
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Breast MRI in the setting of breast carcinoma with suspected microcalcifications and his predictive value in breast cancer management: An interesting case report
Maria Giovanna Fava1 *; Lorena Turano2 ; Francesco Messina2 ; Maria Francesca Plutino4 ; Carmela Tebala2 ; Domenico Azzarello3 ; Grazia Calabrese2 ; Nicola Arcadi2
1 Unit of General Surgery, Great Metropolitan Hospital, Reggio Calabria, Italy
2 Unit of Radiology, Great Metropolitan Hospital, Reggio Calabria, Italy.
3Unit of Oncology, Great Metropolitan Hospital, Reggio Calabria, Italy
4Unit of Pathological Anatomy, Great Metropolitan Hospital, Reggio Calabria, Italy.
*Corresponding Author: Maria Giovanna Fava
Unit of General Surgery, Great Metropolitan Hospital
“Bianchi–Melacrino–Morelli” Via Giuseppe Melacrino
n.21, 89124 Reggio Calabria, Italy
Email: mariagiovannafava@alice.it
Received : Apr 22, 2021
Accepted : May 28, 2021
Published : Jun 02, 2021
Archived : www.jcimcr.org
Copyright : © Fava MG (2021).
Abstract
The Breast Imaging Reporting and Data System (BI-RADS®) is a standardized system of reporting breast pathology used also for Magnetic Resonance Imaging (MRI). It facilitates clear communication between the radiologist and other physicians as surgeons involved in senology, by providing a lexicon that compares breast gland structures to assessment categories in the management recommendations for the onco-surgical choices.
In 30% of all clinical cases in women, breast cancer is correlated to micro-calcifications [1] or occulted lesion as non-palpable nodule and this diagnostic management is not easy, especially if you haven’t an easy access to all the equipment of interventional methods as stereotactic biopsy or radio-pharmacological detection’s method (for example R.O.L.L., Radioguided Occult Breast Lesion Location), and if you cannot know the real distribution of suspected or malignant microcalcifications in mammography.
MRI is more accurate than mammography for prediction of residual malignancy after excisional biopsy for breast cancer with suspicious micro-calcifications [2,3].
MRI’s report often influences the surgical performance. MRI can be useful to correlate malignant microcalcifications with pathological tumor size and to allow the pre-operative drawing in onco-plastic surgery for breast cancer. MRI might be more reliable for predicting residual tumor size after an onco-plastic surgical procedure or a conservative mastectomy, with significant influence on surgical outcomes and disease free survival and risk of relapse [4,5].
Keywords: Breast cancer; Breast MRI; Microcalcifications; Multidisciplinary consultation; Breast conservative surgery.
Citation: Fava MG, Turano L, Messina F, Plutino MF, Tebala C, et al. Breast MRI in the setting of breast carcinoma with suspected microcalcifications and his predictive value in breast cancer management: An interesting case report. J Clin Images Med Case Rep. 2021; 2(3): 1175.
Introduction
MRI of the breast remains controversial as an adjunct to determine candidacy for breast conservation, but prospective randomized clinical trials are underway to define the role of MRI in newly diagnosed breast cancer. Pre- and post-operative imaging’ comparison could be necessary to confirm complete removal of all cancer-associated micro-calcifications, with clinical judgment exercised regarding re-excision for close margins.
Also, it is important to exclude a multifocal and multicentric neoplasm as a contralateral breast cancer and MRI proves to be a thorough examination for this purpose. The contralateral prophylactic mastectomy is becoming increasingly, especially in categories at high risk with BRCA’s mutation. MRI increases Positive Predictive Value and specificity compared to mammography if there are suspected microcalcifications, as in our case; infact Breast MRI has the potential to improve the diagnosis of the category BI-RADS-4 microcalcifications and could alter indications for biopsy-procedure or conservative surgery [6].
Case report
In our case report we have used a combined test, mammography at first and MRI as second level, for the diagnostic strategy to identify the microcalcifications distribution on inferiorinternal quadrant (IIQ) of left side and to decide for a breast conserving therapy for this patient.
