
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Brigatinib treatment for primary lung lesions in non-small-cell lung cancer based on ALK gene rearrangement detected in resected brain metastases: A case report and literature review
Sumin Geng
Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Dongcheng District, Beijing, China.
*Corresponding Author: Sumin Geng
Department of Neurosurgery, Beijing Tiantan Hospital,
Capital Medical University, Dongcheng District, Beijing,
China.
Email: sumingeng@126.com
Received : Apr 26, 2021
Accepted : May 28, 2021
Published : Jun 02, 2021
Archived : www.jcimcr.org
Copyright : © Geng S (2021).
Abstract
Background: Lung cancer is the main cause of brain metastasis, primary lesions in patients with brain metastases from lung cancer are most often treated with surgery, and adjuvant chemoradiotherapy and other therapeutic methods are used to control disease progression based on the characteristics of the primary lesions.
Materials and methods: Here, we report a case of a patient with NSCLC who received brigatinib treatment for the primary lung lesions after the resection of brain metastases based on the ALK gene rearrangement detected in the resected brain metastases by highthroughput sequencing.
Results: The result of ten months follow-up showed satisfactory curative effect. The primary lung lesions disappeared and no sign of recurrence in the brain and lung
Conclusion: This method provides a new option for the treatment of primary lung lesions in patients with brain metastases from lung cancer
