
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Unusual presentation of an intracochlear schwannoma
Sean Holmes1*; Jeremy Watson2; Katherine Babin2; Gauri Mankekar1
1 LSU Shreveport Dept of Otolaryngology/Head and Neck Surgery, LSU Health Shreveport, 1501 Kings Highway, Shreveport, LA, 71103, USA
2 School of Medicine, LSU Health Shreveport, 1501 Kings Highway, Shreveport, LA, 71103, USA.
*Corresponding Author: Sean Holmes
Otolaryngology Resident, Department of Otolaryngology/HNS, LSU Health Shreveport, 1501 Kings Highway,
Shreveport, LA 71103, USA.
Email: sholm6@lsuhsc.edu
Received : Apr 22, 2021
Accepted : May 25, 2021
Published : May 28, 2021
Archived : www.jcimcr.org
Copyright : © Holmes S (2021).
Abstract
In this report, the authors discuss the case of a 49-year-old male presenting with sudden onset moderately severe left-sided Sensorineural Hearing Loss (SNHL), tinnitus, left otalgia, and disequilibrium. Prior to referral to our facility, an MRI was obtained which demonstrated non-specific asymmetric enhancement of the left cochlea that was initially suspected to be labyrinthitis. Patient was treated with valacyclovir and a prednisone burst-taper prior to referral. Despite this treatment, his left SNHL worsened, and he was noted to have left-sided peripheral weakness on Videonystagmography (VNG). Upon referral to our facility, MRI demonstrated an Intra-Cochlear Schwannoma (ICS), with possible associated hemorrhage into the cochlea. After discussion of treatment options, repeat imaging in 6-month interval demonstrated stable persistence of the lesion with no growth. The patient is currently being followed with a “Wait-andScan” regimen. Sudden unilateral SNHL is a rare presenting symptom for ICS and this case highlights not only the rarity in presentation, but also the complexity in diagnosis due to the possibility of intracochlear hemorrhage complicating the imaging work-up.
Keywords: Intra-labyrinthine schwannoma; vestibular schwannoma; sensorineural hearing loss; disequilibrium.
Abbreviations: SNHL: Sensorineural Hearing Loss; VNG: Videonystagmography; ICS: Intracochlear Schwannoma; MRI: Magnetic Resonance Imaging; IAC: Internal Auditory Canal; ILS Intra-Labyrinthine Schwannomas; CT: Computed Tomography; SRT: Speech Reception Threshold.
Citation: Holmes S, Watson J, Babin K, Mankekar G. Unusual presentation of an intracochlear schwannoma. J Clin Images Med Case Rep. 2021; 2(3): 1172.
Introduction/background
Vestibular Schwannomas (VS) are benign neoplasms of the eighth cranial nerve which typically originate from the vestibular ganglion within the Internal Auditory Canal (IAC), particularly Scarpa’s ganglion. They most commonly arise in the IAC and grow concentrically in a medial direction to involve the cerebellopontine angle as they increase in size. This, however, is not the only route of tumor growth, as some IAC Schwannomas may rarely expand laterally from their IAC origin, to involve the labyrinthine structures of the inner ear. Even rarer are the Intra-Labyrinthine Schwannomas (ILS). These lesions are solely contained within the bony labyrinth, have no IAC involvement, and represent a separate pathologic entity from the more commonly reported vestibular schwannomas which arise in the IAC and extend laterally to involve both the IAC and labyrinth to which was previously alluded.
ILS are benign, slow growing tumors that typically arise from the Schwann cells associated with distal branches of the cochlear, superior vestibular, and inferior vestibular nerves [1]. These Schwann cell-containing lesions tend to occur in the modiolus and the basal turn of the cochlea along the path of spiral ganglion dendrites [2]. The clinical presentation of IAC VS produces a combination of otologic signs and symptoms with unilateral, progressive hearing loss one of the most common at presentation (95%). The less commonly reported resulting symptoms include tinnitus, imbalance, vertigo, and aural fullness which can present alone or in combination with one another [3]. Sudden SNHL is an exceedingly rare clinical presentation for ICS which has been minimally reported in the literature regarding this topic.
