
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Madelung’s disease: A case report of laryngeal localization and a review of the literature
Fabrizia Elli1 *; Marco Stacchini2 ; Alberto Daniele Arosio1,5; Roberta Priola3 ; Tommaso Mazzocco4 ; Marco Limarzi2
1Division of Otorhinolaryngology, Department of Biotechnology and Life Sciences, University of Insubria, Varese, Italy.
2Division of Otorhinolaryngology, M. Bufalini Hospital, Cesena, Italy
3Division of Otorhinolaryngology, Department of Biomedicine, Neuroscience and Advanced Diagnostics (BiND), University of Palermo, Palermo, Italy
4Department of Biomedical Sciences and Advanced Therapies, University of Ferrara, Italy.
5PhD student, Biotechnologies and Life Sciences, University of Insubria, Varese, Italy.
*Corresponding Author: Fabrizia Elli
Division of Otorhinolaryngology, Department of
Biotechnology and Life Sciences, University of
Insubria, Ospedale di Circolo e Fondazione Macchi,
Via Guicciardini 9, 21100, Varese, Italy.
Email: fabrizia.elli@hotmail.it
Received : May 01, 2021
Accepted : Jun 01, 2021
Published : Jun 03, 2021
Archived : www.jcimcr.org
Copyright : © Elli F (2021).
Abstract
Madelung’s Disease (MD), also known as benign multiple symmetric lipomatosis or Launois-Bensaude syndrome, is a rare condition. The characteristic feature is the presence of numerous diffuse lipomas at the level of the neck or upper limbs. The etiology is unknown, but a close association with ethyl abuse has been observed. The use of radiological examinations such as ultrasound, computed tomography and magnetic resonance imaging is helpful for the differential diagnosis. There are two classifications mainly used: The Enzi classification and the Donhauser classification. In this article we present a case of MD with laryngeal localization. A 50-year-old man was referred to our department complaining of dysphonia for about 6 months. An abnormal and diffuse enlargement of the anterior part of the neck was noticed, compatible with “Madelung’s Collar”. Fiberoptic examination of the larynx revealed the presence of a lipomatous-like neoformation of the left false vocal cord. The patient underwent surgical removal of the laryngeal neoformation with transoral laser microsurgery. With this article we suggest a possible diagnostic and therapeutic procedure for the treatment of laryngeal lipomatosis.
Keywords: Lipoma; TML; Larynx; Dysphonia; ENT
Citation: Elli F, Stacchini M, Arosio AD, Priola R, Mazzocco T, et al. Madelung’s disease: A case report of laryngeal localization and a review of the literature. J Clin Images Med Case Rep. 2021; 2(3): 1181.
Introduction
Madelung’s Disease (MD), also known as Launois-Bensaude syndrome or multiple symmetric lipomatosis and benign symmetric lipomatosis [1], is a rare condition, with a prevalence of 1: 25,000. It mainly affects males living in the Mediterranean area, with a male: female ratio 15-30: 1 [2]. It presents with the appearance of diffuse lipomas in the proximal upper limbs and neck. The etiology is unknown, but it seems that catecholamines have a fundamental role in promoting the process of lipogenesis [3] and an association with chronic alcoholism (60- Abstract Madelung’s Disease (MD), also known as benign multiple symmetric lipomatosis or Launois-Bensaude syndrome, is a rare condition. The characteristic feature is the presence of numerous diffuse lipomas at the level of the neck or upper limbs. The etiology is unknown, but a close association with ethyl abuse has been observed. The use of radiological examinations such as ultrasound, computed tomography and magnetic resonance imaging is helpful for the differential diagnosis. There are two classifications mainly used: The Enzi classification and the Donhauser classification. In this article we present a case of MD with laryngeal localization. A 50-year-old man was referred to our department complaining of dysphonia for about 6 months. An abnormal and diffuse enlargement of the anterior part of the neck was noticed, compatible with “Madelung’s Collar”. Fiberoptic examination of the larynx revealed the presence of a lipomatous-like neoformation of the left false vocal cord. The patient underwent surgical removal of the laryngeal neoformation with transoral laser microsurgery. With this article we suggest a possible diagnostic and therapeutic procedure for the treatment of laryngeal lipomatosis. Keywords: Lipoma; TML; Larynx; Dysphonia; ENT. 90% of patients) is reported [4]. In its classic form, a specific sign is represented by an important flaring at the level of the anterior neck, which is known as Madelung collar or horse collar [5,6]. Diagnosis is based on the patient’s history and physical examination, while imaging in the form of ultrasound, computed tomography and magnetic resonance, can help in the differential diagnosis. In this report, we present a case of laryngeal MD and share our experience in its treatment.