Keywords: NSCLC; Brain metastasis; ALK gene rearrangement; Brigatinib.
Citation: Geng S. Brigatinib treatment for primary lung lesions in non-small-cell lung cancer based on ALK gene rearrangement detected in resected brain metastases: A case report and literature review. J Clin Images Med Case Rep. 2021; 2(3): 1178.
Introduction
Brain metastasis occurs in approximately 20% of patients with metastatic cancers, especially lung cancer, breast cancer, kidney cancer, and malignant melanoma [1-3]. Lung cancer is the most common cause of brain metastasis, and Non-SmallCell Lung Cancer (NSCLC) with Epidermal Growth Factor Receptor (EGFR) or Anaplastic Lymphoma Kinase (ALK) gene alterations is most likely to result in brain metastasis [1,4,3]. Cancer patients with brain metastases often have poor prognosis. Brain metastases from lung cancer may develop if the disease further progresses after systematic treatment of lung cancer or may have central nervous system symptoms as the first symptoms, and pathological diagnosis can be used to confirm the presence of brain metastases from lung cancer. Currently, brain metastases in lung cancer patients are treated by comprehensive methods, such as surgery, radiotherapy, chemotherapy, targeted therapy, and immunotherapy, to prolong survival and improve quality of life. A large number of studies have confirmed the safety and efficacy of brigatinib treatment for the primary lung lesions and metastases in patients with ALK alteration-related NSCLC based on the ALK gene rearrangement detected in the primary lung lesions [5-8,4]. However, there are no reports regarding the treatment of primary lung lesions with brigatinib based on the characteristics of brain metastases.
