
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An unusual presentation of bradycardia, acidosis, and right ventricular dysfunction after left ventricular assist device implantation: A case report
Jennifer M Elia1*; Karen H Katrivesis1; Ali A Naqvi2; Fabio M Sagebin3; Dawn M Lombardo2; Kei Togashi1
1 Department of Anesthesiology and Perioperative Care, Division of Anesthesia Critical Care Medicine, University of California, Irvine, USA.
2 Department of Medicine, Division of Advanced Heart Failure Cardiology, University of California, Irvine, USA.
3 Department of Surgery, Division of Cardiothoracic Surgery, University of California, Irvine, USA.
*Corresponding Author : Jennifer M Elia
Department of Anesthesiology and Perioperative Care,
Division of Anesthesia Critical Care Medicine, University of California, 101 The City Dr. South, Building 53,
Orange, CA 92868, USA.
Email: jelia@hs.uci.edu
Received : Apr 23, 2021
Accepted : May 28, 2021
Published : Jun 02, 2021
Archived : www.jcimcr.org
Copyright : © Elia JM (2021).
Abstract
Right Ventricular (RV) dysfunction is a common complication seen in 20-50% of patients after Left-Ventricular Assist Device (LVAD) implantation. Although prediction models exist, it is challenging to prevent RV dysfunction and even more difficult to manage. Early recognition is crucial to determine the appropriate pharmacological therapies and decide if implementation of Mechanical Circulatory Support (MCS) is needed. Here, we present a case of RV dysfunction precipitated unexpectedly by a bradycardic episode. The RV dysfunction was refractory to traditional therapies but was successfully managed with right-sided MCS.
Abbreviations: ALV: Left Ventricle/Ventricular; RV: Right Ventricle/ Ventricular; LVD: Left Ventricular Assist Device; RVAD: Right Ventricular Assist Device; MCS: Mechanical Circulatory Support; TEE: Transesophageal Echocardiography; Rpm: Revolutions Per Minute; Svo2 : Mixed Venous Oxygen Saturation; CO2 : Carbon Dioxide; Pao2 : Arterial Partial Pressure Of Oxygen; CPB: Cardiopulmonary Bypass.
Citation: Elia JM, Katrivesis KH, Naqvi AA, Sagebin FM, Lombardo DM, et al. An unusual presentation of bradycardia, acidosis, and right ventricular dysfunction after left ventricular assist device implantation: A case report. J Clin Images Med Case Rep. 2021; 2(3): 1176.
Introduction
The use of Left Ventricular Assist Devices (LVAD) has become increasingly common as more patients are diagnosed with advanced heart failure. The success of these devices and progression of technology have made them promising modalities to prolong life as destination therapy, or to bridge patients to heart transplantation or possibly cardiac recovery. The postoperative care of these patients presents several challenges, with numerous complications that may potentially arise. One of the most serious is Right Ventricular (RV) failure, which occurs in 20-50% of LVAD patients, and leads to a longer hospital course and increased mortality [1]. There are several tools used to predict post-implantation RV failure, but none are highly sensitive and all patients respond differently to LVAD insertion [2]. Additionally, most patients who need LVAD support will have some degree of baseline RV dysfunction due to advanced LV failure.
We present a patient who underwent uneventful LVAD implantation but suffered an unexpected bradycardic episode six hours after surgery. This event initiated progressive deterioration in the patient’s course, ultimately resulting in severe RV failure that required right-sided Mechanical Circulatory Support (MCS).
The patient and family have provided written HIPAA authorization for the authors to evaluate his case and publish relevant data. This manuscript adheres to the Enhancing the Quality and Transparency of Health Research (EQUATOR) guidelines.
