
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Recurrent soft tissue infections associated with complex regional pain syndrome type ll: Reports of two unusual cases
Kannangara Don Walter*; Pandya Dhyanesh
St Luke’s University Health Net Work, Warren Campus, Phillipsburg, NJ 08865, USA.
*Corresponding Author: Kannangara Don Walter
St Luke’s University Health Net Work, Warren Campus,
Phillipsburg, NJ 08865, USA.
Email: kannangara@att.net
Received : Apr 27, 2021
Accepted : Jun 01, 2021
Published : Jun 04, 2021
Archived : www.jcimcr.org
Copyright : © Kannangara DW (2021).
Abstract
Complex Regional Pain Syndrome (CRPS) (Synonyms: Reflex Sympathetic Dystrophy, Causalgia, Sudeck’s atrophy, Algodystrophy) is a chronic neurological condition, usually involving the limbs, that is characterized by severe pain along with sensory, autonomic, motor and trophic involvement. CRPS type ll is when there is an identifiable preceding event causing nerve damage. We present 2 unusual cases: 1. spontaneous bleeding from left leg associated with recurrent infections 2. a calcified mass in abdominal wall with recurrent infections. Recurrent soft tissue infections are rare in CRPS. Both presentations were unique.
Case 1
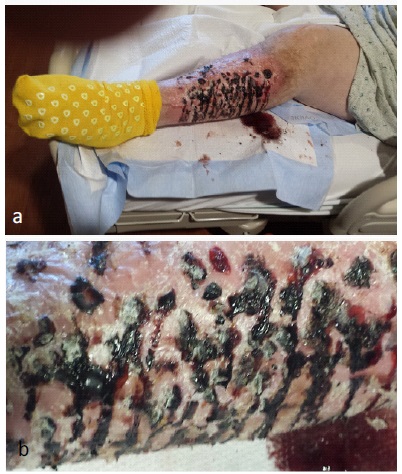
“Spontaneous bleeding from leg” This patient’s CRPS symptoms began after multiple leg surgeries as a teenager. He presented with excruciating leg pain, hyperalgesia and severe vasomotor disturbances resulting in multiple episodes of spontaneous bleeding from the leg and recurrent infections (Figure 1a,b). He has received multiple nerve blocks, pharmacotherapy and debridement of blood clots attached to skin in the operating room due to extreme pain which prevented from cleaning the leg without anesthesia. Episodes of bleeding are usually followed by leg cellulitis for which he has received multiple courses of antibiotics. None of the interventions has resulted in significant relief.
Case 2
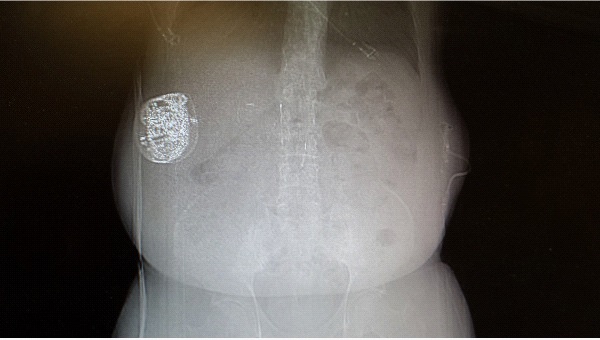
“Calcified mass in abdominal wall” The symptoms in this patient followed a motor vehicle accident 16 years ago. He was admitted to the hospital with a draining sinus in the anterior abdominal wall. A Computed Tomogram (CT) of the abdomen revealed a seroma with a calcified wall at a former embedded morphine pump site (Figure 2). Alcohol sclerotherapy and Jackson-Pratt (JP) drain placement failed. The patient was readmitted a week later with fever, and the fluid from JP drain grew methicillin susceptible Staphylococcus aureus, Enterococcus faecalis and group B Streptococcus. The patient was penicillin allergic. Treatment with vancomycin failed. New cultures grew Citrobacter freundii and Escherichia coli. The calcified mass was surgically excised. He was then treated with ertapenem. The wound eventually closed after one month.
Keywords: Complex regional pain syndrome; Recurrent infections; Spontaneous bleeding.
Citation: Kannangara DW, Dhyanesh P. Recurrent soft tissue infections associated with complex regional pain syndrome type ll: Reports of two unusual cases. J Clin Images Med Case Rep. 2021; 2(3): 1184.