Case report
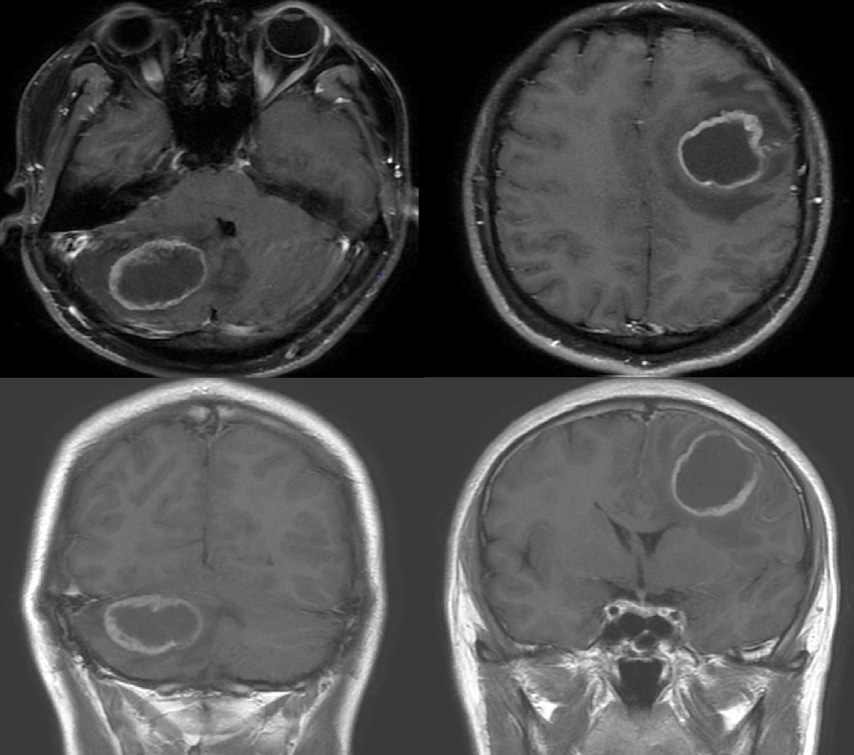
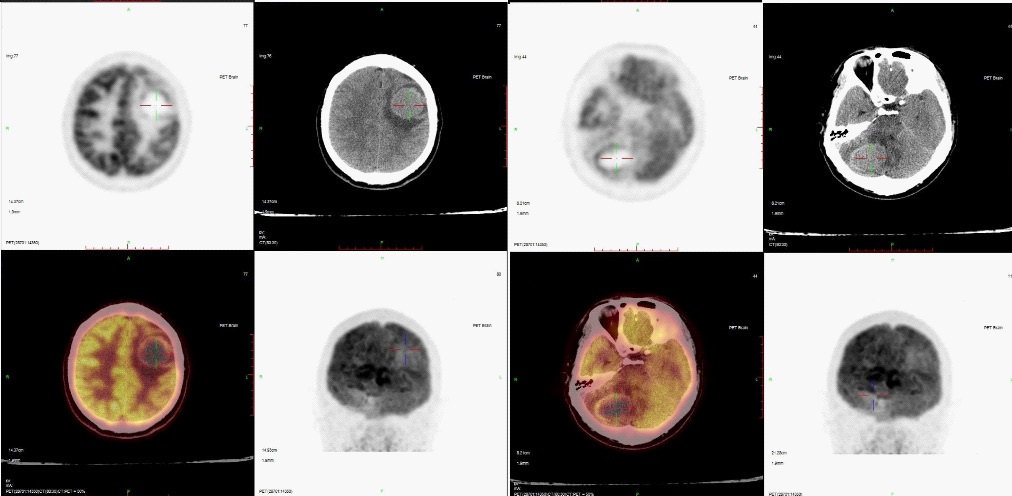
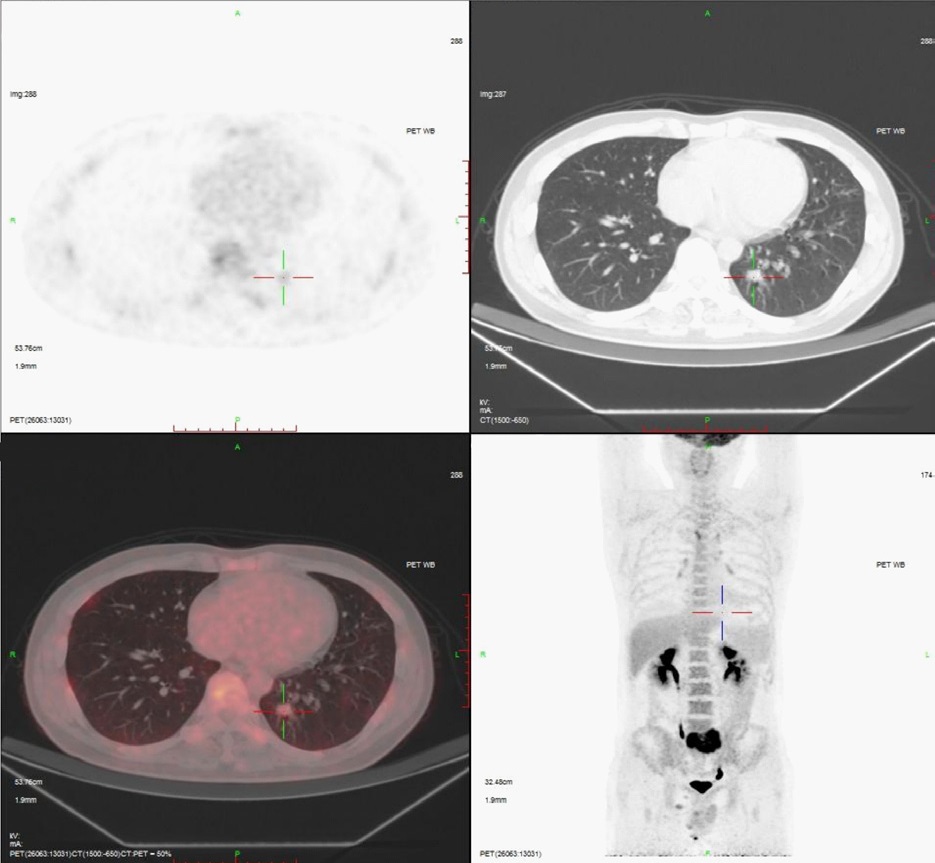
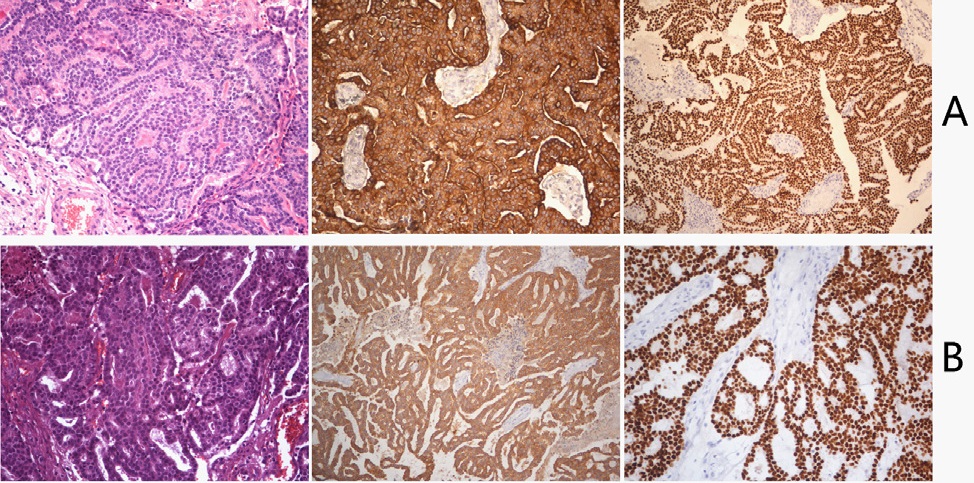
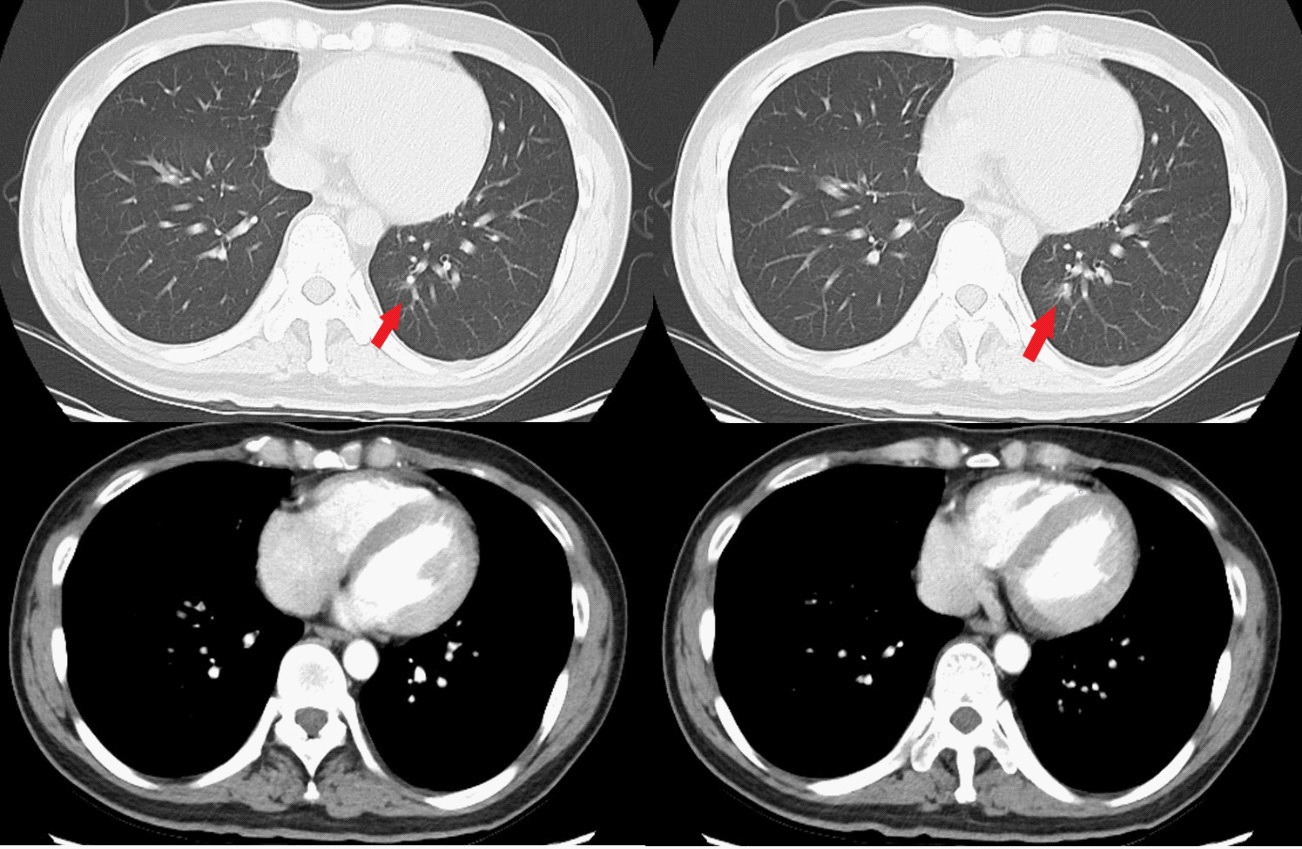
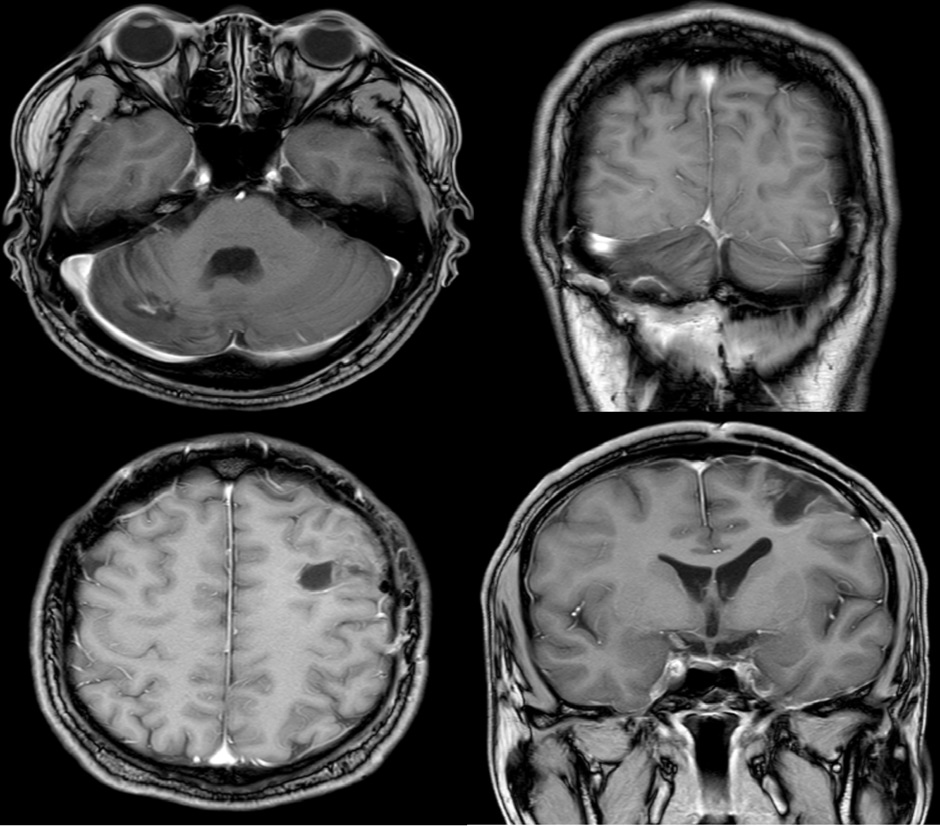
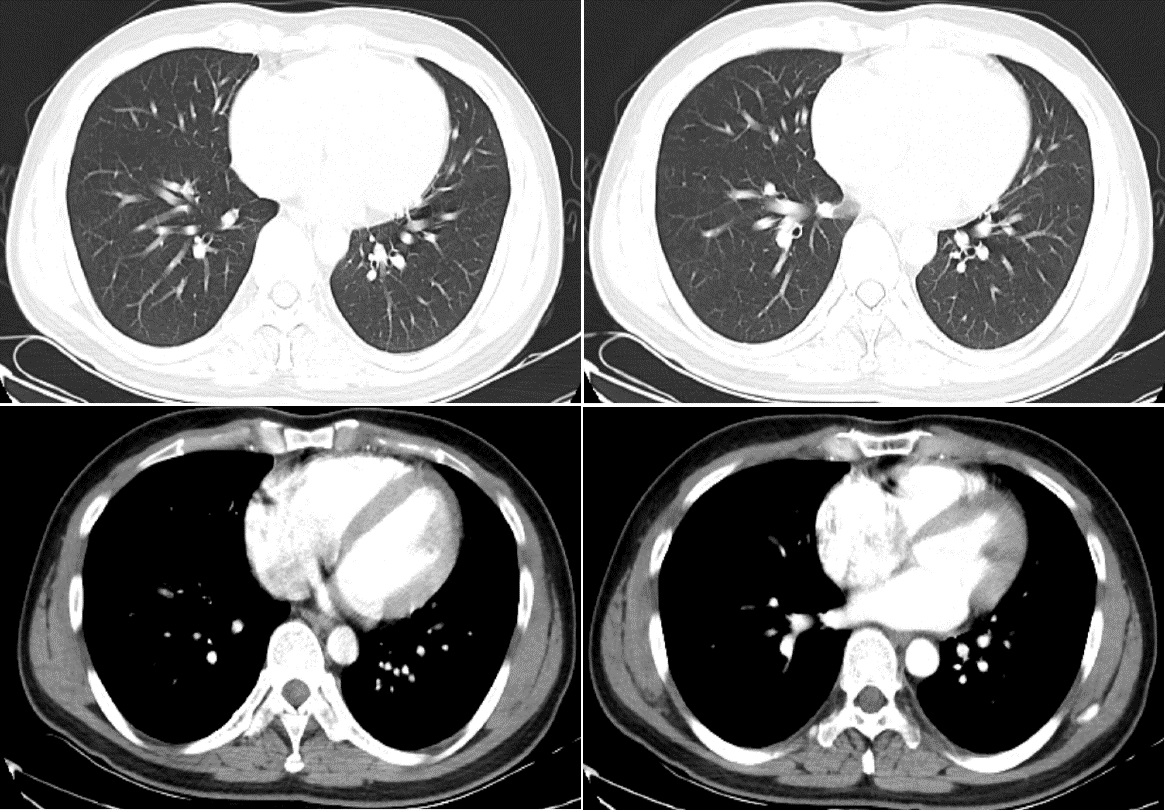
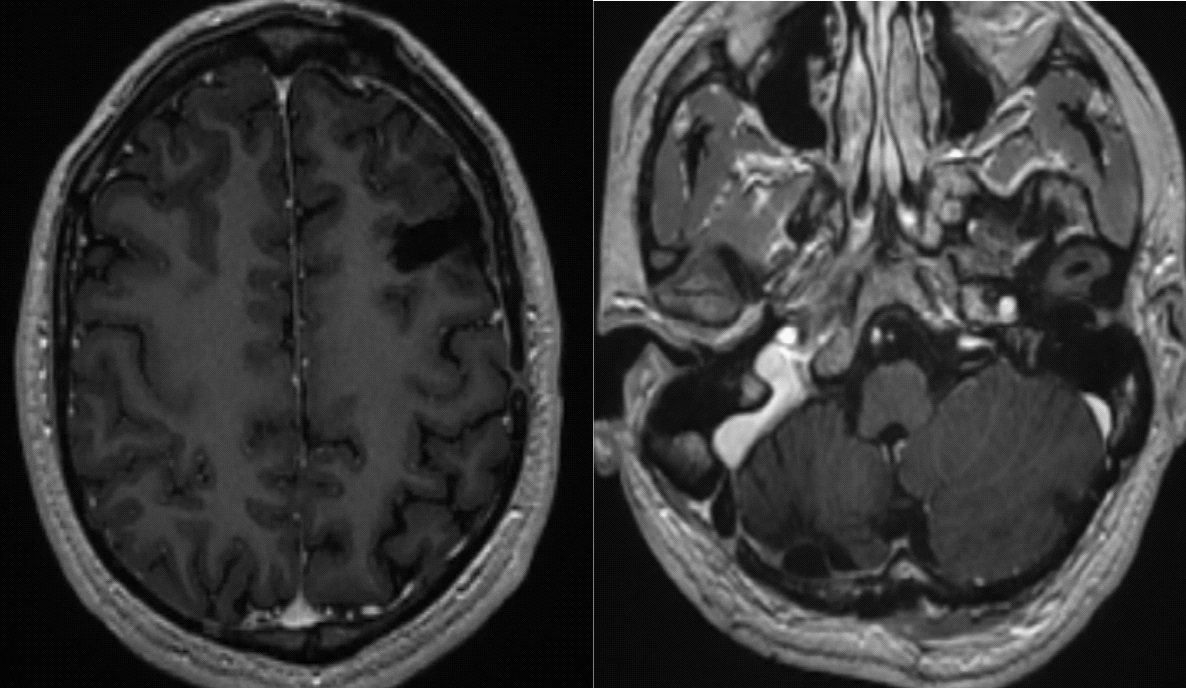
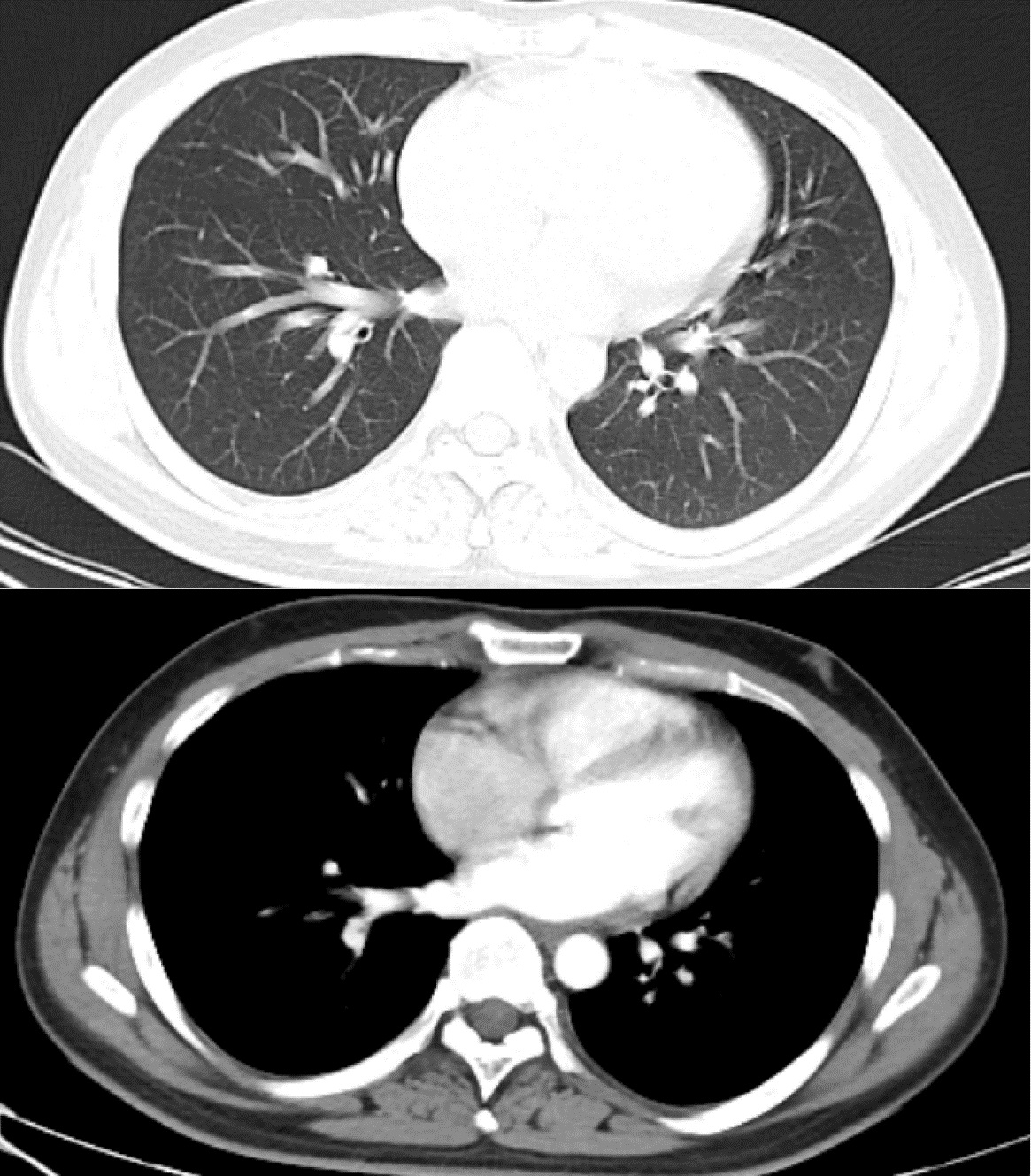
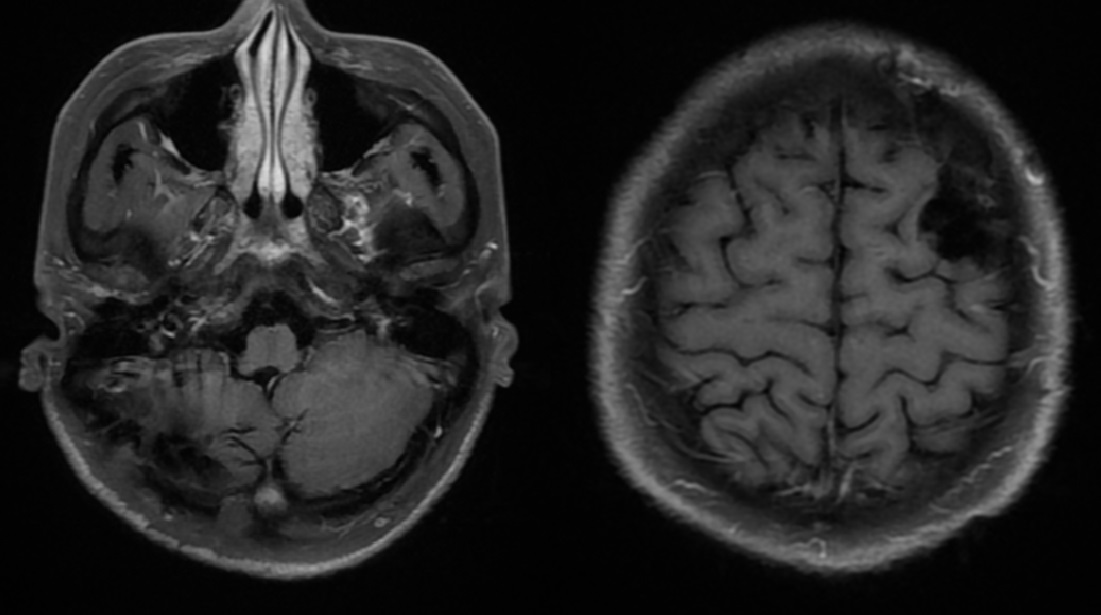
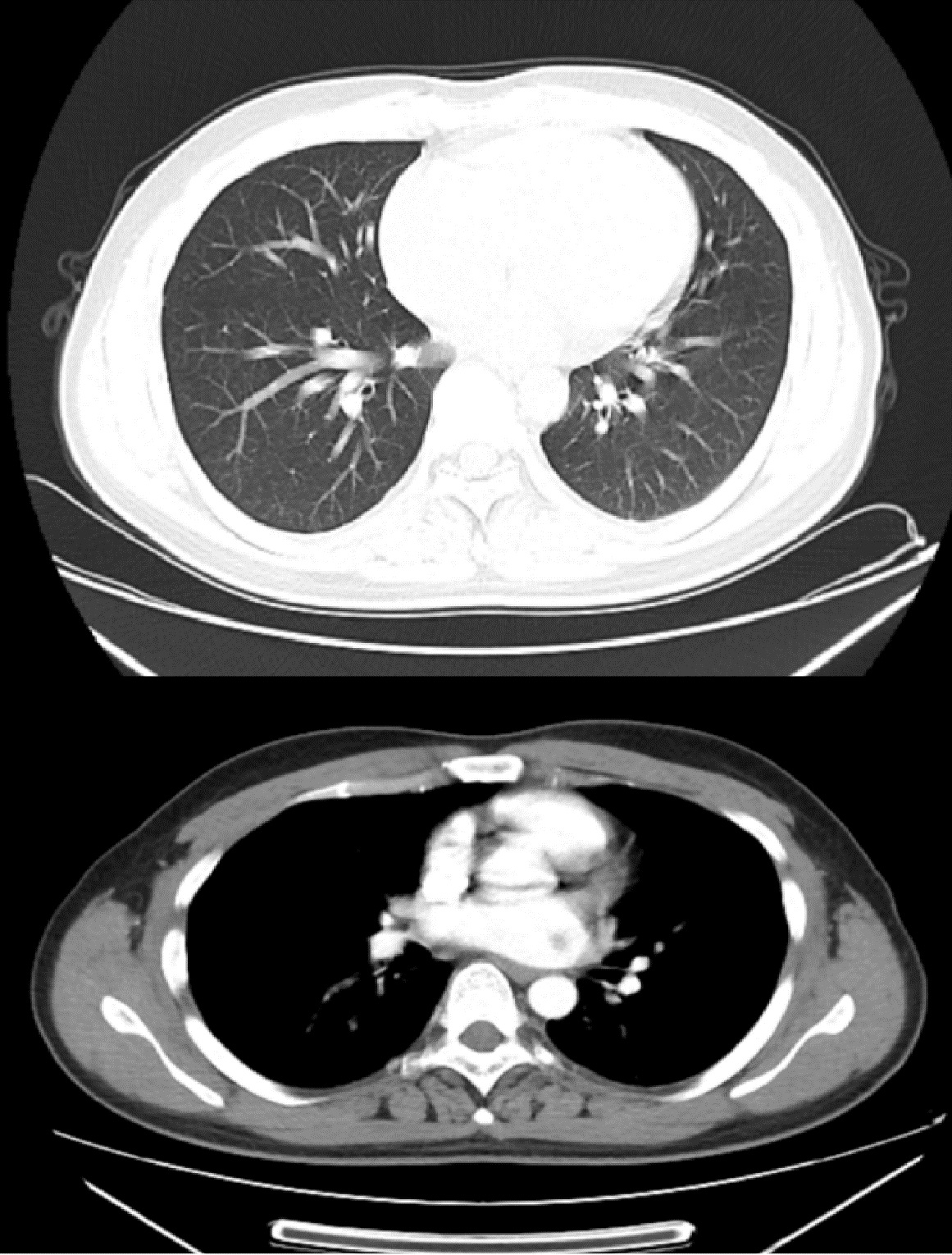
A 29-year-old male patient sought treatment due to headache and vomiting for one month. He underwent cranial Magnetic Resonance Imaging (MRI) examination. The results revealed occupying lesions in the left frontal lobe and the right cerebellum, which were suspected to be metastases (Figure 1). To further confirm the diagnosis, this patient underwent Positron Emission Tomography (PET)-Computed Tomography (CT) examination. The PET-CT results revealed a slightly hypermetabolic lesion (1.3 X 1.2 cm) in the posterior basal segment of the left lower lobe. Therefore, the patient was suspected to have peripheral lung cancer with mediastinal and bilateral hilar multiple lymph node metastases and bilateral lower cervical lymph node metastases. The hypermetabolic mass-like lesions in the left frontal lobe (4.1 X 3.6 cm) and right cerebellum (4.6 X 3.3 cm) were initially considered metastatic tumors (Figure 2). The patient underwent craniotomy for the resection of the lesion in the left frontal lobe due to intracranial