
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Closed posterior dislocation of ankle joint without fracture: A case report and literature review
Ashwani Nugur1 *; Lee Hoggett2 ; Siddharth Lokanathan3 ; Sabeen Akhtar4
1DNB Orthopaedics, Trust Registrar, Trauma and Orthopaedics, Pennine Acute Hospital NHS Trust, UK.
2Speciality Registrar, Trauma and Orthopaedics, Health Education North West, UK.
3DNB Orthopaedics, MRCS, Speciality Doctor, Trauma and Orthopaedics, Pennine Acute Hospital NHS Trust, UK
4FRCS (Trauma and Orthopaedics), Consultant Foot and Ankle Specialist, Pennine Acute Hospital NHS Trust, UK.
*Corresponding Author: Ashwani Nugur
DND Orthopaedics, Trust Registrar, Trauma and
Orthopaedics, Pennine Acute Hospital NHS Trust,
UK.
Email: Ashwanikumar.Nugur@pat.nhs.uk
Received : Apr 29, 2021
Accepted : May 31, 2021
Published : Jun 03, 2021
Archived : www.jcimcr.org
Copyright : © Nugur A (2021).
Abstract
Pure Ankle dislocation is an ankle dislocation without any associated fractures of the ankle and an intact tibiofibular syndesmosis. Only a few isolated case reports and small series of cases are reported in literature. We report a posterior dislocation of ankle joint without any bony fractures with description of its mechanism, management, and literature review
Keywords: Pure Ankle dislocation; ankle dislocation without fracture; posterior dislocation of ankle.
Citation: Nugur A, Hoggett L, Lokanathan S, Akhtar S. Closed posterior dislocation of ankle joint without fracture: A case report and literature review. J Clin Images Med Case Rep. 2021; 2(3): 1180.
Background
Pure Ankle dislocation is an ankle dislocation without any associated fractures of the ankle and an intact tibiofibular syndesmosis. These are seen in moderate or high energy trauma and can be either open or closed injuries. Closed pure ankle dislocations are extremely rare and depend on position of ankle at time of injury. Only a few isolated case reports and small series of cases are reported in literature. Most of the previous reported cases are treated with immediate reduction and immobilisation for a period of 6-8 weeks followed by physiotherapy with good functional outcome.
Case presentation
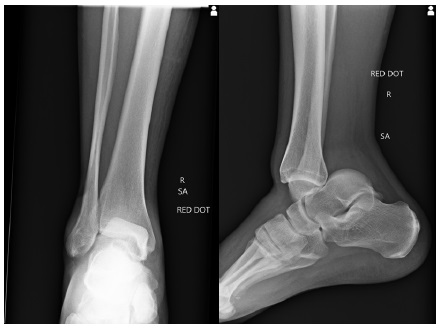
A 48-year-old gentleman with no pre-disposing factors was brought to emergency department with history of falling down 10 steps. He presented with a deformity to his right ankle and bruising over left side of his face. His GCS was 15 on admission. On examination of his right ankle, the distal end of the tibia was prominent anteriorly and impinging on the skin and with foot and heel visibly migrated posteriorly. There was no altered sensation distally. Distal pulses were not palpable but capillary refill time was less than 2 seconds in the toes.