The majority of previously reported cases have been largely restricted to cadaveric studies and autopsy reports, with a paucity of literature on how to diagnose and manage these lesions in a clinical setting of an otherwise healthy patient. Interestingly, these lesions have also been found within the semicircular and reported as an incidental intra-operative finding during labyrinthectomy for refractory Meniere’s disease. Due to their rarity and overlap in presentation with other disease processes including but not limited to Meniere’s disease, accurate diagnosis of these lesions remains a challenging task and is often delayed. Despite the development of high-resolution, gadolinium-enhanced Magnetic Resonance Imaging (MRI) that has increased the frequency of diagnosis of these lesions during the preoperative period, they can remain clinically occult for several years in certain patients [4].
Case presentation
A 49-year-old Caucasian male was referred to our facility from a local otolaryngologist for further evaluation regarding his presentation. Eight months prior to referral, the patient experienced sudden onset SNHL of left ear. At that time, the patient additionally presented with progressively worsening left sided tinnitus that was high-pitched and constant in nature, as well as left otalgia and disequilibrium. The patient also reported a 15-year history of occupational noise exposure. The patient’s family history was significant for a brainstem cyst in his mother as well as a brain cyst associated with compression of the trigeminal nerve in his father. An otologic examination, audiometric evaluation, as well as a multi-planar multi-pulse sequence MRI of the brain with and without contrast was obtained at an outside facility for further evaluation. The results of the MRI were interpreted as inflammation of the left cochlea concerning for labyrinthitis and prompted the administration of a trial of a prednisone taper and Valtrex with a recommendation of patient follow-up in 2 weeks. After 2 weeks, the patient stated that the medical therapy administered failed to relieve his symptoms. At this time, a second audiogram was obtained for further evaluation, which prompted referral to our institution.
At the time of our initial evaluation, the patient reported constant high-pitched ringing tinnitus in the left ear with persistent disequilibrium. Vestibular therapy was initiated which resulted in some improvement but no complete resolution of his imbalance. Further work up was completed with VNG testing, a Romberg test, a Fukuda test, an autoimmune panel, and a CT of the internal auditory canal. The outside MRI images were reviewed at a multidisciplinary neuroradiology conference at our tertiary care facility for which the differential diagnosis was narrowed to ICS with possibility of mild acute hemorrhage within the cochlea. The patient was instructed to return to clinic in six months for a repeat MRI and audiologic evaluation.
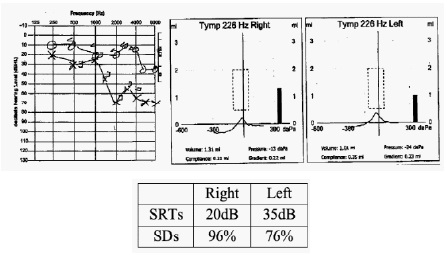
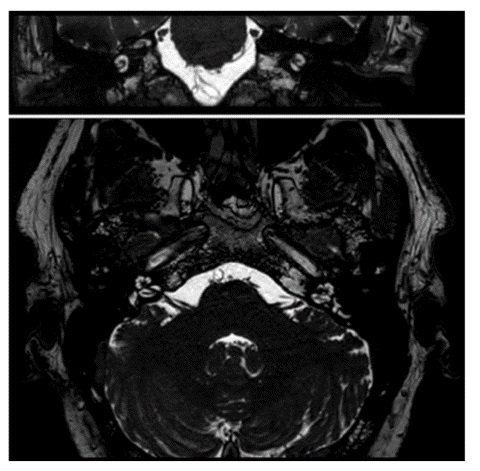
At the patient’s initial visit at the outside otolaryngology clinic eight months prior to referral, an otologic examination revealed normal ear canal, mobile tympanic membranes intact bilaterally without effusion. An audiometric evaluation was performed, which demonstrated mild to moderately severe downsloping sensorineural hearing loss for left ear and mild sensorineural hearing loss of the right ear. The Speech Reception Threshold (SRT) was 20 dB on right and 35 dB on left. Speech discriminations were 96% on right and 76% on the left, and audiogram tracings and a tympanogram was created (Figure 1). In addition, a multi-planar multi-pulse sequence MRI of the brain with and without contrast was performed and demonstrated asymmetric left-sided enhancement in the second turn of the cochlea (Figure 2)