hypertension. The postoperative pathology suggested adenocarcinoma of pulmonary origin, and immunohistochemistry showed positive Thyroid Transcription Factor-1 (TTF-1) expression. One week later, the patient underwent craniotomy again to remove the metastases in the right cerebellum. Postoperative pathology suggested adenocarcinoma of pulmonary origin, and immunohistochemistry also indicated adenocarcinoma of pulmonary origin with positive TTF-1 expression (Figure 3). Meanwhile, the tissue samples of the metastases removed from the right cerebellum were subjected to high-throughput sequencing to sequence the 830- gene panel and analyze the rearrangement of 44 genes and the copy numbers of 88 genes. Missense mutations in the FAT3, GRIN2A, and PTPRB genes and EML4-ALK gene rearrangement were detected in these samples, and no copy number variation was detected. The pathology results and high-throughput sequencing results suggested that the patient had brain metastases from lung cancer and ALK gene rearrangement and thus might benefit from ALK inhibitor therapy. The patients refused to receive further surgical treatment of primary lung lesions. After discharge, he received treatment with the ALK inhibitor brigatinib. At the one-month follow-up visit, chest CT examination indicated that the occupying lesion of the lung was significantly reduced (Figure 4). Therefore, the patient continued with oral brigatinib. At the four-month follow-up visit, the lung CT and cranial MRI examinations did not detect any lung lesions and indicated a stable brain condition without