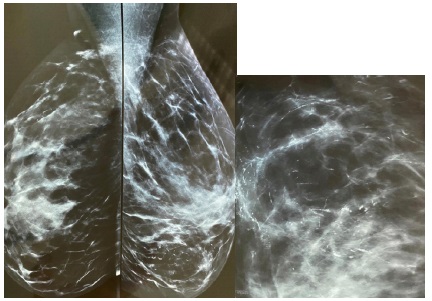
The patient (R.M.) underwent to a mammography exam in June 2000 in a private radiological office that reported: “On the IIQ of left side, pathological microcalcifications distributed at range about for 7 cms and in this context a nodule of 15 mms of heteroformative nature” (Figures 1)
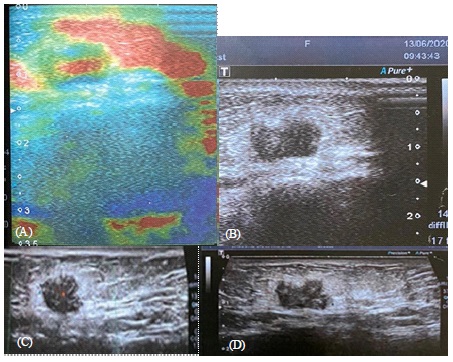
The radiologist performed a breast Ultrasound (US) exam too. (Figures 2a-d).
She did an ultrasound biopsy on the palpable-mass of 15 mms located at the inferior internal quadrant, near the parasternal margin, but the mammography showed an 7 cms extention of the suspected malignant microcalcification on the all IIQ left side without others information. The radiologist did not perform biopsy by stereotaxis of microcalcifications.
The micro-histological exam showed an invasive carcinoma G2, ER +100%, RPg – Mib-1 35-40%, Hercept test ASCO/CAP 2018 2+ or doubtful and the FISH-analysis was positive for amplified profile.
The patient underwent to a breast specialistic and oncologist, and they decided to insert the patient into the diagnostictherapeutic path for breast cancer in our hospital.
The patient performed MRI of the breast with contrast medium whereas she had not undergone to stereotactic biopsy on the micro-calcifications, before surgical and oncological decision in multidisciplinary consultation.
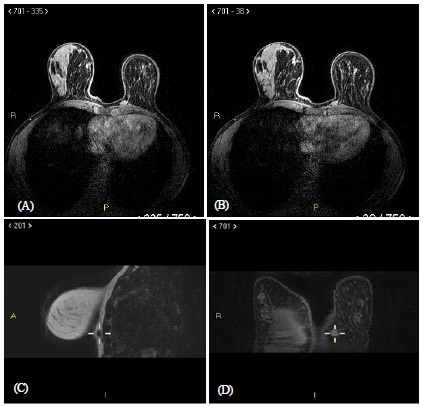
Breast MRI, compared with Mammography and breast US, had shown the presence in the inferior-internal quadrant (IIQ) of the left breast of suspected micro-calcifications (but not clearly malignant), that are scattered in an area of 7 cms; in this context, a 15 mms heteroformative nodule was identified. The breasts appeared with mixed structure and glandular prevalence, with an asymmetrical back-ground enhancement. In the left side, in the IIQ left side, in deep seat, a mass-like of 13 X 7 mms about, with uneven enhancement, with vascular pole on the lateral side and not definitely dissociable from the chest wall (BI RADS 5), was identified. In the superior-internal quadrant (SIQ), there is a focus of early enhancement of 5 mms, of longitudinal morphology which extends anteriorly into the periareolar area (BI RADS 4) (Figures 3a-d).
A CT scan of all body also showed no distant metastasis.
After multidisciplinary consultation, between breast-surgeon and oncologist and radiologist, because of the presence of the suspected microcalcifications BI-RADS 4 at mammography but not in MRI with c.m. and the typical BIRADS 5 nodule in the IIQ and the other BI-RADS 4 nodule to the superior internal quadrant of the same left side, a conservative approach was decided as oncoplastic surgery with a flap of rotation of second level and an accurate histopathology exam for the risk of local relapse in case of not close-margins was requested.
