
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Patients with acute respiratory distress syndrome due to pandemic Coronavirus disease 2019 (COVID-19)
Julia Seeger1; Volker Wenzel2; Jochen Wöhrle1*
1 Division of Nephrology, National University Health System, Singapore.
2 Medical Campus Lake Constance, Department of Anaesthesiology, Friedrichshafen, Germany.
*Corresponding Author: Jochen Wöhrle
Head, Department of Cardiology and Intensive Care
Unit, Medical Campus Lake Constance Klinikum
Friedrichshafen, Germany.
Email: j.woehrle@klinikum-fn.de
Received : Apr 30, 2021
Accepted : Jun 02, 2021
Published : Jun 07, 2021
Archived : www.jcimcr.org
Copyright : © Wöhrle J (2021).
Abstract
We report on a case study of patients with Coronavirus disease 2019 (COVID-19). Evaluation of factors predicting outcome in patients with COVID-19 are very important. Both patients developed respiratory failure complicated by acute respiratory distress syndrome. Patients were intubated and invasively ventilated, underwent prone positioning and careful ventilation according to criteria for acute respiratory distress syndrome. In addition, biomarkers were daily evaluated including C-reactive protein, d-dimer and high-sensitive troponin T. Although treatment did not differ between patients, one patient survived whereas the other one died. The patient who survived had a faster onset of invasive ventilation with prone positioning, a lower maximal level of C-reactive protein and a lower value of high-sensitive troponin T. The use of mechanical ventilation in combination with a high PEEP and an early start of prone positioning in patients with severe ARDS may be beneficial. The values of C-reactive protein and troponin T levels seems to be predictive for the clinical course.
Keywords: Coronavirus disease 2019; COVID-19; Troponin; C-reactive protein; Mechanical ventilation.
Citation: Seeger J, Wenzel V, Wöhrle J. Patients with acute respiratory distress syndrome due to pandemic Coronavirus disease 2019 (COVID-19). J Clin Images Med Case Rep. 2021; 2(3): 1187.
Introduction
In December 2019, a Coronavirus disease 2019 (COVID-19) pandemic started in China [1]. Severe complications including pneumonitis, respiratory failure, and Acute Respiratory Distress Syndrome (ARDS) were the main causes of death due to pandemic COVID-19 infection [2-4]. In an early study the antiviral treatment with lopinavir and ritonavir did not show a benefit beyond standard of care [5]. Remdesivir, a nucleotide analogue prodrug that inhibits viral RNA polymerase, showed clinical improvement in 36 of 53 patients with COVID-19 infection [6]. The combination of baricitinib plus remdesivir was superior to remdesivir alone in reduction recovery time and accelerating improvement in clinical status among patients with COVID-19 [7]. In majority of hospitals dealing with COVID-19 ARDS patients the supportive treatment includes lung-protective invasive ventilation with early start of prone positioning, antibiotics to avoid or to treat bacterial superinfection, and careful analysis of laboratory values. C-reactive protein as well as troponin have been linked to a worse prognosis of patients with COVID-19 [8-10].
Case study
We report on two patients with severe Acute Respiratory Distress Syndrome (ARDS) due to pandemic COVID-19 infection and testing of inflammatory and ischemic parameters. The first patient was a 63-year-old man with known insulin dependent diabetes mellitus and arterial hypertension. Onset of symptoms, i.e. fever, dyspnoea, cough, headache, and myalgias, was 12 days before admission to our Intensive Care Unit (ICU). ICU admission was necessary due to rapid respiratory deterioration with severe dyspnoea and tachypnoea. Initial oxygen saturation at ambient air was 88%. The patient was intubated with rapid sequence induction and mechanically ventilated, prone positioning was started 90 minutes after intubation.
The second patient was a 71-year-old man with mild nephropathy, arterial hypertension, and a history of smoking. Admission to ICU became necessary because of respiratory deterioration with a breathing frequency of 34 per minute and an oxygen saturation below 88% despite supply of oxygen by nasal probe. Onset of symptoms (cough and dyspnoea) was 10 days before admission to our ICU. There were no oral drug administrations apart from an angiotensin-converting enzyme inhibitor in patients 1 and a calcium antagonist in patient 2. Echocardiography demonstrated a normal Left Ventricular (LV) function in the first patients and a mildly reduced LV function in patient 2.