lesion recurrence (Figure 5). At the ten-month follow-up visit, the lung CT and cranial MRI examinations also indicated stable condition in both brain and lung (Figure 6). At the eighteen-month follow-up visit, the lung CT and cranial MRI examinations still indicated stable condition in both brain and lung (Figure 7).
Discussion
Regarding the treatment of brain metastases from lung cancer, the National Comprehensive Cancer Network (NCCN) guidelines (version 3.2020 NSCLC) currently recommend segmentectomy for primary lung lesions under 2 cm and targeted treatment based on the results of molecular detection of resected tumor tissue for metastases. The first-line drugs recommended for metastases from ALK-rearranged NSCLC include alectinib, brigatinib, and ceritinib. Stereotactic Radiotherapy (SRT) is recommended for limited brain metastases, and surgical treatment with postoperative adjuvant SRT or Whole-Brain Radiotherapy (WBRT) is recommended for symptomatic limited brain metastases. The NCCN guidelines (version 1.2020 CNSC) also recommend that for limited brain metastases of unknown origin, systemic examination should be completed, and surgical resection of lesions should be performed to determine the nature of the mass, relieve the mass effect, and alleviate brain symptoms. Many recent studies also consider that the joint use of multiple methods, such as surgery, radiotherapy, and chemotherapy, can relieve symptoms, prolong survival, and improve life quality. In the treatment of brain metastases, surgical treatment with adjuvant radiochemotherapy is recommended