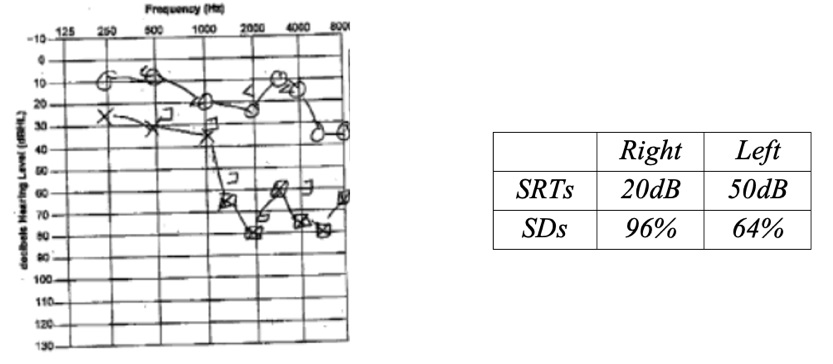
At the patients 2 week follow-up visit, the second audiogram that prompted patient referral was completed, which demonstrated worsening of the patients left-sided sensorineural hearing loss (Figure 3).
At the time of our initial evaluation, the patient was noted to have a positive Romberg test and abnormal Fukuda test, swaying to the left. The patient’s autoimmune panel was shown to be negative. Videonystagmography (VNG) demonstrated leftsided peripheral vestibular weakness, evidenced by a caloric reduced caloric response of 18% in the left ear (Figure 4).
A CT of the internal auditory canal was also obtained at our initial evaluation and demonstrated a normal appearing cochlea and vestibule with well-developed semicircular canals. (Figure 5)
At the patient’s six-month follow-up evaluation, a repeat MRI was ordered. This imaging demonstrated enhancement of a very small mass within the cochlea that was stable in size when compared to the initial MRI findings, confirmatory for the suspected diagnosis (Figure 6).
In addition to the imaging, a repeat audiometric evaluation demonstrated relatively stable left-sided SNHL (Figure 7).
After discussion of treatment options, the patient elected to proceed with a “Wait-and-Scan” approach. Serial imaging and audiograms are being performed for close surveillance. The patient continues vestibular therapy with improvement for treatment of his disequilibrium and has been followed up with our facility for a total period of 7 months since initial referral. We continue to see this patient at regular 6-month follow-up intervals and he is currently doing well.
Discussion
Intra-Labyrinthine Schwannomas (ILS) are benign neoplasms that arise de novo in the cochlea, vestibule, semicircular canals, or a combination of these structures with no extension into the Internal Auditory Canal (IAC). Currently, ILS can be subclassified into 7 groups based on the inner ear structures that are affected. The subclasses include intravestibular, intracochlear, intravestibulocochlear, transmodiolar, transmacular, transotic, and tympanolabyrinthine. Of these subclasses, the most commonly reported type of ILS is the intravestibular type and the least commonly reported type are the intravestibulocochlear and transotic types. Schwannomas that are exclusively confined to the cochlea are extremely rare [6].
ILS can occur any time between the ages of 7 and 84 with the average presenting age being approximately 52 years of age [1]. Previous reports describing patients with ILS showed that the most common presenting symptom was unilateral hearing loss (93-100%), followed by tinnitus (50%), vertigo (30-51%), imbalance, and aural fullness [4,6-10]. The hearing loss associated with ICS is most frequently classified as sensorineural and progressive in nature and is typically associated with poor speech recognition ability. However, approximately 15-32% of patients can present with hearing loss of sudden onset. There is evidence demonstrating a mixed-type hearing loss that is presumed to be the result of increased intracochlear impedance with these tumors causing a secondary endolymphatic hydrops resulting in disequilibrium and vertigo [5]. The nonfluctuating hearing loss that is typically seen in ILS could differentiate the nature of the disease from the other possible causes of hearing deterioration, indicating the necessity for high-resolution techniques of imaging [4].