Introduction
Historically the earliest references to CRPS probably dates back to Ambrose Paré, a barber and surgeon during the 16th century reign of French King Charles IX, who recognized a severe and persistent pain syndrome after limb phlebotomy, or ‘Bloodletting’ [1]. The earliest cases of CRPS in North America were likely described in 1864 by physician Silas Weir Mitchell, who characterized a specific type of pain resulting from gunshot wounds during the Civil War in patients complaining of severe burning pain associated with shinning red skin. In 1872, he referred to this condition as ‘Causalgia’, where the pain exceeded what is expected from the inciting injury [2]. In 1900, a Hamburg surgeon Paul Sudeck described the clinical and radiological findings of a painful condition with spotty decalcification in x-rays which later received the name Sudeck’s atrophy [3,4]. French neurosurgeon Rene Leriche believed, that the syndrome was caused by increased activity of the sympathetic nervous system and introduced a surgical periarterial sympathectomy in 1916 [5]. In 1946, James A. Evans, Massachusetts physician, described patients experiencing intense suffering associated with abnormalities of the sympathetic nervous system, and referred to the condition as ‘reflex sympathetic dystrophy [6-8]. The condition has been also described under the term Algodystrophy [9]. The term Complex Regional Pain Syndrome has been in use since the early nineties. CRPS is a chronic neurological condition, usually involving the limbs, that is characterized by severe pain along with sensory, autonomic, motor and trophic involvement. The condition may be induced following surgery, trauma or without an obvious cause. The course may vary from mild and self-limiting to severe, chronic and disabling. CRPS is classified into types I and II based on absence or presence of identifiable nerve injury [10]. The epidemiology, pathophysiology and treatment has been reviewed by Goh et al. [10]. Multiple other recent reviews on the subject have been published [11-16].
Case 1
A 43-year-old male was admitted with fever, left leg erythema, spontaneous bleeding from left leg (Figure 1a,b) and excruciating pain. The pain was described as similar to pouring gasoline on the leg and lighting a match. He will not let anyone touch the leg. He will only let debridement of clotted blood on the leg under anesthesia. This was one of several hospital admissions for the same complaint. The patient stated that, he had the problem since age 17 after having multiple lower extremity orthopedic procedures. According to the mother, he had 13 nerve blocks for the right knee and 10 nerve blocks for the left leg and 1 epidural block without much relief. He was opiate dependent. He had a history of Methicillin Resistant Staphylococcus Aureus (MRSA) infections in the past. The admission temperature was 102.5 Fahrenheit (F), pulse 96/minute, respiratory rate 18/ minute and blood pressure 130/59. He was obese, left leg was erythematous with blood oozing and blood clots attached to the leg. The patient was bed-ridden with an indwelling Foley catheter. The White Blood Cell Count (WBC) was 18,900 (NL 4500-11,000). Cultures from the leg grew MRSA and Group B Streptococcus. He also had a catheter related enterococcal UTI. During this admission he had debridement of blood clots stuck to his leg under anesthesia and intravenous vancomycin. The fever subsided in 4 days and he was discharged after 6 days. He has received multiple courses of antibiotics for associated cellulitis in the past. With each admission, he stays in the hospital for about 1-2 weeks.
Case 2
A 58-year-old male with the history of CRPS type 2 following a vehicular accident 16 years ago, failed sympathectomy and history of an intrathecal hydromorphone (dilaudid) pump for pain relief, was admitted with a draining sinus in the anterior left abdominal wall. A computerized tomogram revealed a calcified fluid filled mass at the site (Figure 2). This was a former implanted morphine pump site which had been in place for 5 years and then removed. This was treated with Alcohol sclerotherapy and drain placement by interventional radiology. A week later, the patient was admitted to the hospital with a temperature of 101F, WBC 11,700 and the fluid from JP drain grew methicillin susceptible Staphylococcus aureus, Enterococcus faecalis and group B Streptococcus. The patient was penicillin allergic and was treated with intravenous vancomycin. He did not improve and repeated cultures grew Citrobacter freundii and Escherichia coli. The antibiotic was changed to ertapenem. The infected calcified mass was surgically excised. The wound healed in about 1 month.
