
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Can I have epidural analgesia if I have tinea versicolor?
Francesca Ciano; Matteo Biancone; Bruno Antonio Zanfini*; Stefano Catarci; Gaetano Draisci
1 Department of Emergency, Anesthesiological and Reanimation Sciences, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Largo A. Gemelli 8 00168, Rome, Italy.
*Corresponding Author: Bruno Antonio Zanfini
Department of Emergency, Anesthesiological and
Reanimation Sciences, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Largo A. Gemelli 8
00168, Rome, Italy.
Email: brunoantonio.zanfini@policlinicogemelli.it
Received : Apr 30, 2021
Accepted : Jun 07, 2021
Published : Jun 10, 2021
Archived : www.jcimcr.org
Copyright : © Zanfini BA (2021).
Citation: Ciano F, Biancone M, Zanfini BA, Catarci S, Draisci G. Can I have epidural analgesia if I have tinea versicolor?. J Clin Images Med Case Rep. 2021; 2(3): 1189.
Introduction
Labor and delivery, while perceived as gratifying and joyful, are nonetheless among the most painful events women can experience in life. Treating pain is nowadays one of the essential elements in assisting women during labor.
Epidural analgesia is the best option to ensure the optimal control of pain for the mother without compromising the wellbeing of the fetus. The main contraindications to neuraxial analgesia techniques include patient refusal, known bleeding diathesis or abnormal coagulation tests, elevated intracranial pressure (particularly in the presence of an intracranial space occupying lesion), severe aortic or mitralic valve stenosis and infections at the puncture site [1].
There are many pathogens responsible for cutaneous infections at the dorsal-lumbar level, yeasts of the Malassetia genus being the most commonly implicated. Malassetia Globulosa is the predominant species in the Tinea Versicolor infection [2,3]. Also implicated are M. Sympodialis, M. Furfur and others as well [4]. These fungi are normal components of the cutaneous flora but the transformation from yeasts to micelia can lead to the pathology. The cause for this occurrence is still unknown, yet there are a few contributing factors leading to this infection that affects mostly adolescents and young adults; these are genetic predisposition [5], heat and humidity, immunosuppression, contraceptives, pregnancy and malnutrition.
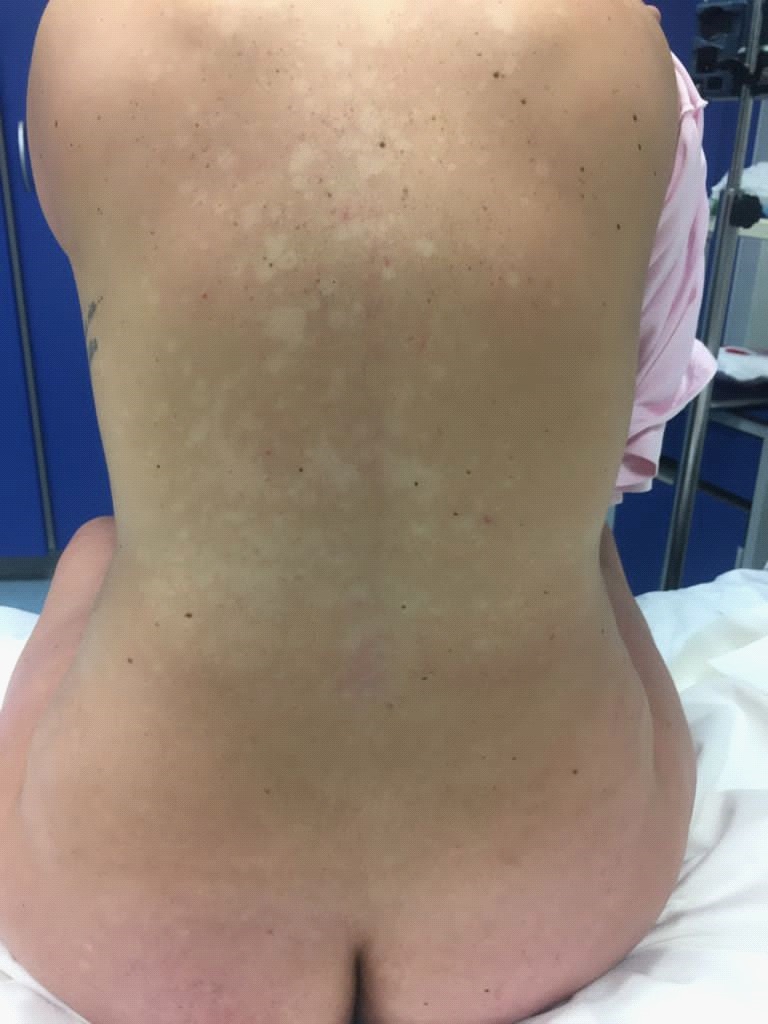
It manifests with characteristic hypo- or hyper-pigmented spots alongside the trunk, the neck, and the face. The majority of the times infection is entirely superficial but cases of meningitis and Central Nervous System (CNS) infections from hematogenous spread have been reported [6,7]. The literature supports with data that adequate antiseptic preparation of the skin effectively prevents meningitis occurrence after epidural puncture [8]; other cases are reported where a small incision of the skin allows for a safer passage of the needle directly in the subcutis without going thnrough the corneal layer.
