
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
High risk of delayed or missed diagnosis of mucinous appendiceal neoplasm by transvaginal ultrasound: A case series
Francesca Rizzello1,*, Giulia Vannucci2; Maria Elisabetta Coccia3
1 Assisted Reproductive Technology Centre, Careggi University Hospital, Florence, Italy.
2 University of Florence, Florence, Italy
3 Department of Biomedical, Experimental and Clinical Sciences “Mario Serio”, University of Florence, Florence, Italy
*Corresponding Author: Francesca Rizzello
Assisted Reproductive Technology Center, Careggi
Hospital, University of Florence, Largo Brambilla 3,
50134 Florence, Italy.
Email: francesca.rizzello@gmail.com
Received : Apr 27, 2021
Accepted : Jun 01, 2021
Published : Jun 04, 2021
Archived : www.jcimcr.org
Copyright : © Rizzello F (2021).
Abstract
Appendiceal Neoplasm is a rare tumour with a vague and nonspecific clinical presentation. Delayed or missed diagnosis could result in mucin spill into the peritoneal cavity because of cancer infiltration or spontaneous rupture of appendix. This condition is called Psuedomyxoma Peritonei (PMP) and has a very poor prognosis if not treated properly. We present 4 cases of Appendiceal Neoplasm misdiagnosed as adnexal masses of different origin: Dermoid cyst of the right ovary; stump of the previously removed tube; ectopic pregnancy; ovarian malignancy. It is important for gynaecologists to recognize mucinous appendiceal neoplasm in the differential diagnosis of right adnexal masses in order to reduce the risk of misdiagnosis.
Keywords: Appendiceal Neoplasm, Adnexal Masses, Transvaginal Ultrasound, Misdiagnosis.
Abbreviations: AMK: Appendiceal Mucocele; PMP: Psuedomyxoma Peritonei; TV-US: Transvaginal Ultrasound; COC: Combined Oral Contraceptive; IVF-ICSI: In Vitro Fertilisation Intracytoplasmic Sperm Injection; ICSI-ET: Intracytoplasmic Sperm Injection/Embryo Transfer; B-HCG: Beta Human Chorionic Gonadotropin; CT: Computed Tomography; HIPEC: Hyperthermic Intraperitoneal Chemotherapy; CEA: Carcinoembryonic antigen (CEA); CA19-9: Carbohydrate Antigen 19- 9; CA125: Cancer Antigen 125; αFP: Alpha-Fetoprotein; Ca72.4: Cancer Antigen 72.4; Ca 15-3: Cancer Antigen 15-3; IOTA: International Ovarian Tumor Analysis.
Citation: Rizzello F, Vannucci G, Coccia ME. High risk of delayed or missed diagnosis of mucinous appendiceal neoplasm by transvaginal ultrasound. A case series. J Clin Images Med Case Rep. 2021; 2(3): 1185.
Introduction
Appendiceal Mucocele (AM) was described for the first time by Rokitansky in 1842 and later defined by Feren in 1976 [1]. AM is an abnormal dilatation of the appendiceal lumen due to an abnormal production and accumulation of mucus. Appendiceal neoplasms are rare tumours mostly diagnosed incidentally during surgeries performed for appendicitis, accounting for 0.5%-1.0% of appendectomy specimens [2]. Clinical presentation is often vague and non-specific. Sometimes patients might show abdominal pain or a pelvic palpable mass mimicking adnexal pathology. Delayed or missed diagnosis could result in mucin spill into the peritoneal cavity because of cancer infiltration or spontaneous rupture of appendix. This condition is called Psuedomyxoma Peritonei (PMP) and has a very poor prognosis if not properly treated.
In this case series, we aimed to highlight the common features of appendiceal neoplasms at transvaginal ultrasound (TVUS), and the possible differential diagnoses in the gynaecological setting.
Case presentation
Case 1
A 33 years old woman was referred to the Assisted Reproductive Technology Centre for a primary infertility. During controlled ovarian stimulation for IVF-ICSI a right adnexal mass was diagnosed. The mass was described as a bilocular formation sized 62 X 42 X 47 mm. The mass was located anteriorly to the medial surface of the right ovary and showed a mixed hypohyper echogenicity, with no vascularisation. A dermoid cyst of the right ovary was firstly suspected (Figure 1).

In the same year she underwent surgery. An appendiceal mass was revealed instead of the adenexal one and a standard appendicectomy was performed. Histopathology revealed Low grade Appendiceal Mucinous Neoplasm. The patient did not report any problem in a three-year follow-up after surgery.
Case 2
A 39 years old woman was referred to the Assisted Reproductive Technology for a secondary infertility. Her medical history included a right salpingectomy because of hydrosalpinx. During TV-US a unilocular mass with mixed echogenic content, sized 46 X 28 mm was detected near the right ovary. Furthermore, an anechoic unilocular mass of 51 mm diameter was detected close to the left ovary. A stump of the previously removed right tube was firstly hypotized.