Case report
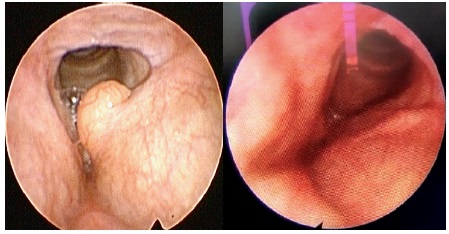
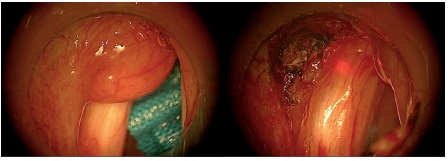
A 50-year-old man presented with a 6-month history of mild dysphagia and progressive dyspnea. Flexible transnasal endoscopy revealed a cystic growth originating from the left ventricle, partially projected into the lumen, with partial reduction of the respiratory space. The lesion was approximately 1.5 cm in diameter, translucent in appearance and covered with normal mucosa (Figure 1a). Both vocal cords were moble and hypopharyngeal and laryngeal anatomy showed no other abnormalities. CT scan showed hypertrophy of the paraglottic adipose tissue at the level of the left false vocal cord, extended up to its free edge (Figure 2). Neck US showed hypertrophic - hyperechoic tissue apparently of lipomatous nature at the level of the neck and the parotid. Indication to surgical removal via Transoral Laser Microsurgery (TLM) was given. The size of the lesion and its welldefined border allowed for complete surgical excision. At the end of the procedure, a continuous wave laser treatment on the excisional margins and on the wound bed was performed [7], in order to prevent possible relapses (Figure 3).
The patient was discharged the day after the surgery, reporting neither dysphagia nor breathing difficulties. Pathological examination revealed a 1.5 cm lipomatous formation with focal spindle cells, without atypia. After 2 months, no recurrence was noticed (Figure 1b).

Discussion
MD is a rare disease the pathophysiology of which is still unknown. Various theories have been proposed: A defect in the lipolytic pathway in response to catecholamines [3] or mutations or deletions of mitochondrial DNA [8]. Two different classifications are used in clinical practice: the classification by Enzi et al [9], based on the anatomical distribution of fat, and the more recently proposed by Donhauser et al [10]. Enzi's classification defines two categories: type 1, in which the distribution of fat is symmetrical and mainly involves neck, shoulders, supraclavicular triangle and proximal upper limbs and type 2, in which fat deposits are localized in the abdomen and thighs (also typical of the patient with classical obesity). The Donhauser classification defines three types of MD: Type 1 - neck distribution, type 2 - pseudo-athletic appearance and type 3 - gynecological appearance (Table 1).
Table 1: Enzi and Donhauser classification of Madelung's disease.
Enzi |
Donhauser |
Affected body areas |
Type 1 |
Type I (horse collar) |
Neck, upper back, shoulder girdle, and upper arms |
Type II (pseudo athletic type) |
Shoulder girdle, deltoid region, upper arms, and thorax |
|
Type III (gynecoid type) |
Lower body, especially the thighs and medial side of the knees |
|
Type 2 |
Type IV (abdominal type) |
Abdomen |
The use of imaging is an aid in the diagnosis. CT scans primarily evaluate the size and location of the growth, while MRI provides superior definition of the soft tissues [11] allowing for better delineation of the extent and localization of the mass. On MRI, MD-related fat appears as unencapsulated and distributed along the vascular / muscular planes. On the contrary, the classic lipomas are localized in the subcutaneous space with an unencapsulated appearance.
Differential diagnosis encompasses other pathologies such as angiolipoma, neurofibroma, liposarcoma, lipoblastomatosis, lipodystrophy, lymphoma, neurofibromatosis and diseases of the salivary glands. Lipomas usually grow slowly and might cause aesthetic problems, rarely causing mass effect on surrounding structures, with symptoms depending upon their size and location. Laryngeal lipomas are rare, representing around 0.6% of all benign lesions of the larynx [12]. Given their location, they can be responsible for pharyngodynia, hoarseness, dyspnea and dysphagia. To date, 73 clinical cases of laryngeal lipomas have been found in the literature (Table 2).
Table 2: Summary of reported cases of endolaryngeal lipoma from 1994 to today.