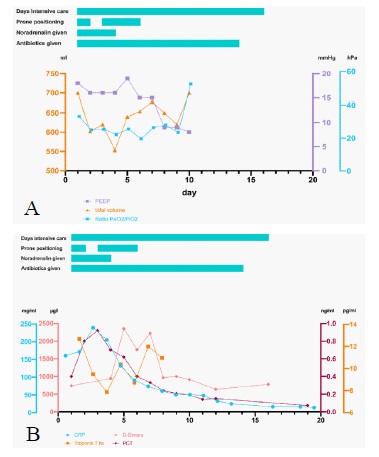
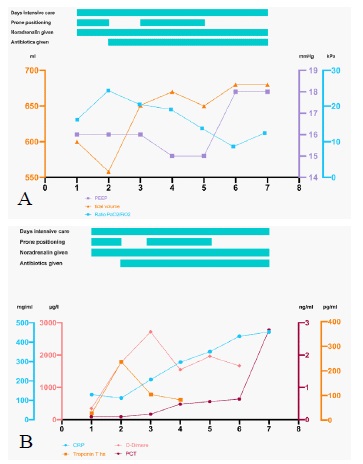
Diagnosis of Coronavirus disease 2019 (COVID-19) by realtime Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR) performed from a throat swab specimen was positive for SARSCoV-2 in both patients. The first patient was intubated with rapid sequence induction and invasively ventilated for 12 days, the second patient was initially non-invasively ventilated with BIPAP (Biphasic Positive Airway Pressure) followed by videolaryngoscopic intubation and invasive ventilation for another 7 days. In both patients there was no evidence for typical or atypical pathogen, tests for influenza type A and B were negative. Patients were treated with lung-protective invasive ventilation with application of ARDS criteria [11,12] and high peep pressure, intravenous antibiotics to treat and avoid bacterial superinfection, vasopressors and were negatively balanced regarding volume status. Prone positioning was started within the first 2 hours after intubation and mechanical ventilation for a total of 16 hours each cycle. In both patients lung protective ventilation with a low tidal volume and a high peep pressure was applied. In both patients the FiO2 could be reduced to 0.5 at day 1-2, but there was an increasingly deterioration in patient 2 with a subsequent FiO2 of 1.0. Ratio of PaO2 /FiO2 , tidal volume as well as PEEP are detailed in Figure 1A for patient 1 and Figure 2A for patient 2. We did not use antiviral treatment, or immunoglobulins or another specific treatment strategy. Urin production ranged from 1500 mL to 7330 mL in patient 1 and 4180 mL to 7560 mL in patient 2. Both patients were on low-dose anticoagulation with unfractionated heparin and received a course of dexamethasone. As detailed in Figure 1B and 2B values of d-dimer ranged from 737-2354 µg/L (peak day 5) in patient 1 and 346- 1960 µg/L (peak day3) in patient 2. Creatine-kinase ranged from 138-1419 U/L (peak day 7) in patient 1 and 257-1858 U/L (peak day 6) in patient 2. Maximal value of high-sensitive troponin T was 11,5 pg/mL (peak day 2) in patient 1 and 287 pg/mL (peak day 2) in patient 2. Peak C-reactive protein was 222 mg/L (peak day 3) in patient 1 and continuously declined starting at day 3, while C-reactive protein continuously increased in patient 2 up to 441 mg/L (final day). Procalcitonin values increased up to 0.92 ng/mL in patient 1 at day 3 and continuously increased in patient 2 up to 2.78 at day 7 (last day). Course of lab values are depicted in Figure 1B and 2B.
While in patient 1 vasopressors could be stopped at day 4 after intubation, there was a subsequent higher need to maintain the circulation in septic shock of patient 2. In addition, empirical antimicrobial therapy with broad-spectrum antibiotics was initiated after ICU admission in both patients. Patient 1 was extubated after clinical improvement after 11 days of mechanical ventilation, patient 2 experienced a clinical deterioration with hemodynamic instability and increasing vasopressor doses and died 7 days after initiation of mechanical ventilation.