Currently, MRI is the gold standard for diagnosis of ILS. Before the use of MRI, these rare benign neoplasms were incidentally identified during surgical procedures of the inner ear or during a postmortem autopsy [4,7-9,11]. Due to the recent advances in MRI and its technology, physicians have an enhanced ability to detect these small lesions within the inner ear. These tumors typically demonstrate gadolinium contrast enhancement on T1- weighted images with a “Filling Defect” seen on T2-weighted images [12].
Surgery is not imperative after a patient is diagnosed with ILS. Many factors contribute to the treatment approach including tumor size, evidence of tumor growth, the degree of hearing loss, intractable vestibular symptoms, as well as the current diagnosed patient comorbidities [6-9]. The need for surgical removal for ILS is generally reserved for tumors causing vertiginous symptomatology and for those that have extended into the internal auditory canal, cerebellopontine angle, or the middle ear [4]. Generally, patients with ILS and preserved hearing are treated with follow-up observation considering that the lesion is benign, with many of these tumors exhibiting no growth, and surgical removal resulting in complete hearing loss in the operated ear [1]. After the initial diagnosis, it is currently recommended that a follow-up examination should include rescanning at 12 months. If there is absence of tumor growth, an MRI scan should be repeated every 2 years [13].
This unique clinical presentation of ICS including sudden SNHL with disequilibrium highlights the vast array of symptoms with which ICS can present. This case also highlights the importance of follow-up imaging in patients whose symptoms do not improve.
References
- Neff BA, Willcox TO, Sataloff RT. Intralabyrinthine schwannomas. Otol Neurotol. 2003.
- Deux JF, Marsot-Dupuch K, Ouayoun M, Tran Ba Huy P, Sterkers JM, et al. Slow-growing labyrinthine masses: Contribution of MRI to diagnosis, follow-up and treatment. Neuroradiology. 1998
- Elias TGA, Perez Neto A, Zica ATS, Antunes ML, Penido N de O. Different clinical presentation of intralabyrinthine schwannomas – A systematic review. Brazilian Journal of Otorhinolaryngology. 2019.
- Magliulo G, Colicchio G, Romana AF, Stasolla A. Intracochlear schwannoma. Skull Base. 2010.
- Kennedy RJ, Shelton C, Salzman KL, Davidson HC, Harnsberger HR. Intralabyrinthine schwannomas: Diagnosis, management, and a new classification system. Otology and Neurotology. 2004.
- Zhu AF, McKinnon BJ. Transcanal surgical excision of an intracochlear schwannoma. Am J Otolaryngol - Head Neck Med Surg. 2012.
- Grayeli AB, Fond C, Kalamarides M, Bouccara D, Cazals-Hatem D, et al. Diagnosis and management of intracochlear schwannomas. Otol Neurotol. 2007.
- Jiang ZY, Kutz JW, Roland PS, Isaacson B. Intracochlear schwannomas confined to the otic capsule. Otol Neurotol. 2011.
- Miller ME, Moriarty JM, Linetsky M, Lai C, Ishiyama A. Intracochlear schwannoma presenting as diffuse cochlear enhancement: Diagnostic challenges of a rare cause of deafness. Ir J Med Sci. 2012.
- Salzman KL, Childs AM, Davidson HC, Kennedy RJ, Shelton C, Harnsberger HR. Intralabyrinthine schwannomas: Imaging diagnosis and classification. Am J Neuroradiol. 2012.
- Yoshida T, Sone M, Naganawa S, Nakashima T. Accuracy of 3.0 Tesla magnetic resonance imaging in the diagnosis of intracochlear schwannoma. Auris Nasus Larynx. 2011.
- Tieleman A, Casselman JW, Somers T, Delanote J, Kuhweide R, et al. Imaging of intralabyrinthine schwannomas: A retrospective study of 52 cases with emphasis on lesion growth. In: American Journal of Neuroradiology. 2008.
- Bittencourt AG, Alves RD, Ikari LS, Burke PR, Gebrim EMS, Bento RF. Intracochlear schwannoma: Diagnosis and management. Int Arch Otorhinolaryngol. 2014.