Case description
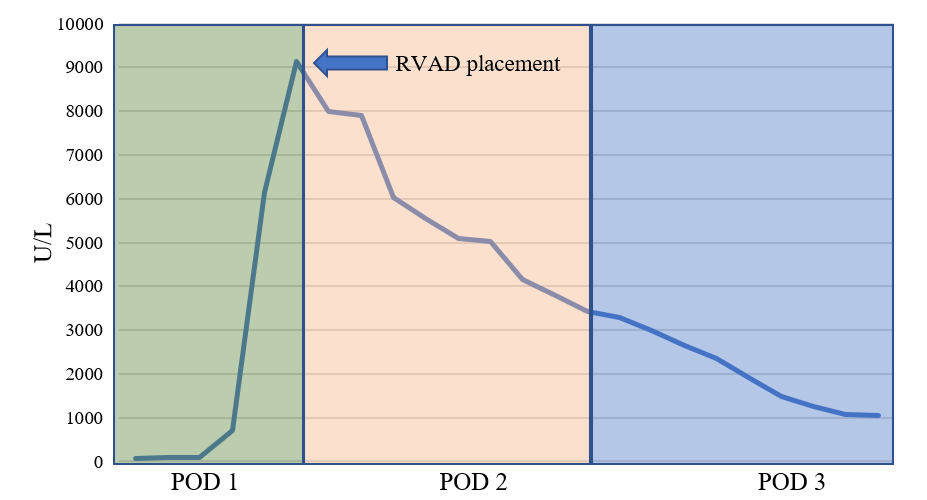
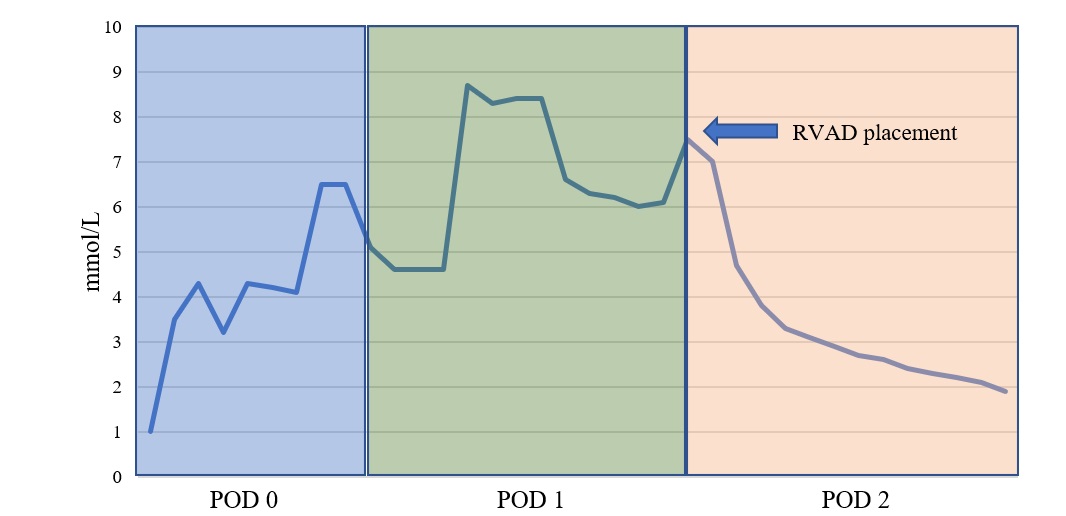
A 59-year-old-male with new-onset nonischemic cardiomyopathy presented in cardiogenic shock, and was determined to be eligible for Left-Ventricular Assist Device (LVAD) implantation after acute management with inotropic agents and temporary left-sided mechanical circulatory support. Pre-operative transthoracic echocardiography imaging revealed his RV function to be mild to moderately reduced. Additionally, he was treated for atrial flutter with amiodarone at standard dosing for six weeks prior to surgery without successful chemical conversion. The patient underwent HeartMate III (Abbott, Illinois) implantation via open sternotomy approach. Right Ventricular (RV) function was normal in the operating room post-implantation and he spontaneously converted to normal sinus rhythm after separation from cardiopulmonary bypass. Six hours following surgery, the patient’s mixed-venous oxygen saturation (SvO2 ) decreased from 77% to 52%, fever developed, and mean arterial pressure declined, necessitating upward titration of his vasoactive infusions. Transesophageal echocardiography (TEE) revealed a dilated Left Ventricle (LV) with normal RV function, so LVAD speed was increased to 5800 rpm from 5200 rpm with mild improvement in his hemodynamics. Subsequently, the patient developed sinus bradycardia with heart rates between 30-40 bpm with further decline in his hemodynamics, necessitating transvenous cardiac pacing. The patient experienced continued hemodynamic deterioration resulting in worsening SvO2 to 12%, followed by profound end-organ damage including severe transaminitis (AST 9,128 U/L, ALT >5,000 U/L; Figure 1) and lactic acidosis (8.7 mmol/L; Figure 2).