Discussion
We report on two cases with COVID-19 infection and severe ARDS. Although supportive treatment was identical, only one patient survived. Mortality rate in patients requiring intensive care unit support or mechanical ventilation with COVID-19 infection has been reported to be high. In a series of 24 patients from the Seattle Region 75% of patients needed mechanical ventilation and mortality rate was 50% [3]. In an early series of 191 patients from China [2], 54 patients (28.3%) died. Apart from age a d-dimer value greater than 1 ug/mL on admission was associated with a higher risk of in-hospital death. In a series of 1099 patients from China overall rate of death was 1.4% with a need for intensive care unit therapy in 5.0% [4]. Focusing on critically ill patients who were admitted to the ICU, mortality rate was 61.5% (32 out of 52 patients) [13]. In this series patients suffered from liver dysfunction in 29%, pneumothorax in 2%, acute kidney injury in 29%, cardiac injury in 23%, ARDS in 67% and hospital-acquired infection in 13.5%. In a meta-analysis [14] 20.3% of patients required intensive care unit, 32.8% presented with ARDS and 6.2% with shock. Mortality rate was 13.9% in the whole study population of 656 patients [14]. Other reported complications are acute pulmonary embolism [15] in a patient with absence of major predisposing factors or cardiac tamponade complicating myo-pericarditis in a COVID-19 patient [16]. Our two patients did not experience pericardial effusion, pulmonary embolism or pneumothorax. Both patients suffered from severe ARDS. In patient 2 cardiac injury due to septic shock was demonstrated by an elevated high-sensitive troponin T level which has been linked to an increased risk of mortality [8-10]. Anticoagulation with low-dose unfractionated heparin was used in both patients to avoid thrombotic complications. Both patients had severe septic shock, were treated with vasopressors and experienced respiratory failure with subsequent need for mechanical ventilation.
There is an ongoing discussion in the medical field whether to postpone mechanical ventilation. Reasons triggering this discussion might be that the mortality of patients with respiratory failure and need for mechanical ventilation is very high. In our patient 1 intubation with rapid sequence induction and mechanical ventilation was started soon after respiratory deterioration at a very low Horowitz Index whereas in patient 2 the respiratory failure initially aimed to be adressed by non-invasive ventilation inhibiting the early start of prone positioning. Prone positioning with a prone duration greater than 12 h/d in patients with ARDS has been linked to an improved survival [11,12]. We recommend not to postpone intubation and mechanical ventilation but rather to initiate appropriate use of invasive mechanical ventilation which subsequently allows an early start of prone positioning. A delayed start of prone positioning, as in patient 2, was associated with an inferior outcome.
Apart from ventilation, both cases did differ in course of Creactive protein which is a good prognostic marker of COVID-19 patients in combination with troponin T, and other thromboinflammatory biomarkers such as D-dimer, fibrinogen, ferritin, and interleukin 6 [10]. Both patients experienced symptoms 10-14 days prior to respiratory failure, which is in line with previous publications showing that respiratory failure may occur 7-14 days after infection with COVID-19 [14]. Concomitant dis- Concomitant dis- Concomitant dis Concomitant diseases were arterial hypertension in both patients as well as Type II diabetes in patient one, thus both typical cardiovascular risk factors. In a series of 54 mortality cases of COVID-19 from the Republic of Korea age (< or > 70 years old) as well as presence or absence of underlying illness was associated with a similar duration between symptom onset to death [17]. In a series of 85 fatal cases most patients died of multiple organ failure [18] with 81% of patients suffering from shock and 74% from ARDS.
