
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Acute anterior myocardial infarction complicated by a large ventricular septal defect
Yi Ming1,2*; Cao Qian1; Liu Qiang1,2
1 Department of Fu Wai Hospital Chinese Academy of Medical Sciences, Shenzhen (Shenzhen Sun yat-sun Cardiovascular Hospital), Guangdong, Shenzhen 518057, PR China.
2 Department of Clinical Medicine, University of South China, Hunan, Hengyang 421001, PR China.
*Corresponding Author : Yi Ming
Department of Chinese Academy of Medical Sciences Fu
Wai Hospital Shen Zhen Hospital, Shenzhen Sun yat-sun
Cardiovascular Hospital, Guangdong, Shenzhen 518057,
PR China.
Email: mingming8909@163.com
Received : Apr 20, 2021
Accepted : May 24, 2021
Published : May 27, 2021
Archived : www.jcimcr.org
Copyright : © Ming Y (2021).
Citation: Ming Y, Qian C, Qiang L. Acute anterior myocardial infarction complicated by a large ventricular septal defect. J Clin Images Med Case Rep. 2021; 2(3): 1169.
Clinical image description
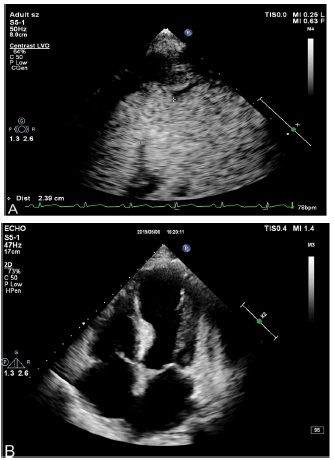
Post-Infarction Ventricular Septal Defect (PIVSD) are a rare complication of Acute Myocardial Infarction (AMI). According to clinical guidelines, surgical repair of a PIVSD is the recommended acute-stage course of treatment. Nevertheless, thoracotomy is not always clinically suggested for patients with unstable hemodynamics and otherwise at high risk. Currently, percutaneous interventional closure of a PIVSD represents an alternative therapy, and an attractive option for particular patients [1,2]. Here we report a 67-year-old man was transferred to Shenzhen Sun yat-sen Cardiovascular Hospital to evaluate a PIVSD and undergo repair. Echocardiography confirmed a large Ventricular Septal Defect (VSD) and significant left-to-right shunt (Figure 1a). Few reports of the closure of a PIVSD at an acute/subacute stage have been previously published. An interventional closure treatment (Amplatzer Septal Occluder device) was successfully performed after bridging to a subacute stage through use of mechanical circulatory backup (Figure 1b).
Declarations
Ethics approval and consent to participate: Ethics approval for the study was given by Fu Wai Hospital Shenzhen Hospital. ChiCTR2100043897.
Consent for publication: The report was approved by the ethics review committee of our institution (Fu Wai Hospital Shenzhen Hospital, Guangdong) and consent was obtained from the patient and his family for their personal or clinical details along with any identifying images to be published in this study.
Availability of data and materials: All available information is contained within the present manuscript.
Competing interests: The authors declare that they have no competing interests.
Funding: The work was supported partly by the Shenzhen Science and Technology Research and Development Fund (NO JCY20180302173849459).
Authors' contributions: YM, CQand LQ were involved in compilation of data and major contributors writing the manuscript. CQ performed the transthoracic echocardiogram and follow up. LQ performed the myocardial perfusion imaging. All authors have read and approved the submitted manuscript
Acknowledgements: We are grateful for the contribution and support of the family members.
References
- Tai S, Tang JJ, Tang L, et al. Management and Outcome of Ventricular Septal Rupture Complicating Acute Myocardial Infarction: What Is New in the Era of Percutaneous Intervention?. Cardiology. 2018; 141: 226-232.
- Moreyra AE, Huang MS, Wilson AC, et al. Trends in incidence and mortality rates of ventricular septal rupture during acute myocardial infarction. The American journal of cardiology. 2010; 106: 1095-1100.