Treatment
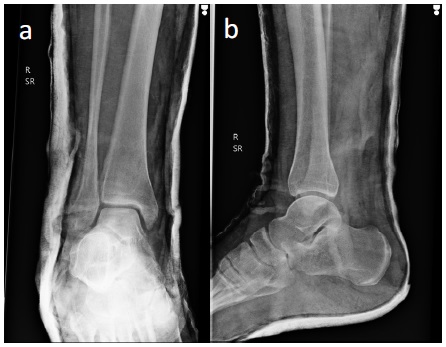
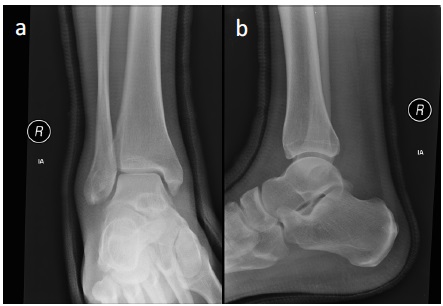
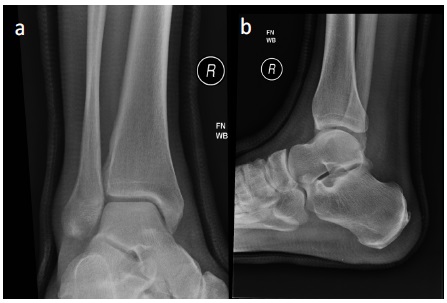
Urgent manipulation under sedation was undertaken in A&E department to reduce the ankle dislocation. Reduction was done with inline traction, with the knee in a flexed position longitudinal traction was applied holding the heel in the direction of deformity with one hand and pushing it anteriorly and a second hand pushing the distal tibia posteriorly. Distal pulses were palpable after reduction and there was no altered sensation distally. Subsequently, a below knee slab was applied. Check x rays were done, and he was sent home with advice of non-weight bearing mobilisation on right leg. A VTE risk assessment was performed and he was discharged from the department with VTE prophylaxis. He was followed up as an outpatient in the fracture clinic and converted into a light-weight fibreglass cast one week following the injury (Figure 3). The cast was removed at 6 weeks after check x ray (Figure 4) and full weight bearing mobilisation was started with a referral to physiotherapy for strengthening. He had returned to his pre-injury level of activity by 12 weeks. He has had a good functional outcome with full range of ankle movement at 7 months follow up.
Discussion
Pure ankle dislocation is an ankle dislocation without any associated fractures. These are seen in moderate or high energy trauma and can be either open or closed injuries. A French surgeon, Peraire reported this for the first time in 1913 [1]. Closed pure ankle dislocations are extremely rare. In the largest series of pure ankle dislocations reported by Moehring, the majority of cases were open dislocations [2]. Systemic review by Lachaln et al of available English literature identified 154 cases with common causes cited as sporting accidents (31%) or motor vehicle accidents (30%). Their analysis showed incidence of pure ankle dislocation is 0.065% (13/20,000) in patients with an ankle injury or 0.46% (23/5000) in patients with an ankle dislocation [3].
The stability of ankle joint depends on bony and soft tissues factors. The Ankle joint is a hinge joint formed by distal tibia, fibula and talus. The rhomboid shaped talus enclosed in the ankle mortise is the main factor for medial and lateral stability of ankle joint [4]. The soft tissues comprise of ligaments, muscle, tendons and joint capsule and contribute to the stability of the mortice joint alongside the bony architecture. The ligaments on the medial aspect are the deep and superficial deltoid ligaments. On the lateral aspect the ligamentous complex is made up of the anterior talofibular ligament, calcaneal fibular ligament and posterior talofibular ligament. These medial and lateral ligament structures give additional stability in the mediolateral plane. However, anterior posterior stability is weaker with only support from the joint capsule and the muscles and tendons crossing ankle joint. The position of ankle at the time of incident determines this unique injury. A classification by Fahey and Murphy is based on the direction of displacement of talus, it can be anterior, posterior, medial, lateral and upward direction or a combined form [5]. Most of reported cases are posterior or posteromedial dislocations. According to the previous reported few case series, it is suggested pure ankle dislocation occurs when the rhomboid shaped talus slips out posteriorly - the ankle is in maximally plantar flexed and inverted position with axial loading [6-8]. Moehring et al proposed pure ankle dislocation can occur due to predisposing factors like medial malleolus hypoplasia, ligamentous laxity and peroneal muscle weakness [2]. Although rare, neurovascular complications have also been reported with type of injury. Wroble et al reported about 10% incidence of vascular and neurological damage [9]. Garbuio et al in their series had five cases with nerve involvement [6]. Neurovascular compromise and infections were predominantly seen in open injuries and these require early reduction, meticulous debridement and washout [2,10]. Literature also reports cases with devastating complication leading to amputation due to vascular compromise [2,11]. In our case, this injury was as result a moderate energy trauma resulting in a closed isolated ankle dislocation. Although distal pulses were not palpable initially due the deformed position of ankle, they were palpable soon after reduction. He did not have neurological symptoms