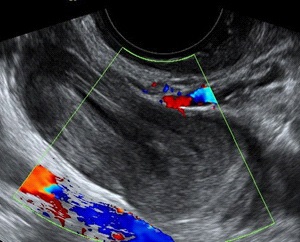
The patient was prescribed Combined Oral Contraceptive (COC) and then TV-US was repeated after two menstrual periods. Two months later, due to the persistence of the adnexal masses a laparoscopic surgery was proposed. A laparoscopic surgery with a left salpingectomy was performed in another hospital three months later. Laparoscopy was performed by a team of gynecologists who did not observe any right adnexal pathology. The appendix was probably not studied. Therefore the patient returned to our clinic to continue the infertility treatment. During TV-US the same right mass was observed. It measured 53 X 25 mm and was described as uniloculare cyst with inhomogeneous content, “onion skin” like (Figure 1). The patient underwent a second surgery for laparoscopic appendicectomy. Appendiceal Mucinous Neoplasm was diagnosed after the histopathological examination.
Case 3
A 47 years woman underwent treatment by Intracytoplasmic Sperm Injection/Embryo Transfer (ICSI-ET) using her husband's sperm and donor eggs. Due to the occurrence of menstrual-like bleeding, the patient did not perform the serum beta hCG levels as scheduled. The patient presented to our centre lamenting the occurrence of right lower quadrant abdominal pain. She was submitted to a pregnancy test and a TV-US. Pregnancy test was positive and a right mass measuring 47 X 23 mm with in homogeneous content constituted by echogenic layers arranged like a circle (onion-skin like echogenicity) was observed at TV-US. An ectopic pregnancy was suspected (Figure 2). B-hCG was tested again but showed negative. Also serum tumor markers CEA, CA19-9, CA125, CYFRA21, αFP, Ca72.4, Ca 15-3 were negative. She underwent a Computed Tomography (CT) of the abdomen and pelvis. The mass was described with water-like content and continuing with the cecum. The patient underwent laparoscopic surgery. An appendiceal mass was observed and a standard appendicectomy was performed. Bilateral adenexa were normal. A Low Grade Appendiceal Mucinous Neoplasm was the histopathological diagnosis.

Case 4
A 48 years old woman presented to the emergency department with mild abdominal pain and severe bloating that occurred suddenly. An abdominal ultrasound showed ascites and a right multilocular mass with multiple locules measuring 25cm. (Figure 4). The abdominal CT confirmed ascites, a right formation with multiple locules sized 28x20cm and an omental thickening. CEA, CA 19.9 and CA 125 showed increased. An ovarian malignancy was firstly suspected. She underwent surgery and bilateral adnexectomy, appendicetomy and omentectomy were performed. The histopathological diagnosis was appendicolar mucinous adenocarcinoma with infiltration. Cytoreductive surgery, with right hemicolectomy and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) were then performed.

Discussion
AM is an abnormal dilatation of the appendiceal lumen due to an abnormal production and accumulation of mucus. The term appendiceal mucocele is outdated and nowdays the term Mucinous Appendiceal Neoplasm is used. Appendiceal Neoplasm is an infrequent tumor with an incidence of 0.2% - 0.7% in appendiceal pathologies [3]. It is more frequent among the female population aged 50 years or more. The clinical presentation is often vague and non-specific.
The patients with appendiceal neoplasm are asymptomatic or may present chronic or acute pain in the right lower abdomen often mistaken with appendicitis. Sometimes the patients could have a pelvic palpable mass miming adenexal pathology in women.
Ultrasonography (US) and Computed Tomography (CT) can be used to detect appendiceal neoplasm. CT scan is considered the gold standard with an accuracy rate of 87.7% [4].
Appendiceal neoplasm studied on US is defined by some features: diameter larger than 1,5 cm, “onion skin” appearance, nodular enhancing of wall [5]. RMI is superior in studying peritoneal lesions. PET is not indicated. Once a lesion is detected by imaging, Colonscopy is indicated in order to analyse other appendiceal/colonic lesions. However the definitive diagnosis is histopathological. Tumor markers as CEA, CA 19-9 and CA 125, are not specific but could be useful in terms of prognosis. Elevated levels at the time of appendicectomy indicate an increased risk of recurrence or death [6].
TV-US allows the recognition of numerous adnexal masses with high specificity and sensitivity [7]. However, some findings remain not clearly attributable and may lead to mismanagement. Masses originating from the appendix are included in these cases.
Furthermore, although pelvic masses are often managed in the gynaecological setting, gynaecologists does not have the expertise to recognize the masses of appendicular origin. Actually International Ovarian Tumor Analysis (IOTA) does not include the ‘Onion-Skin’ pattern among terms and definitions to describe the sonographic features of pelvic masses [7].