Author |
Country |
No. pts. |
Age/ sex |
Site |
Symptoms |
Eckel and Jungehülsing, [23] 1994 |
Germany |
3 |
- |
Hypopharynx |
- |
Zbären et al, [23] 1995 |
Switzerland |
1 |
47/M |
Larynx |
- |
Wenig et al, [23] 1995 |
USA |
3 |
28/F |
Supraglottic larynx (n = 2) and piriform sinus |
Airway obstruction, dysphagia, throat discomfort, sensation of excessive secretion in the throat |
Welinder et al, [23] 1996 |
Denmark |
1 |
- |
Vallecula epiglottica |
Fatal airway obstruction |
Anand, [13] 1997 |
India |
1 |
48/M |
Right aryepiglottic fold |
Intermittent respiratory obstruction |
Mevio et al, [14] 1997 |
Italy |
1 |
- |
Larynx |
- |
Gao et al, [23] 1997 |
China |
1 |
- |
Hypopharynx |
Dysphagia, throat discomfort, and airway obstruction |
Yoskovitch et al, [15] 1999 |
Canada |
1 |
- |
- |
- |
Barry et al, [23] 2000 |
France |
5 |
M/F |
Hypopharynx and larynx |
- |
Jungehülsing et al, [23] 2000 |
Germany |
7 |
M/F |
Hypopharynx and larynx |
- |
Maged and Riad, [23] 2000 |
Scotland |
1 |
50/M |
Larynx |
Hoarseness and dyspnea |
Srinivasan and Davies, [23] 2000 |
UK |
1 |
57/M |
Pharynx and larynx |
Snoring and intermittent choking |
Nishiyama et al, [23] 2001 |
Japan |
1 |
82/F |
Hypopharynx |
Wheezing and intermittent breathlessness |
Grützenmacher et al, [23] 2002 |
Germany |
1 |
42/M |
Left aryepiglottic fold |
Throat discomfort and airway obstruction |
Lippert et al, [23] 2002 |
Germany |
2 |
-/- |
- |
- |
Miloudi et al, [23] 2005 |
Morocco |
1 |
57/F |
Epiglottis |
Dyspnea and dysphagia |
Singhal et al, [23] 2005 |
India |
1 |
56/F |
Epiglottis |
Fatal airway obstruction |
Dereköy et al, [23] 2007 |
Turkey |
1 |
63/F |
Tonsil |
Confusion, disorientation, and difficult intubation |
Jawar et al, [17] 2007 |
India |
1 |
63/M |
Right arytenoid |
Change of voice |
Mitchell et al, [23] 2007 |
UK |
1 |
62/F |
Oropharynx |
Stridor |
Mattioli et al, [23] 2008 |
Brazil |
1 |
58/M |
Larynx |
Hoarseness and dyspnea |
Minni et al, [23] 2008 |
Italy |
1 |
48/M |
Paraglottic space |
Hoarseness and soft voice |
De Vincentis et al, [23] 2010 |
Italy |
1 |
62/M |
Right ary-epiglottic fold |
Dyspnea, dysphonia |
Mohammad et al, [23] 2010 |
Iran |
1 |
41/M |
Right supraglottic larynx |
Voice change and dyspnea |
Megan et al, [20] 2010 |
England |
1 |
-/- |
Larynx |
- |
Eyigor et al, [23] 2011 |
Turkey |
1 |
60/M |
Vocal fold and vocal process of the arytenoids |
Hoarseness |
Lee DH et al, [16] 2011 |
Korea |
1 |
- |
Larynx |
Dyspnea |
Nader et al, [23] 2012 |
Iran |
1 |
63/M |
Right aryepiglottic fold |
Intermittent stridor and snoring |
Landínez-Cepeda et al, [21] 2012 |
Spain |
1 |
-/M |
Larynx |
Dyspnea |
Lee HS et al, [22] 2013 |
Taiwan |
4 |
-/M 56/M 57/M 50/M |
Glottic larynx (n = 3) and larynx |
Dyspnea, stridor, neck swelling, dysphonia |
D’antonio et al, [24] 2013 |
Italy |
1 |
65/M |
Left true vocal fold |
Hoarseness, choking spells, stridor, dyspnea |
Cáceres et al, [25] 2013 |
Spain |
1 |
-/- |
Pharyngoepiglottic |
- |
Sotirović et al, [26] 2014 |
Serbia |
1 |
- |
Hypopharynx |
- |
Kodiyan et al, [27] 2015 |
USA |
2 |
58/M 79/F |
Larynx |
Shortness of breath, dysphagia, and globus sensation. Non-progressive hoarseness and globus sensation |
Tan et al, [28] 2016 |
Malaysia |
1 |
55/M |
Right vallecula |
Odynophagia and mild shortness of breath |
Bochnia et al [29] 2016 |
Poland |
1 |
-/- |
Left arytenoepiglottic fold |
Light dysphagia |
Hui Zhu et al, [30] 2016 |