Case report
A 32 yo primigravida at term (40 w) was admitted in our labor and delivery unit in active labor with painful contractions. The patient was not allergic, her pregnancy was physiologic, and she had a diagnosis of Tinea Versicolor at 36 w by a dermatologist. The patient reported mild truncal pruritus, physical examination of the back showed diffuse hypo-pigmented lesions in dorso-lumbar region. At 4 cm of cervical dilation she asked for epidural analgesia which was administered to her after confirmation of informed consent acquired during the ante-partum anesthesiologic visit at 34 w.
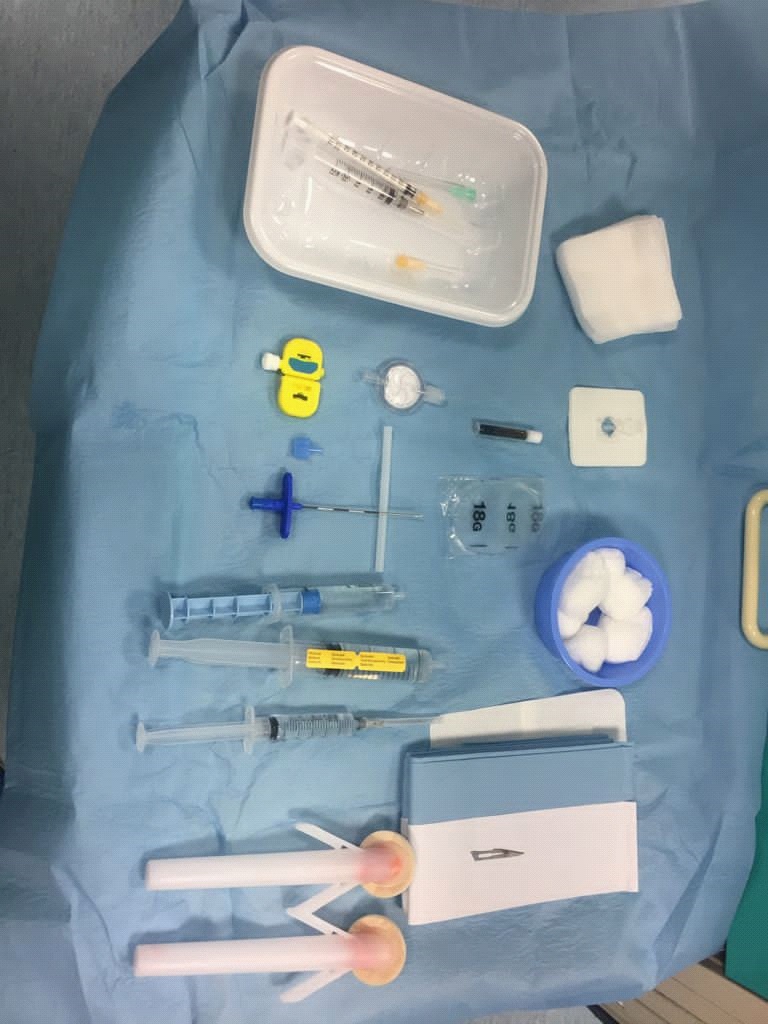
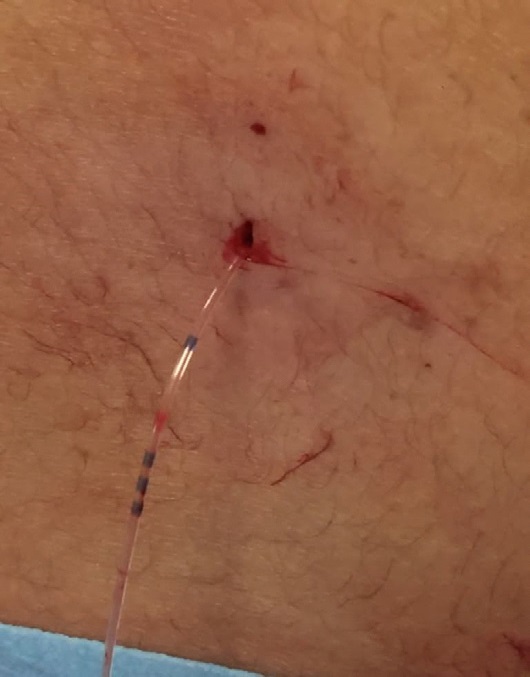
The patient was placed in sitting position and the intervertebral space L3-L4 was identified. After skin disinfection with ChloraprepTM 2%CHG/70% IPA and local anesthesia with Lidocaine 2% 5 ml a small incision of the superficial layer of the skin with a scalpel #11 was performed. The Tuohy 18G needle was then introduced through the subcutis in the epidural space followed by an epidural catheter placement. The skin was sealed with surgical glue and steri-stripes. There were no periprocedural complication.