He was intubated, sedated and required high-dose inotropes and vasopressors to maintain hemodynamic stability. Neuromuscular blockade was used for paralysis to avoid patientventilator dissociation and thus increased oxygen consumption. Despite these efforts, end-organ malperfusion worsened and acidosis ensued, requiring continuous renal replacement therapy. Escalating doses of vasoactive infusions were necessary to maintain adequate perfusion. Given the deterioration of his clinical picture and progression of RV dysfunction (Supplemental Digital Content, Video 1), the decision was made to initiate right-sided MCS.
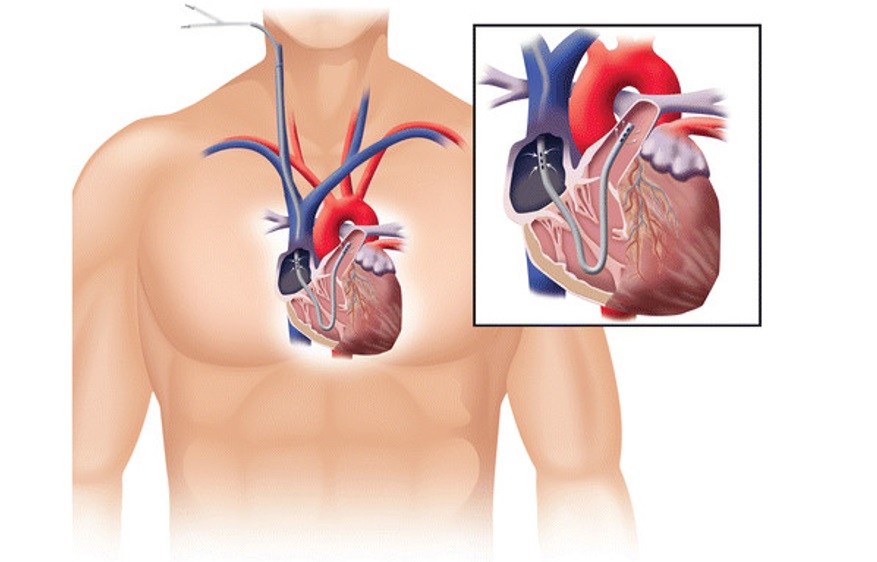
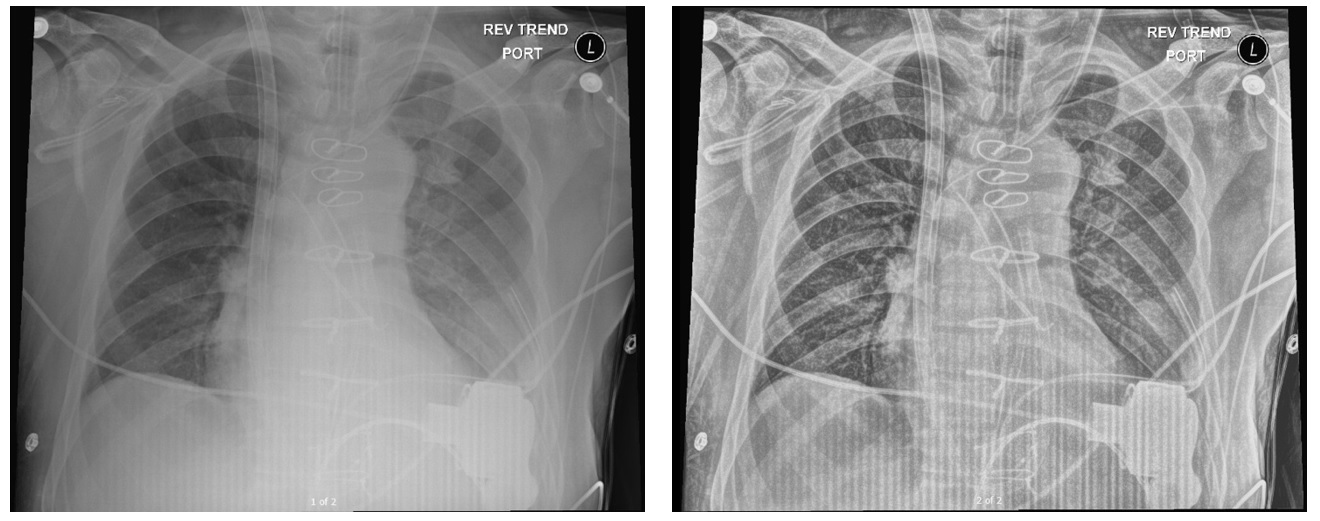
A ProTek Duo cannula was inserted through the right internal jugular vein and connected to a CentriMag (Abbott, Pleasanton, CA) pump with initial flows at 4.4L/min (Figure 3 A,B). In the subsequent 24 hours, improvements were seen in liver function (Figure 1), lactate (Figure 2), and SvO2 . The patient was rapidly weaned to minimal vasopressor and inotropic support.