We did not use antiviral treatment, immunoglobulins or other specific treatment strategies, since no specific treatment has been clearly proven to be beneficial at the timepoint of treatment. In an early randomized trial, the use of lopinavirritonavir in adults with severe COVID-19 infection was studied [5]. With randomization of 199 patients mortality rate after 28 days was 19.2% in the lopinavir-ritonavir group versus 25.0% in the standard-care group with no statistical difference. Compassionate use of remdesivir, a nucleotide analogue prodrug that inhibits viral RNA polymerases, has been linked to a clinical improvement in 68% (36 of 53 patients) [6]. Indication for compassionate use of remdesivir was an oxygen saturation of 94% or less with ambient air or oxygen support. Thirteen percent of patients died after completion of remdesivir treatment. Mortality rate was 18% in patients requiring invasive ventilation. In other series without specific therapy mortality rate of COVID-19 patients with mechanical ventilation was 50% [3] and 62% after admission to intensive care unit [13] which supports the idea that remdesivir may provide benefit in COVID-19 critical ill patients. In a recent published trial 1033 patients were randomized to baricitinib plus remdesivir versus remdesivir. Baricitinib plus remdesivir was superior to remdesivir alone in reducing recovery time and accelerating improvement in clinical status among patients with Covid-19 [10]. The 28-day mortality was 5.1% in the combination group and 7.8% in the control group (hazard ratio for death, 0.65; 95% CI, 0.39 to 1.09). Serious adverse events were less frequent in the combination group than in the control group (16.0% vs. 21.0%; difference, -5.0 percentage points; 95% CI, -9.8 to -0.3; P =0.03), as were new infections (5.9% vs. 11.2%; difference, -5.3 percentage points; 95% CI, -8.7 to -1.9; P=0.003).
Inflammatory and ischemic parameters have the potential to predict the clinical course of patients with ARDS due to COVID-19 infection. Apart from a specific therapy use of mechanical ventilation in combination with a high PEEP and an early start of prone positioning in patients with severe ARDS should be applied.
References
- Li Q, Guan X, Wu P, Wang X, Zhou L, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020; 382: 1199-1207.
- Zhou F, Yu T, Du R, Fan G, Liu Y, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020; 395: 1054- 1062.
- Bhatraju PK, Ghassemieh BJ, Nichols M, Kim R, Jerome KR, et al. Covid-19 in critically ill patients in the Seatlle region – case series. N Engl J Med. 2020; 382: 2012-2022.
- Guan W, Ni Z, Hu Y, Liang W, Ou C, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708-1720.
- Cao B, Wang Y, Wen D, Liu W, Wang J, et al. A trial of lopinavirritonavir in adults hospitalized with severe Covid-19. N Engl J Med. 2020; 382: 1787-1799.
- Grein J, Ohmagari N, Shin D, Diaz G, Asperges E, et al. Compassionate use of remdesivir for patients with severe Covid-19. N Engl J Med. 2020; 382: 2327-2336.
- Kalil AC, Patterson TF, Mehta AK, Tomashek KM, Wolfe CR, et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med. 2021; 384: 795-807.
- Ali J, Khan FR, Ullah R, Hassan Z, Khattak S, et al. Cardiac Troponin I Levels in Hospitalized COVID-19 Patients as a Predictor of Severity and Outcome: A Retrospective Cohort Study. Cureus. 2021; 13: e14061.
- Mengozzi A, Georgiopoulos G, Falcone M, Tiseo G, Pugliese NR, et al. The relationship between cardiac injury, inflammation and coagulation in predicting COVID-19 outcome. Sci Rep. 2021; 11: 6515.
- Chaudhary R, Garg J, Houghton DE, Murad MH, Kondur A, et al. Thromboinflammatory Biomarkers in COVID-19: Systematic Review and Meta-analysis of 17,052 Patients. Mayo Clin Proc Innov Qual Outcomes. 2021; 5: 388-402.
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017; 195: 1253-1263.
- Griffiths MJD, McAuley DF, Perkins GD, Barrett N, Blackwood B, et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Resp Res. 2019; 6: e000420.
- Yang X, Yu Y, Xu J, Shu H, X J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med. 2020; 8: 475-481.
- Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Pena R, Holguin-Rivera Y, et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Medicine and Infectious Disease 2020; 34: 101623.
- Danzi GB, Loffi M, Galeazzi G, Gherbesi E. Acute pulmonary embolism and COVID-19 pneumonia: A random association?. Eur Heart. J 2020; 41: 1858.
- Hua A, O´Gallagher K, Sado D, Byrne J. Life-threatening cardiac tamponade complicating myo-pericarditis in COVID-19. Eur Heart J. 2020; 41: 2130.
- Korean Society of Infectious Diseases and Korea Centers for Disease Control and Prevention. Analysis on 54 mortality cases of coronavirus disease 2019 in the Republic of Korea from January 19 to March 10, 2020. J Korean Med Sci. 2020; 35: e132.
- Du Y, Tu L, Zhu P, Mu M, Wang R, et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan: A retrospective observational study. Am J Respir Crit Care Med. 2020; 201: 1372-1379.