USA |
3 |
34/M 70/F 56/M |
Left arytenoids |
Hoarseness and difficulty breathing. |
Hypopharyx |
|||||
Posterior arytenoids and left piriform sinus |
|||||
Acquaviva et al, [31] 2016 |
Italy |
1 |
63/F |
Left piriform sinus |
Severe dyspnea |
Deutsch et al, [32] 2016 |
UK |
1 |
62/M |
Left laryngopharynx |
Intermittent airway obstruction, dysphagia |
Demir et al, [33] 2016 |
Turkey |
1 |
34/- |
False vocal fold |
Hoarseness, globus sensation |
Wolf-Magele et al, [34] 2016 |
Austia |
1 |
-/- |
Larynx |
Stridor and dyspnea |
Nada et al, [35] 2017 |
Tunisia |
1 |
32/F |
Left aryepiglottic fold |
Changes in voice |
Burkes et al, [36] 2019 |
USA |
1 |
-/M |
Larynx |
Hoarseness, dysphagia, globus sensation, and neck fullness |
Reid et al, [37] 2019 |
Canada |
2 |
-/- |
Larynx |
Dyspnea, hoarseness and stridor |
Azimivaghar et al, [38] 2019 |
India |
1 |
68/M |
Left glottic |
Dysphonia |
Azandaryani et al, [39] 2019 |
India |
1 |
47/M |
Left supraglottic larynx |
Hoarseness, dyspnea and neck fullness |
Okromelidze et al, [40] 2019 |
USA |
1 |
51/M |
Left vocal folds |
Hemoptysis and sore throat |
Yunxia et al, [41] 2020 |
China |
1 |
70/M |
Suglottic |
Progressive dyspnea |
Qin-Ying et al, [42] 2020 |
China |
1 |
65/F |
Left epiglottis |
Pharyngeal paraesthesia |
Lombardo et al, [43] 2020 |
Italy |
1 |
28/F |
Left aryepiglottic fold |
Dyspnea |
Azar et al, [44] 2021 |
USA |
1 |
35/M |
Supraglottic |
Dysphagia and dyspnea |
The elective treatment of a laryngeal lipoma is radical surgical excision to reduce the chances of recurrence. Depending on the size and location of the tumor, endoscopic removal, with or without CO2 laser, is indicated for lipomas smaller than 2 cm [36,37]. On the contrary, for non-pedunculated tumors or tumors larger than 2 cm, the definitive treatment is through an open technique with an external approach (thyrotomy, transhyoid pharyngotomy or lateral pharyngotomy) [36,38]. In the case exposed, the use of the TLM CO2 laser proved to be effective in granting a radical excision in the absence of bleeding or other complications. The use of the photocoagulation technique on the resection margins was employed in order to decrease the chance of recurrence [34].
Conclusion
Lipomas of the larynx are rare and often asymptomatic diseases. However, as their dimension increases, they might lead to life-threatening clinical situations, including airway obstruction. In the literature, 2 cm lipomas represent the maximum limit for the use of intraoral surgery. Beyond this dimension, the surgical approach with an open technique might find indication. The use of the TLM with CO2 laser made it possible to perform a less invasive surgery with a lower risk of bleeding, while granting a radical excision and a shorter hospitalization [26].
Authors' contributions: All authors contributed to data analysis and manuscript writing. All authors have reviewed and approved the final version of the manuscript.
References
- Liu G, Liu T, Shen C, Zhou L, Ouyang R. A case reports. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2020 28; 45: 96-101.
- Jimenez Aragon F, Morales Puebla JM, Corzon Pereira T. Madelung’s disease. Acta Otorrinolaringol Esp. 2013; 64: 166-167
- Enzi G, Inelmen EM, Baritussio A, Dorigo P, Prosdocimi M, Mazzoleni F. Multiple symmetric lipomatosis: A defect in adrenergicstimulated lipolysis. J Clin Invest. 1977; 60: 1221-1229.