After a gradual wean under echo guidance, and with inotropic support of milrinone and epinephrine, he was able to be removed from Right Ventricular Assist Device (RVAD) support on post-operative day 21. He was discharged home three weeks later without the need for long-term dialysis.
Rising level of AST values (U/L, reference range 13 – 39 U/L) leading up to right ventricular assist device (RVAD) placement, after which values slowly decline over next several days. ALT levels also followed a similar pattern.
Lactate trend (reference 0.5 – 2 mmol/L) with peak on Post-Operative Day (POD) 1 at 8.7 mmol/L and progressive decline and normalization after right ventricular assist device (RVAD) placement early POD 2.
A. Illustration of the ProTek Duo Cannula and proper placement with inflow portion in the right atrium and outflow in the main pulmonary artery *J Cardiothorac Surg. 2016; doi:10.1186/s13019-016-0515-y
B. Portable chest radiographs depicting successful placement of the ProTek Duo Cannula with insertion in the right internal jugular vein.
Discussion
RV failure is unfortunately rather common after LVAD implantation, occurring in up to 20-50% of cases. Patients with non-ischemic heart failure, such as our patient, have a significantly higher incidence than those with ischemic heart failure [1]. Several structural mechanisms can explain the etiology of RV dysfunction seen after LVAD implantation. Leftward shift of the intraventricular septum associated with improved LV emptying can result in poor RV contraction [3,4]. Additionally, increased venous return from the improved cardiac output, as well as volume resuscitation in the perioperative period, can overload an already stressed RV [3].
Some of the dimensions evaluated to predict RV failure include Tricuspid Annular Plane Systolic Excursion (TAPSE), RV short/long axis ratio, tissue doppler derived tricuspid lateral annular systolic velocity (S’), and RV-to-LV end-diastolic diameter ratio (Table 1) [2,5,6]. Invasive measurements from right heart catheterization can also be utilized as predictors such as Pulmonary Artery Pulsatility index (PAPi) and RV Stroke Work Index (RVSWI) [7]. Unfortunately, no measure has both high specificity and sensitivity, necessitating the use of multiple dimensions for clinical decision making. Post-operatively, monitoring of right heart function is achieved by frequent hemodynamic assessments of central venous pressure, pulmonary artery pressure, cardiac index, and SvO2 as well as laboratory parameters and frequent echocardiography if warranted.
Table 1: Echocardiography parameters used to assess RV dysfunction |
|
Measurement |
Abnormal value |
TAPSE |
< 1.6 cm |
RV short/long axis ratio |
> 0.6 |
RV-to-LV EDD ratio |
> 0.72 |
S’a |
< 10 cm/s |
Abbreviation: TAPSE: tricuspid annular plane systolic excursion; RV: right ventricle; LV: left ventricle; EDD: end-diastolic diameter |
|
Bradycardia is an uncommon cause of RV failure after LVAD implantation. However, in a patient with long-standing atrial flutter or post-cardiac surgery, sinus node dysfunction can occur [8]. In this case, although the patient spontaneously converted to sinus rhythm after separation from cardiopulmonary bypass, it is possible that a systemic inflammatory response unmasked sinus node dysfunction and caused sustained bradycardia. In a hypermetabolic state, such as in this post-surgical patient, bradycardia was especially detrimental resulting in severe end-organ malperfusion and low SvO2 . We suspect the patient suffered RV dysfunction secondary to ongoing cardiac malperfusion and altered right-sided mechanics. Use of amiodarone pre-operatively may have also contributed to the development of bradycardia, but we could not be certain if this was ultimately the culprit.