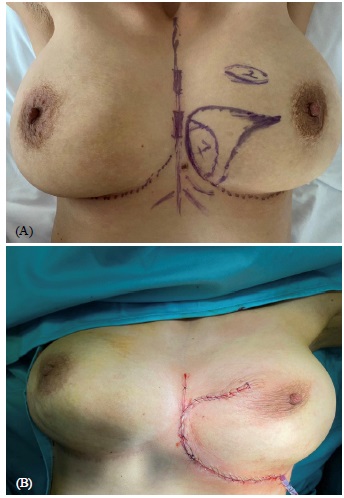
The surgical tactic (Figures 4a-b) was chosen after a detailed study and reconstruction-phases of the MRI reporting that allowed to carry out the pre-operative drawing and the safe choice of a conservative surgical procedure [7]. The removal of internal- inferior quadrant was made and also a separate excision for the other nodule without removing excess tissue. The malignant nodule was located in the IIQ near the parasternal position and infiltrating superficially the muscle tissue below, in the same context of a large cluster microcalcifications that were benign at the final histopathology exam.
The reconstruction was made with oncoplastic flap obtained through mobilitazion of the gland at the inframammary sulcus and at the intermammary sulcus. A total axillary lymphadenectomy was made. Two drainages were placed respectively in the breast bed and in the axillary region.
The post-operative results were good, the drainage on the breast was removed after 5 days and the one on the axillary region after 21 days, without sieroma or others later complications. A good scarring was encouraged by application of a special cream for scar and by monitoring every week the patients. The resection surgery of breast parenchyma of the lower-internal quadrant of the left breast, fixed in formalin, was submitted to Anatomical Pathology Laboratory [8,10] and subjected to macroscopic exam. It was about the size of 5, 5 X 5 X 4 cm with lozenge of the skin of 5 X 4 cm. Also the benign nodule at the superior internal quadrant was examined.
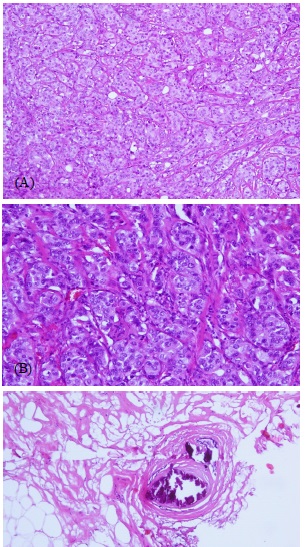
When cut the main quadrant, a firm neoplasm of withish colour, hard consistency and of maximum diameter 1,3 cm was found. It was 1 cm from the skin, 1,2 cm from inferior margin (marked with single long wire), 0,5 cm from parasternal margin (marked with double short wire) and 0,2 cm from deep margin (marked with ink). The skin was normconformed. The surrounding parenchyma looked adipose. The formalin-fixed paraffin-embedded tissue material was cut in 3–4 μm thick sections and deparaffinised. The sections were stained with hematoxylin-eosin. The material under examination consisted of a stellate invasive carcinoma into abundant fibrotic stroma with a solid, nonglandular architecture (tubule formation < 10%, score 3), high grade pleomorphic nuclei with prominent nucleoli (score 3) and mitotic count of five per 10 hpf 40x (score 1): It was a moderatly differentiated invasive duct carcinoma, histologic grade 2, score 7, based on criteria established by Elston and Ellis (Figures 5a-b).
Benign microcalcifications was found in the surrounding parenchyma, but not into the tumor. They were typically benign vascular calcifications, corresponding to calcium deposits in the walls of the mammary arteries. The primary composition of breast calcifications is hydroxyapatite, which will appear dark blue on hematoxylin and eosin stains (Figure 5c).