Evidence supports conservative management with Immediate closed manipulation under sedation or anaesthesia as the preferred method of treatment [12,13]. Urgent reduction is important as to prevent neurovascular compromise, avoid skin damage and reduce swelling. Reduction is performed with inline traction. The knee is flexed to relax the achilles tendon. The heel is grasped with one hand, longitudinal traction is applied, and the heel is translated anteriorly to reduce the talus back to its anatomical position. Once reduced, most authors recommend that the ankle should be immobilised in cast for a period of 6-8 weeks [14-16]. Tarantino et al recommended immobilisation for a shorter period of 30 days [17]. CT scan can be done in suspicion of any osteochondral loose bodies trapped within the joint. In case of any instability post removal of plaster cast, an MRI scan may be performed to assess the extent of ligament injury. In our case, the ankle was immobilised in a backslab for 1 week and then a full cast for a further 5 weeks. As he did not have osteochondral fragment visible on radiographs and did not have instability during cast application at 1 week and after cast removal, CT scan and MRI scan was not required. A Cadaveric study has shown that plantarflexion injuries results in rupture of soft tissues like anterior joint capsule, anterior talofibular ligament and deep fibres of deltoid ligament [18]. However, controversy remains in terms of acute ligament repair. Open injuries and unstable ankle joint may require surgical treatment in form of external fixator application, capsule repair and ligament reconstruction. Toohay et al noted that instability is rare even with massive ligament ruptures [19]. It is described that ligaments are opposed once reduced and are always shredded and contused in these dislocations which makes the repair difficult. Uçar et al in their series of open pure dislocations, performed debridement and primary closure of wounds without repair of capsule or ligaments and the ankle was immobilised in cast for 4 weeks and then angle adjustable brace for applied for next 2 weeks [20]. A study by Finkemeier et al recommend late ligament repair in cases of instability and propose conservative management in both closed and open tibiotalar dislocations without fractures [21]. In a series of 16 cases by Elise et al found no instability, two patients presented joint stiffness, and four patients complained about paraesthesia in the areas of the anterior tibial nerve or intermediary dorsal cutaneous nerve. They also reported 25% had persistent pain and degenerative arthritis [12]. Recent systemic review by Lachaln et al of available English literature noted that 50% (77/154) of cases were open and 73% of cases were in males. 46% of 154 patients were treated nonoperatively and 26% (37 patients) had ligamentous repair. The mean period of immobilisation was just over 6 weeks (range 2-16 weeks). Most of the patients had good functional outcomes. The most common long-term complications were reduced ankle range of motion with incidence of 18%. Ankle instability was present in only 2.6% and it was not influenced by acute ligament repair [3]. In the Moehring et al. series with follow up ranging from 15 months to 10 years, 2 patients out of 12 had bad results and one had degenerative arthritis[2]. Garbuio et al. in their series with a mean follow up of 12 months, had a high rate of degenerative changes in the joint five out of nine cases [6]. Wroble et al in their series with long follow up ranging from 2 to 24 years all patients had calcifications and osteophytes on radiographs, however range of motion of ankle was normal in all expect for 4 patients [9]. Uçar et al reported 1 out 5 patients had joint space narrowing and osteophytes after 6 years of follow up [20]. Our patient returned to his pre-injury level of activity by 12 weeks and was having painless full range of motion and stable ankle at his 7 months follow up visit but had mild paraesthesia around heel. However, long term followup is needed to look for any degenerative changes.
Learning points
- Closed ankle dislocation without fracture is a rare injury.
