihtyanova SI, Harvey J, et al. Revisiting ANCA-associated vasculitis in systemic sclerosis: clinical, serological and immunogenetic factors. Rheumatology (Oxford) 2013; 52: 1824-1831.
- Cui Z, Zhao MH, Segelmark M, et al. Natural autoantibodies to myeloperoxidase, proteinase 3, and the glomerular basement membrane are present in normal individuals. Kidney Int. 2010; 78: 590-597.