At least, she started a chemotherapy scheme with Adriamycin and Cyclophosphamide every 21 days for 4 cycles and then Taxol every week for 12 cycles with Herceptin every 3 weeks all the first year of oncological treatment; after pharmacological therapy, she might start a oncological follow-up, with the promise of a future contralateral surgical symmetrization procedure after this first treatment.
Discussion
Micro-calcifications are a common finding in mammography for breast screening and they usually require invasive procedures to diagnose or exclude malignancy, as sterotactic biopsy; but many microcalcifications are due to benign lesions and the correct indication for breast MRI might be an additional diagnostic tool used to distinguish benign from malignant mammographic microcalcifications in this setting of a complex breast carcinoma [11].
Sensitivity, specificity, positive and negative Predictive Values (PV) for breast MRI are almost higher to mammography or ultrasound exam.
MRI is useful in the Neoadjuvant Chemotherapy (NAC) treatment to allow Breast-Conserving Therapy (BCT) in patients who required mastectomy at presentation
Breast MRI is more accurate than mammography in assessing treatment response and these patients have less risk of Local-Regional Recurrence (LRR) undergoing breast-conserving surgery if preoperative MRI features including Breast Imaging Reporting and other profiles such as clinical-pathologic features (age, stage, tumor subtype, histologic grade, lymphovascular invasion and Hormonal receptor status) [12,13]. MRI can be useful in the surgical decision and to allow an oncoplastic conservative procedure instead of a conservative mastectomy or a demolytic breast procedure. The Local Regional Recurrence (LRR) is more frequently observed in the same quadrant as the original tumor in the down-staged BCT group than in the preplanned BCT patients as in this case. Breast MRI has the potential to improve the diagnosis of category-microcalcifications and could alter indications for biopsy. In fact, MRI can reliably exclude malignancy in suspicious microcalcifications. Microcalcifications can be detected by MRI in human whole breast specimens by the application of phase derivative imaging. Breast density and reasons for referral had no significant influence on the diagnostic performance of breast MRI [14,15].
The use of the breast MRI was optimal in our case for the microcalcifications’ locatization and their definition, especially because we did not have available the R.O.L.L. technique, that is usually a simple, safe and well-tolerated method by patients. In our case, R.O.L.L. was not indicated because of the not clearly malignant nature of microcalcifications [16], as MRI showed.
If we would like to compare the efficacy of a possible radioguided localization (R.O.L.L.) versus a pre-operative MRI localization in terms of clear margins, re-intervention rates, excess of resected breast tissue, and operative times, we could define that they are equally effective to excise microcalcifications with clear margins, providing similar re-intervention rates and resection volumes, especially in cases where MRI images of microcalcifications don’t seem clearly malignant [17].
Conclusion
Technical developments have improved the quality of breast MRI, allowing the acquisition of isotropic high-resolution images. In addition, multiparametric breast MRI has largely replaced the conventional approach, which was primarily based on conventional contrast-enhanced sequences alone for lesion classification.
Indications for breast MRI are now consolidating. MRI allows for improvement of surgical practice, reducing re-excisions while preventing unnecessary mastectomies. From an economic perspective, and to improve patient comfort, breast MRI can be optimized by adjusting the protocol with regard to the indication.
For indications where the exclusion of disease is most important, abbreviated protocols may be used. On the other hand, when lesions need to be characterized in detail, or when the frequency of findings is high, multiparametric protocols are mandatory.
MRI is a good detection method not only for a mass-lesion, but also for defining an architectural distortion, asymmetries and microcalcifications described in mammography.
MRI protocol for breast cancer offers improved time and workflow efficiencies and has the potential to increase the number of breast cancers detected, as occult carcinoma or multifocal cancer and it is a safe method to define surgical procedures for suspected microcalcifications and the detection of pathologically relevant invasive breast cancer at earlier stages.
MRI is superior to mammography not only in revealing the location, the shape, the border, internal structure of the mass and its chest-wall invasion, but also in revealing the axillary lymph nodes and the internal mammary lymph nodes and the mammary pluggers; MRI is an adequate method to determine the mass nature in displaying microcalcification as BIRADS-3 or BIRADS-4 micracalcifications.