Medical management for RV failure is centered on optimizing RV contractility and reducing RV volume overload with the use of pulmonary vasodilators, inotropes, and diuresis. If RV dysfunction is refractory to medical management, MCS may be indicated [9]. The devices available for percutaneous RV support include Impella RP (Abiomed, Massachusetts), ProTek Duo (TandemLife, Pittsburg) cannula connected to a centrifugal pump (also known as RVAD), or Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO). Compared to the Impella RP, the ProTek Duo allows for more mobility due to its insertion site in the internal jugular vein compared to the femoral vein. Additionally, an oxygenator may be spliced into the RVAD circuit in a configuration referred to as oxy-RVAD [9]. Both devices are typically placed in the catheterization lab under fluoroscopic and TEE guidance. In our experience, optimal positioning of the Impella RP catheter can be difficult due to its “S” shaped curvature, further complicating care if the device becomes malpositioned in the ICU. Additionally, femoral access for the Impella RP limits patient mobility. There is no evidence to date that compares outcomes between these percutaneous methods for RV support in the post-LVAD population. Also, the optimal timing of temporary right-sided MCS in post-LVAD patients is unclear [9,10]. In this case, the RVAD was inserted before the development of severe RV failure to pre-emptively support a tenuous RV with little reserve and improve end-organ perfusion.
This patient had an unexpected presentation of bradycardiainduced RV failure post-LVAD implantation which led to severe multi-organ failure. Although this presentation is uncommon, early recognition of RV dysfunction from any cause is paramount to appropriately manage this complex process and consideration of MCS may be warranted.
Acknowledgements: We acknowledge the Springer Nature publishing group of the Journal of Cardiothoracic Surgery for allowing us to use an illustration from an open access article (Figure 3A).
References
- Løgstrup BB, Nemec P, Schoenrath F, et al. Heart failure etiology and risk of right heart failure in adult left ventricular assist device support: The European Registry for Patients with Mechanical Circulatory Support (EUROMACS). Scand Cardiovasc J. 2020; 1-9.
- Paluszkiewicz L, Börgermann J. The value of echocardiographic examination in predicting right ventricular heart failure in patients after the implantation of continuous-flow left ventricular assist devices. Interact Cardiovasc Thorac Surg. 2018; 27: 931- 937.
- Lampert BC, Teuteberg JJ. Right ventricular failure after left ventricular assist devices. J Heart Lung Transplant. 2015; 34: 1123- 1130.
- Santamore WP, Gray LA Jr. Left ventricular contributions to right ventricular systolic function during LVAD support. Ann Thorac Surg. 1996; 61: 350-356.
- Meluzín J, Spinarová L, Bakala J, et al. Pulsed Doppler tissue imaging of the velocity of tricuspid annular systolic motion; a new, rapid, and non-invasive method of evaluating right ventricular systolic function. Eur Heart J. 2001; 22: 340-348.
- Kapur NK, Esposito ML, Bader Y, et al. Mechanical Circulatory Support Devices for Acute Right Ventricular Failure. Circulation. 2017; 136: 314-326.
- Kang G, Ha R, Banerjee D. Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation. J Heart Lung Transplant. 2016; 35: 67-73.
- Peretto G, Durante A, Limite LR, Cianflone D. Postoperative arrhythmias after cardiac surgery: Incidence, risk factors, and therapeutic management. Cardiol Res Pract. 2014; 2014: 615987.
- Kormos RL. The right heart failure dilemma in the era of left ventricular assist devices. J Heart Lung Transplant. 2014; 33: 134- 135.
- Takeda K, Naka Y, Yang JA, et al. Timing of temporary right ventricular assist device insertion for severe right heart failure after left ventricular assist device implantation. ASAIO J. 2013; 59: 564-569.
- Kazui T, Tran PL, Echeverria A, et al. Minimally invasive approach for percutaneous CentriMag right ventricular assist device support using a single PROTEKDuo Cannula. J Cardiothorac Surg. 2016; 11: 123.
- Aaronson KD, Silvestry SC, Maltais S, et al. Patients Awaiting Heart Transplantation on HVAD Support for Greater Than 2 Years. ASAIO J. 2016; 62: 384-389.