for oligometastases or cases of three or fewer lesions that can be easily removed by surgery. For patients who cannot tolerate surgery due to poor physical condition, SRT, or WBRT can be considered. For patients with multiple brain metastases or contraindications for surgery, WBRT is the first choice, and SRT with adjuvant chemotherapy may be suitable in some cases [9-11,3]. Because some patients are at risk due to intracranial hypertension, the treatment order is important. Most scholars believe that the intracranial occupying lesions should be resected before the treatment of primary lesions based on the systemic conditions[1,10]. In this study, the patient had severe intracranial hypertension. Therefore, based on the guidelines and the recommendations of most researchers and scholars, we first resected the metastases in his left frontal lobe and right cerebellum by craniotomies to alleviaten the intracranial hypertension.
The patient first underwent surgical treatment so that pathological tissue could be obtained for pathological examinations and high-throughput sequencing. The relevant results confirmed that the patient’s brain lesions were metastatic lesions of lung origin and had characteristics of ALK gene rearrangement. Past studies have shown heterogeneity between primary tumors and brain metastases and that the branched evolution of primary tumors and brain metastases may generate different types of mutant genes [2]. However, the concordance between the primary lesions and the metastases was high (>80%) for the mutation of major drivers, such as EGFR, KRAS, TP53, and ALK[12]. Some scholars studied the ALK-related molecules in primary lung lesions and the corresponding brain metastases, and their results support the high concordance of ALK status between primary lesions and metastases [13,14]. Therefore, we inferred that ALK gene rearrangement occurred in both primary lung lesions and brain metastases in this patient and that ALK inhibitors might achieve satisfactory therapeutic efficacy for both primary lung lesions and brain metastases in this patient. The above studies provide a theoretical basis for the treatment of primary lung lesions with ALK inhibitors based on ALK gene rearrangements detected in brain metastases. Since the FDA’s approval of the use of a first-generation ALK inhibitor, crizotinib, in clinical practice, the treatment of NSCLC patients has been greatly improved [15,16]. It has been reported that NSCLC patients may develop resistance to crizotinib after taking it for a period of time, and brigatinib, a second-generation ALK inhibitor, is superior to crizotinib in terms of efficacy [8]. In addition, brigatinib penetrates the blood-brain barrier more easily than crizotinib. Therefore, we speculated that brigatinib can not only control primary lung lesions but also improve the treatment effect for brain conditions. Since the patient refused to receive further surgical treatment of primary lung lesions, we treated the patient with the ALK inhibitor brigatinib based on the aforementioned theoretical basis and relevant studies. The follow-up results indicated a satisfactory therapeutic effect.