Discussion
Complex regional pain syndrome is a devastating painful condition, most often involving a limb associated with neuropathic pain, autonomic dysfunction, sensory and motor abnormalities and trophic changes [4]. Patients with persistent pain become narcotic dependent often resulting in life long disability. Both patients reported, were narcotic dependent for many years. Most patients with autonomic dysfunction develop erythema in affected limb due to vasodilatation. We have not seen reports of actual bleeding due to bursting of blood vessels as in case 1. Recurrent infections are uncommon, which was seen in in both our cases.
Therapy of CRPS involves a multidisciplinary approach including invasive and noninvasive methods. Noninvasive methods include pharmacotherapy, physical and occupational therapy and psychological therapy. Pharmacotherapy depends on symptoms and includes treatment of neuropathic pain, free radical scavengers, steroids and agents interfering with bone metabolism. Invasive methods include spinal cord stimulators, opioid therapy (implanted morphine pumps, intrathecal pumps), sympathetic blocks and sympathectomy [10]. After failure of multiple modes of intervention, extreme cases of intractable pain and disability have ended in limb amputations [17-19]. More than 100 such cases have been reported [17-19].
References
- Shim H, Rose J, Halle S, Shekane P. Complex regional pain syndrome: A narrative review for the practicing clinician. B J A. 2019; 123: e424-e433.
- Mitchell SW. Injuries of Nerves and their Consequences. JB Lippincott. Philadelphia. 1872; 377.
- Sudeck P. Ueber die akute entzündliche knochenatrophie. Arch F Klin Chir. 1900; 62: 147.
- Sudeck P. Acute (trophoneurotic) osseous atrophy after inflammation and traumas of the extremities. Dtsch Med Wochenschr. 1902; 28: 336-338.
- Leriche R. De la causalgie envisageée comme une neévrite du sympathique et de son fraitment par la deénudationet l’excision des plexus nerveux peériarte riels. Presse Mée. 1916; 24: 178- 180
- Evans JA. Reflex sympathetic dystrophy. Surg Gynecol obstet. 1946; 82: 36-43.
- Evans JA. Sympathectomy for reflex sympathetic dystrophy. JAMA. 1946; 132: 60-623.
- Evans J. Reflex sympathetic dystrophy. Report on 57 cases. Ann Int Med. 1947; 26: 417-426.
- Doury PC. A spectrum of disease Algodystrophy. historical perspectives, criteria of diagnosis, and principles of treatment. Hand Clin. 1997; 13: 327-337.
- Goh EL. Chidambaram S, Ma D. Complex Regional Pain Syndrome: A Recent Update. Burns Trauma. 2017; 5: 2-21.
- Maihofner C, Seifert F, Markovic K. Complex Regional Pain Syndromes: New Pathophysiological concepts and therapies: Eur J Neurol.2010; 17: 649-660.
- Borchers AT, Gershwin ME. Complex Regional Pain Syndrome: A comprehensive and critical review; Autoimmune Rev: 2014; 13: 242-265.
- Bruehl S. Complex regional pain syndrome. BMJ. 2015; 29: h2730.
- Neumeister MW, Romanelli M R. Complex regional pain syndrome. Clin Plast Surg. 2020; 47: 305-310.
- Urits I, Shen A H, Jones MR, Wiswanath O, et al. Complex regional pain syndrome, Current concepts and treatment options. Curr Pain Headache Rep. 2018; 22: 10.
- Kessler A, Yoo M, Calisoff R. Complex regional pain syndrome: An updated comprehensive review. Neuro Rehabilitation. 2020; 47: 253-264.
- Bodde MI, Dijkstra PU, den Dunnen WF, Geertzen JH, Therapy -resistant complex regional pain syndrome type I:to amputate or not. J Bone Joint Surg Am. 2011; 93: 1799-1805.
- Bodde MI, Dijkstra PU, Schrier E, van den Dungen JJ, den Dungen WF, et al. Informed decision-making Regarding Amputation for Complex Regional Pain Syndrome Type I. J Bone Joint Surg Am. 2014; 96: 930-934
- Midbari A, Suzan E, Adler T, Melamed E, Norman D, et al. Amputation in patients with complex regional pain syndrome: A comparative study between amputees and non-amputees with intractable disease. Bone Joint J. 2016; 98: 548-554.