- They require immediate closed manipulation.
- They have good functional outcome with immobilisation for 6 weeks followed by physiotherapy.
- These injuries do not always require cross sectional imaging
References
- Peraire A. Luxation tibo-astragalienne avec issue à l’extérieur du péroné non fracturé à travers une boutonnière cutanée. Présentation de malade. Paris Chir. 1913; 5: 959.
- Moehring H, Tan R, Marder R, Lian G. Ankle dislocation. J Orthop Trauma. 1994; 8: 167–72
- Lachlan W, David O, Daniel G, Markus K. Pure Ankle Dislocation: A Systematic Review of the Literature and Estimation of Incidence. Injury. 2017; 48: 2027-2034.
- Bonnin J. Dislocations and fracture-dislocations of the talus. Br J Surg. 1940; 28: 88
- Fahey JJ, Murphy JL. Dislocations and fractures of the talus. Surg Clin North Am. 1965, 45: 79–102.
- Garbuio P, Gerard F, Gagneux E. Pure dislocation of the tibiotalar joint. Report of 9 cases. Rev Chir Orthop. 1995; 81: 601–608.
- Shaik MM, Tandon T, Agrawal Y, Jadhav A, Taylor LJ. Medial and lateral rotatory dislocations of the ankle after trivial trauma– pathomechanics and management of two cases. J Foot Ankle Surg. 2006; 45: 346–350.
- Prost à la Denise J, Tabib W, Pauthier F. Long‐term result of a pure tibiotalar dislocation in a child. Orthop Traumatol Surg Res. 2009; 95: 558–562.
- Wroble RR, Nepola J, Malvitz TA. Ankle dislocation without fracture. Foot Ankle. 1988; 9: 64–74.
- Dlimi F, Mahfoud M, Berrada MS, El Bardouni A, El Yaacoubi, M. Open medial ankle dislocation without associated fracture: A case report. Foot Ankle Surg. 2011; 5: 008.
- Kelly PJ, Peterson LF. Compound dislocation of the ankle without fracture. Am J Surg. 1962; 103: 170–172.
- Elisé S, Maynou C, Mestdagh H, Forgeois P, Labourdette P. Tibiotalar dislocations without associated fracture: report on 16 cases. Acta Orthop Belg. 1998; 64: 25–34
- Georgilas I, Mouzopoulos G. Anterior ankle dislocation without associated fracture: A case with an 11-year follow-up. Acta Orthop Belg. 2008; 74: 266–269.
- Colville, MR; Colville, JM, Manoli A, 2nd: Posteromedial dislocation of the ankle without fracture. J Bone Joint Surg Am. 1987; 69: 706 – 711
- Hatori M, Kotajima S, Smith RA, Kokubun S. Ankle dislocation without accompanying malleolar fracture. Acase report. Ups J Med Sci. 2006; 111: 263 – 268.
- Thangarajah T, Giotakis N, Matovu E. Bilateral ankle dislocation without malleolar fracture. J Foot Ankle Surg. 2008; 47: 441– 446.
- Tarantino U, Cannata G, Gasbarra E, et al. Open medial dislocation of the ankle without fracture. J Bone Joint Surg Br. 2008; 90: 1382-1384.
- Funk JR. Ankle injury mechanisms: lessons learned from cadaveric studies. Clin Anat. 2011; 24: 350–361.
- Toohey J, Worsing R. A long term of follow up study of tibiotalar dislocations without associated fractures. Clin Orthop. 1989; 239: 207–210
- Bekir Yavuz Uçar, Serdar Necmioğlu, Mehmet Bulut, Ibrahim Azboy, Abdullah Demirtaş, Open Ankle Dislocations Without Associated Fracture. Foot & Ankle International. 2012; 33: 828-831.
- Finkemeier C, Engebretsen L, Gannon J. Tibiotalar dislocation without fracture: treatment principles and outcome. Knee Surg Sports Traumatol Arthrosc 1995; 3: 47–49.