- Brea-Garcia B, Cameselle-Teijeiro, J, Couto-Gonzalez, I, TaboadaSuarez, A, et al. Madelung’s disease: Comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthetic Plast Surg. 2013; 37: 409-416.
- Gonzalez-Garcia R, Rodriguez-Campo FJ, Sastre-Perez J, Munoz-Guerra MF. Benign symmetric lipomatosis (Madelung’s disease): Case reports and current management. Aesthetic Plast Surg. 2004; 28: 108-112.
- Verna G, Kefalas N, Boriani F, Carlucci S, Choc I, et al. LaunoisBensaude syndrome: An unusual localization of obesity disease. Obes Surg. 2008; 18: 1313-1317.
- Wolf-Magele A, Schnabl J, Url C. et al. Acute dyspnea caused by a giant spindle cell lipoma of the larynx. Wien Klin Wochenschr. 2016; 128: 146–149
- Plummer C, Spring PJ, Marotta R, Chin J, Taylor G, et al. Multiple symmetrical lipomatosis: A mitochondrial disorder of brown fat. Mitochondrion. 2013; 13: 269-276.
- Enzi G, Busetto L, Ceschin E, Coin A, Digito M, et al. Multiple symmetric lipomatosis: Clinical aspects and outcome in a longterm longitudinal study. Int J Obes Relat Metab Disord. 2002; 26: 253-261.
- Donhauser G, Vieluf D, Ruzicka T, Braun-Falco O. Benign symmetric Launois-Bensaude type III lipomatosis and BureauBarrière syndrome. Hautarzt. 1991; 42: 311-314.
- Schrader M. Improved diagnosis of laryngeal lipoma by computerized tomography. HNO. 1988; 36: 161–163.
- Khorsandi Ashtiani MT, Yazdani N, Saeedi M, et al. Large lipoma of the larynx: a case report. Acta Med Iran 2010; 48: 353–356.
- Job A. Recurrent laryngeal lipoma. Indian journal of otolaryngology and head and neck surgery: Official publication of the Association of Otolaryngologists of India. 1997; 49: 284-285.
- Mevio E, Calabrò P, Redaelli GA, Perano D, Rosso R. Lipomatosi simmetrica benigna: Malattia di Madelung [Benign symmetrical lipomatosis: Madelung’s disease. Acta Otorhinolaryngol Ital. 1997; 17: 64-67
- Yoskovitch A, Cambronero E, Said S, Whiteman M, Goodwin WJ. Giant lipoma of the larynx: A case report and literature review. Ear Nose Throat J. 1999; 78: 122-125.
- Lee DH, Lim SC, Lee JK. Laryngeal involvement in Madelung disease. Otolaryngol Head Neck Surg. 2011; 144: 481-482.
- Talsania J, Shah VP, Shah AL, Goyal MN, Manjunatha Rao SV. Unusual case of laryngeal lipoma. Indian J Otolaryngol Head Neck Surg. 2007; 59: 85-86.
- De Vincentiis M, Greco A, Mascelli A, Soldo P, Zambetti G. Lipoma of the larynx: A case report. Acta Otorhinolaryngol Ital. 2010; 30: 58-63.
- Khorsandi Ashtiani MT, Yazdani N, Saeedi M, Amali A. Large Lipoma of the Larynx: A Case Report. Acta Med Iran. 2010; 48: 353-356.
- Durr ML, Agrawal N, Saunders JR, Ha PK. Laryngeal lipoma associated with diffuse lipomatosis: Case report and literature review. Ear Nose Throat J. 2010; 89: 34-37.
- Landínez-Cepeda GA, Alarcos-Tamayo EV, Millás-Gómez T, Morais-Pérez D. Laryngeal lipoma associated with Madelung’s disease: A case report. Acta Otorrinolaringol Esp. 2012; 63: 311-313.
- Lee HS, Koh MJ, Koh YW, Choi EC. Transoral robotic surgery for huge spindle cell lipoma of the hypopharynx. J Craniofac Surg. 2013; 24: 1278-1279.
- Nader S, Nikakhlagh S, Rahim F, Fatehizade P. Endolaryngeal lipoma: Case report and literature review. Ear Nose Throat J. 2012; 91: E18-21.
- D’Antonio A, Mottola G, Caleo A, Addesso M, Boscaino A. Spindle cell lipoma of the larynx. Ear Nose Throat J. 2013; 92: E9.