In our case series Appendiceal Mucinous Neoplasms were misdiagnosed with dermoid cyst; stump of a previously removed tube; ectopic pregnancy; ovarian malignancy.
The delayed or missed diagnosis could result in mucin spill into the peritoneal cavity because of cancer infiltration or spontaneus rupture of appendix. It is called Pseudomyxoma Peritonei (PMP) and is correlated with a bad prognosis if not treated properly [8]. However the prognostic significance of PMP is different considering the level of cellularity within the mucin [9].
Modality of treatment and follow-up is still not standardized. Standard appendicectomy is the initial procedure. Laparoscopic approach and open surgery could be both used even if the use of laparoscopy is controversial. An histopathological diagnosis of adenocarcinoma should result in subsequent right hemicolectomy [10]. In case of PMP, cytoreductive surgery, chemotherapy and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) are indicated [11,12].
The prognosis of appendiceal neoplasm is correlated to the histology and to tumor progression in PMP. Without this progression, the 5-year survival of the benign form is almost 100%, while that of the malignant forms varies from 30 to 80% [13,14]. The 5 years survival for PMP varies from 23 to 77% [3,15].
Conclusions
Appendiceal mucinous neoplasm is a rare form of pathology. A timely preoperative diagnosis is difficult due to its non-specific symptoms and its high risk of misdiagnosis as adnexal mass. This may delay surgical intervention and may lead to spontaneous rupture with prognostic worsening. Thus, it is important for gynaecologists to know that mucinous appendiceal neoplasm should be considered in the differential diagnosis of adenexal masses in order to decrease delayed and advanced diagnosis. An appropriate and updated ultrasound training on this pathology should be performed by gynaecologists.
References
- Idris LO, Olafe OO, Adejumobi OM, Kolawole AO, Jimoh AK. Giant mucocele of the appendix in pregnancy: A case report and review of literature. Int J Surg Case Rep. 2015, 9: 95–97.
- Pickhardt PJ, Levy AD, Rohrmann CA, Kende AL. Primary neoplasms of the appendix: Radiologic spectrum of disease with pathologic correlation. Radiographics. 2003; 23: 645-62.
- Rymer B, Forsythe RO, Husada G. Mucocoele and mucinous tumours of the appendix: A review of the literature. Int J Surg. 2015. 18:132–135.
- Kwak HD, Ju JK. A prospective study of discrepancy between clinical and pathological diagnosis of appendiceal mucinous neoplasm. Ann Surg Treat Res. 2020; 98: 124–129.
- Kameda T, Kawai F, Taniguchi N, Omoto K, Kobori Y, Arakawa K. Evaluation of whether the ultrasonographic onion skin sign is specific for the diagnosis of an appendiceal mucocele. Journal of Medical Ultrasonics. 2014, 41: 439–443.
- Overman MJ, Compton CC, Raghav K, Lambert LA. Appendiceal mucinous lesions. UpToDate. 2020.
- Timmerman D, Valentin L, Bourne TH, Collins WP, Verrelst H, Vergote I and Group, International Ovarian Tumor Analysis (IOTA). Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound Obstet Gynecol. 2000; 16: 500-505.
- Morano WF, Gleeson EM, Sullivan SH, Padmanaban V, Mapow BL, et al. Clinicopathological features and management of appendiceal mucocele: A systematic review. Am Surg. 2018; 84: 273–281.
- Misdraji J, Carr NJ, Pai RK. Appendiceal serrated lesions and polyps. WHO Classification of Tumours: Digestive System Tumours. 5th ed. WHO Classification of Tumour Editorial Board (Ed), IARC. 2019; 141.
- Valasek MA, Pai RK. An update on the diagnosis, grading, and staging of appendiceal mucinous neoplasms. Adv Anat Pathol. 2018; 25: 38–60.
- Milovanov V, Sardi A, Ledakis P, et al. Systemic chemotherapy (sc) before cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (crs/hipec) in patients with peritoneal mucinous carcinomatosis of appendiceal origin (pmca). Eur J Surg Oncol. 2015; 41: 707–712.
- Chua TC, Moran BJ, Sugarbaker PH, et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J Clin Oncol. 2012; 30: 2449–2456.
- Matias-García B, Mendoza-Moreno F, Blasco-Martínez A, Busteros-Moraza JI, Diez-Alonso M, et al. A retrospective analysis and literature review. BMC Surg. 2021; 21: 79.
- Rouchaud A, Glas L, Gayet M, Bellin MF. Appendiceal mucinous cystadenoma. Diagn Interv Imaging. 2014; 95: 113–116.
- Fish R, Renehan AG, Punnett G, Aziz O, Fulford P, et al. Referral and treatment pathways for pseudomyxoma peritonei of appendiceal origin within a national treatment programme. Colorectal Dis. 2018; 20: 888–896.