The patient had a painless uncomplicated vaginal delivery; she and her healthy newborn were discharged home 3 days later. No fever or CNS signs of infection were present. The obstetrical follow-up visit after a month and an anesthesiologic follow-up phone call at 6 months were both negative for neurological issues and the patient reported outcome for the whole procedure was excellent.


Discussion
Fungal encephalitis and meningitis from spinal canal contamination are exceptionally rare but potentially fatal complications following neuraxial blocks [10]. Compared with spinal anesthesia where smaller atraumatic needles are used (usually 25-27G), epidural analgesia technique requires larger gauge cutting needles (18G) which carry along a potential much higher risk of introducing deeply particles of skin and therefore an increased risk of infection.
Epidural analgesia is the golden standard for pain control in labor and delivery. In Italy this procedure is part of the essential level of assistance; in selected hospitals it is guaranteed to all laboring women asking for it, provided that an informed consent is previously acquired in the context of an antepartum anesthesiological visit and that clinical and environmental conditions are safe for the patient at the time of admission in the labor and delivery unit.
This patient had no other contraindications but fungal infection at the epidural puncture site. Literature supporting data account for additional precautions like a prolonged and deep cutaneous disinfection [7] and a small skin incision allowing to insert the needle under the affected corneal layer [9]. No data exist on a clear superiority of a given choice over another; given the potentially poor neurological outcome in case of fungal CNS infection with risk of neurologic sequelae we decided to sum the benefits of the two methods in the aim of obtaining an additional reduction of the infection risk.
Further studies are needed and data collection necessary to define the best procedure for such cases.
Conclusion
In patients with Tinea Versicolor, when a woman in labor asks for epidural analgesia a prolonged deep skin disinfection with Clorexidina + Isopropilic alcohol makes the procedure safe. Lacking RCT excluding every potential risk, performing a small cutaneous incision at the site of puncture allows for corneal layer bypass and can be considered as an extra preventive measure against potential CNS fungal infection.
References
- Morgan & Mikhail’s Clinical Anesthesiology, 5th edition. (Chapter 45).
- Morishita N, Sei Y. Microreview of Pytiriasis versicolor and Malassezia species Mycopathologia. 2006; 162: 373.
- Karakas M, Turaç-Biçer A, Ilkit M, et al. Epidemiology of pityriasis versicolor in Adana, Turkey. J Dermatol. 2009; 36: 377.
- Schwartz RA. Superficial fungal infections. Lancet. 2004; 364: 1173.
- Hafez M, el-Shamy S. Genetic susceptibility in pityriasiss versicolor. Dermatologica. 1985; 171: 86.
- Clark A, Camann W, Mavropoulos A. Epidural analgesia in a parturient with lumbar tinea versicolor. Int J Obstet Anesth. 2013; 22: 265-266.
- Dubar G , Omarjee M, Viguié C, Barbarot S, Mignon A. Analgésie péridurale obstétricale chez une femme ayant un pityriasis versicolor de la région lombaire. Ann Fr Anesth Reanim. 2011; 30: 597-599.
- Turhakia MB, Bauchat J. Combined spinal epidural in a parturient with tinea versicolor. J Clin Anesth 2017; 43: 63-64.
- Reis PV, Mendes LC, Oliveira R. Is Tinea Versicolor a contraindication for epidural analgesia? Minerva anestesiol. 2016; 82: 1019-1021.
- Ritter JM, Muehlenbachs A, Blau DM, Paddok CD, Shieh WJ, et al, Lockhart SR. Exserohilum infections associated with contaminated steroid injections: A clinicopathologic review of 40 cases. AM J Pathol. 2013; 183: 881-892.