- Cáceres Gómez-Valadés R, Rodríguez Pérez MI, Pedrero Gil AL, Zambrano Castaño D. Lipoma faringoepiglótico gigante pediculado en vía aérea [Pedunculated giant pharyngoepiglottic lipoma in the airway]. Rev Esp Anestesiol Reanim. 2013; 60: 544.
- Sotirović J, Vukomanović-Djurdjević B, Baletić N, Pavićević L, Bijelić D, Perić A. Recurrent lipomatous tumor of hypopharynx: case report and literature review. Acta Clin Croat. 2014; 53: 365-368.
- Kodiyan J, Rudman JR, Rosow DE, Thomas GR. Lipoma and liposarcoma of the larynx: case reports and literature review. Am J Otolaryngol. 2015; 36: 611-615.
- Tan KS, Jalaluddin WMS. Lipoma of vallecula-a case report. BJR Case Rep. 2016; 2: 20150460.
- Bochnia M, Grabowski K, Zalewska A, Morawska–Kochman M. Angiofibrolipoma of the larynx: Case report and literature review. Head Neck. 2016; 38: E81-E83.
- Zhu H, Sun J, Wei S, et al. Well-Differentiated Laryngeal/Hypopharyngeal Liposarcoma in the MDM2 Era Report of Three Cases and Literature Review. Head and Neck Pathol. 2017; 11: 146–151.
- Gilberto Acquaviva, Theodoros Varakliotis, Stefano Badia, Francesco Casorati, Alberto Eibenstein, Gianluca Bellocchi, “Lipoma of Piriform Sinus: A Case Report and Review of the Literature”, Case Reports in Otolaryngology. 2016; 2521583.
- Deutsch PG, O’Connell J. Laryngeal lipoma: A rare cause of acute intermittent airway obstruction. BMJ Case Rep. 2016; 2016: bcr2016215506.
- Demir D, Eraslan Ö, Güven M, Kösem M. Rare cases of benign tumors of the head and neck: lipoma of larynx and sternocleidomastoid muscle. Kulak Burun Bogaz Ihtis Derg. 2016; 26: 118-122.
- Nada G, Omezzine JS, Maher D, Nouha BH, Hssine H. Laryngeal lipoma: A rare cause of dysphonia. Pan Afr Med J. 2017; 26: 9.
- Burkes JN, Campos L, Williams FC, Kim RY. Laryngeal Spindle Cell/ Pleomorphic Lipoma: A Case Report. An In-Depth Review of the Adipocytic Tumors. J Oral Maxillofac Surg. 2019; 77: 1401-1410.
- Reid J, Wehrli B, Sowerby LJ. Spindle Cell Lipomas of the Respiratory Tract: A Case Report and Comprehensive Literature Review. Ann Otol Rhinol Laryngol. 2019; 128: 1086-1091.
- Azimivaghar J, Javadirad E, Montazer S. Laryngeal Lipoma: A Clinicopathologic Case Report. Indian J Otolaryngol Head Neck Surg. 2019; 71: 876-878.
- Azandaryani AR, Eftekharian M, Taghipour M. Large Laryngeal Lipoma with Extra Laryngeal Component Mimics Mixed Form Laryngocele: A Case Report. Adv J Emerg Med. 2019; 3: e45.
- Okromelidze L, Middlebrooks EH, Bhatt AA. Lipoma of the Larynx and Other Differential Diagnoses. J Clin Imaging Sci. 2019; 9: 51.
- Ma Y, Zhou B, Wang S. Large lipoma in the subglottic larynx: A case report. Journal of International Medical Research. 2020.
- Qin-Ying W, Shui-Hong Z, Yong-Cai L, Hai-Hong C. Spindle cell lipoma of the larynx: A case report. Medicine (Baltimore). 2020; 99: e21118.
- Lombardo N, Lobello N, Piazzetta G, Ciriolo M, Pelaia C, et al. Intrinsic Laryngeal Lipoma Treated with Transoral CO₂ Laser Microsurgery: An Unusual Case Report. Am J Case Rep. 2020; 21: e920528.
- Azar SS, Buen F, Chia JJ, Ma Y, Caron J, Dry S, et al. Spindle Cell Lipoma Arising from the Supraglottis: A Case Report and Review of the Literature. Head Neck Pathol. 2021.
- Kanika Rana, Ravi Meher, Ishwar Singh, Vineet Narula, Jaffer Husein Sura, Lipoma in unusual head and neck region: Case series of 4 patients, International Journal of Pediatric Otorhinolaryngology. 2013; 8: 75-78.