Previous studies on brain metastases from NSCLC mostly used surgically removed primary lung lesions to detect gene mutations, and the patients received maintenance treatment based on the detection results. The NCCN guidelines also recommend drug treatment based on molecular detection results from lung tumor lesions to control systemic metastases. However, the treatment of primary lung lesions based on ALK gene rearrangement detected in brain metastases has not been reported. From the reported successful case of brigatinib treatment for primary lung lesions in NSCLC based on ALK gene rearrangement detected in resected brain metastases, we can see that for patients with stable primary lung lesions and high-risk brain metastases, brain metastases can be resected first, and then targeted treatment of primary lung lesions can be planned based on the results detected in the tumor tissue samples from the resected brain metastases. This method can prevent further surgical trauma and is thus more acceptable to patients. This study has some limitations. First, only one patient was successfully treated using the proposed method, and the patient was followed up for eighteen months. Studies with a larger sample size and longer follow-up period are needed to verify the effectiveness of this treatment method and determine whether long-term stable control can be achieved. Second, the results will be more convincing if the tumor markers, circulating tumor cells, and circulating tumor DNA in blood can be dynamically monitored.
Conclusion
We reported the case of a patient with NSCLC who received oral brigatinib, an ALK inhibitor, to treat primary lung lesions after the resection of brain metastases based on ALK gene rearrangement detected in the resected brain metastases. This study provides clinical evidence for exploring new ideas and methods for the treatment of patients with brain metastases from lung cancer
References
- Achrol AS, Rennert RC, Anders C et al. Brain metastases. Nature reviews Disease primers. 2019;5: 5.
- Brastianos PK, Carter SL, Santagata S et al. Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets. Cancer discovery. 2015.
- Franchino F, Ruda R, Soffietti R. Mechanisms and Therapy for Cancer Metastasis to the Brain. Frontiers in oncology. 2018; 8: 161.
- Gaye E, Geier M, Bore P et al. Intra-cranial efficacy of brigatinib in an ALK-positive non-small cell lung cancer patient presenting leptomeningeal carcinomatosis. Lung cancer (Amsterdam, Netherlands). 2019; 133: 1-3.
- Camidge DR, Kim DW, Tiseo M et al. Exploratory Analysis of Brigatinib Activity in Patients With Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer and Brain Metastases in Two Clinical Trials. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2018; 36: 2693- 2701
- Spencer SA, Riley AC, Matthew A, Di Pasqua AJ. Brigatinib: Novel ALK Inhibitor for Non-Small-Cell Lung Cancer. The Annals of pharmacotherapy. 2019; 53: 621-626.
- Gettinger SN, Bazhenova LA, Langer CJ et al. Activity and safety of brigatinib in ALK-rearranged non-small-cell lung cancer and other malignancies: A single-arm, open-label, phase 1/2 trial. The Lancet Oncology. 2016; 17: 1683-1696.
- Camidge DR, Kim HR, Ahn MJ et al. Brigatinib versus Crizotinib in ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2018; 379: 2027-2039.
- Collen C, Christian N, Schallier D et al. Phase II study of stereotactic body radiotherapy to primary tumor and metastatic locations in oligometastatic nonsmall-cell lung cancer patients. Ann Oncol. 2014.
- Wrona A, Dziadziuszko R, Jassem J. Management of brain metastases in non-small cell lung cancer in the era of tyrosine kinase inhibitors. Cancer treatment reviews. 2018; 71: 59-67.
- Salvati M, Tropeano MP, Maiola V et al. Multiple brain metastases: A surgical series and neurosurgical perspective. Neurol Sci. 2018.
- Wang H, Ou Q, Li D, et al. Genes associated with increased brain metastasis risk in non-small cell lung cancer: Comprehensive genomic profiling of 61 resected brain metastases versus primary non-small cell lung cancer (Guangdong Association Study of Thoracic Oncology 1036). Cancer. 2019.
- Nicoś M, Krawczyk P, Wojas-Krawczyk K et al. Evaluation of ALK gene rearrangement in central nervous system metastases of non-small-cell lung cancer using two-step RT-PCR technique. Clin Transl Oncol. 2017.
- Trejo Bittar HE, Luvison A, Miller C, Dacic S. A comparison of ALK gene rearrangement and ALK protein expression in primary lung carcinoma and matched metastasis. Histopathology. 2017.
- Solomon B, Kim D, Wu Y et al. Final Overall Survival Analysis From a Study Comparing First-Line Crizotinib Versus Chemotherapy in ALK-Mutation-Positive Non-Small-Cell Lung Cancer. 2018; 36: 2251-2258.
- BJ S, T M, DW K, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. 2014; 371: 2167-2177.