The various actors involved in Breast Cancer management, as in our case that was discussed in a multidisciplinary evaluation, proposed an up-to-date diagnostic and interventional strategy, based on the predictive values and the BI-RADS classification of breast MRI in pre-operative setting for the microcalcifications that are usually highlighted in the first level exams or mammography as a safe and appropriate approach in outcomes and results for breast carcinoma
References
- Rominger M, Wisgickl C, Timmesfeld N. Breast microcalcifications as type descriptors to stratify risk of malignancy: A systematic review and meta-analysis of 10.665 cases with special focus on round/punctate microcalcifications. Rofo. 2012; 184:1144- 1152.
- DeMartini W, Lehman C. A review of current evidence-based clinical applications for breast magnetic resonance imaging. Magn Reson Imaging. 2008; 19: 143-150.
- Fischer U, Kopka L, Grabbe E. Breast carcinoma: effect of preoperative contrast-enhanced MR imaging on the therapeutic approach. Radiology. 1999; 213: 881-888.
- A Rao, J Feneis, C Lalonde, H Ojeda-Fournier. A Pictorial Review of Changes in the BI-RADS Fifth Edition. Radiographics. 2016; 36: 623-639.
- Barbara Bennani-Baiti, Pascal A Baltzer. MR Imaging for Diagnosis of Malignancy in Mammographic Microcalcifications: A Systematic Review and Meta-Analysis. Radiology. 2017; 283: 692- 701.
- A Luini et al: Preoperative localization and surgical approach in 344 cases of non-palpable breast lesions. Eur J Surg Oncol 1991; 17: 480-484.
- Bartlomiei Szynglarewicz, et al: Breast segmentectomy with rotation mammoplasty as an oncoplastic approach to extensive ductal carcinoma in situ. World J Surg Oncol. 2016; 14-72.
- Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. The value of histological grade in breast cancer: Experiences from a large study with long-term follow-up. Histopathology 1991; 19: 403-410.
- Arancibia PL, Taub T, López A,Díaz ML, Sáez C. Calcificaciones mamarias: Descripción y clasificación según la 5.a edición BIRADS Rev Chil Radiol. 2016; 22: 80-91.
- Bell BM, Gossweiler M. Benign Breast Calcifications. [Updated 2020 Aug 10]. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2021.
- Takayoshi Uematsu, Sachiko Yuen, Masako Kasami, Yoshihiro Uchida. Dynamic contrast-enhanced MR imaging in screening detected microcalcification lesions of the breast: Is there any value?. Breast Cancer Research and Treatment. 2007; 103: 269– 281.
- Hlawatsch A, Teifke A, Schmidt M, Thelen M. Preoperative assessment of breast cancer: sonography vs MR imaging. AJR Am J Roentgenol. 2002; 179: 1493-501.
- Hata T, Takahashi H, Watanabe K, et al. Magnetic resonance imaging for preoperative valuation of breast cancer: A comparative study with mammography and ultrasonography. I Am Coll Surg 2004; 199: 173-174.
- Eun NL, Son EJ, Gweon HM, Youk JH, Kim JA. The value of breast MRI for BI-RADS category 4B mammographic microcalcification: based on the 5th edition of BI-RADS. Clin Radiol. 2018; 73: 750- 755.
- Benjam K Y Chan,Jill A Wiseberg–Firtell, Ramesh H S Jois, Katrin Jensen, Riccardo A Audisio. Localization techniques for guided surgical excision of non-palpable breast lesions. Cochrane Database Syst Rev. 2015.
- Masahiro Sakakibara et al: MRI-guided quadrantectomy in patients with ductal carcinoma in situ detected preoperatively by mammographic calcifications. J Am Coll Surg. 2014; 2019: 295- 302.
- Akiko Shimauchi et al: Breast MRI as a Problem-solving Study in the Evaluation of BI-RADS Categories 3 and 4 Microcalcifications: Is it Worth Performing? Acad Radiol. 2018; 25: 288-296.