
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Dasatinib-induced pleural and pericardial effusion: A case report and review
Siméon Matile1; Jérôme Voegeli2; Gregor John1,3*
1 Department of Internal Medicine, Neuchâtel Hospital Network, Maladière 45, 2000 Neuchâtel, Switzerland.
2 Rue Numa-Droz 187, 2300 La Chaux-de-Fonds, Switzerland.
3 Geneva University, Michel-Servet 1 Geneva, Switzerland.
*Corresponding Author: Gregor John
Department of Internal Medicine, Hôpital neuchâtelois, Maladière 45, 2000 Neuchâtel, Switzerland.
Email: gregor.john@rhne.ch
Received : Apr 12, 2021
Accepted : Jun 17, 2021
Published : Jun 22, 2021
Archived : www.jcimcr.org
Copyright : © John G (2021).
Abstract
Introduction: Tyrosine Kinase Inhibitors (TKI) have dramatically changed the prognostic of chronic myeloid leukemia. However, they have been associated with several side effects.
Case report: We describe a case of a patient admitted for bilateral exudative pleural and pericardial effusions. After a complete work-up, we concluded to a dasatinib-related side effect.
Management and outcome: The patient received oxygen supply, aerosols of ipratropium/salbutamol, and 50 mg of Prednisone for 5 days. The treatment by dasatinib was stopped. She remained asymptomatic at the two-month control by her haematologist. The chest xray showed a small remaining bilateral effusion.
Discussion: Based on this case, we performed a literature review on the subject to give insight on the associated risk factors, treatment options and prognostic. Dasatinib-related pleural effusion is frequent, but most often asymptomatic. Further studies are needed to better understand its mechanism and help guide treatment.
Keywords: Dasatinib; pleural; pericadial; effusion; side effect; case report.
Citation: Matile S, Voegeli J, John G. Dasatinib-induced pleural and pericardial effusion: A case report and review. J Clin Images Med Case Rep. 2021; 2(3): 1193.
Introduction
Chronic Myeloid Leukaemia (CML) is a myeloproliferative disorder of the hematopoietic stem cell caused by a translocation between the BCR and ABL gene. The resulting Philadelphia chromosome (t9; 22) promotes unregulated proliferation of myeloid precursor cells. The incidence of CML is 1-1.5/100’000 per year. Tyrosine Kinase Inhibitors (TKI) have dramatically changed prognostic and treatment of the disease. First generation TKI may result in the development of resistance and intolerance. Amongst second generation TKI, dasatinib is generally well tolerated. However, it has been associated with a higher risk for Pleural Effusions (PE). In this article, we describe a case of bilateral dasatinib-induced pleural and pericardial effusion, summarize available evidence on this condition and propose a management strategy.
Case description
A 59 years old woman known for type 2 diabetes, tobacco related chronic obstructive pulmonary disease and CML, presented to ED for a one-day history of dyspnea at rest, cough and sputum expectoration. She also complained of an interscapular pain. She had no fever, night sweet, weight loss or history of travelling. Her only medication consisted of dasatinib 100 mg daily. At the diagnosis of CML (2016), she started imatinib 400 mg that resulted in major molecular response. However, the treatment had to be discontinued after 8 months because of a facial oedema (very common side effect of imatinib). Then, her medication switched with dasatinib for the last 2.5 years.
On admission, the patient was tachypneic (20 breaths/min), tachycard (110 beats/min), her blood pressure was 127/82 mmHg, her temperature 37.1°C and oxygen saturation was 85% on room air. Pulmonary auscultation revealed wheezing and bibasal hypoventilation. There was no leg oedema or hepatojugular reflux. The cardiac examination was unremarkable. We excluded enlarge liver, spleen, or lymph nods.
The laboratory showed a leucocytosis (13.2 G/l) and a modestly elevated C-reactive protein (31 mg/l), but no renal or hepatic dysfunction and an unraised NT-proBNP (90 ng/l). The chest CT-scan confirmed the bilateral pleural effusion and a 1 cm large pericardial effusion. The transthoracic echocardiography revealed no sign of compression and a normal ventricular function. Thoracocentesis retrieved 1.5 liters of an exudative pleural liquid (2 /3 Light’s criterias: Pleural LDH=181 U/l, plasma LDH=181 U/l (ratio>0.6), pleural protein=47 g/l, plasma protein=71 g/l (ratio>0.5)). The liquid was predominantly lymphocytic (6170 cells, 97% of lymphocytes, 3% of polymorphonucleated cells). The analysis showed a negative adenosine deaminase assay, no bacterial growth, no malignant cells on cytology, and no argument for a chylothorax. The BCR-ABL was undetectable (major molecular response).
We concluded to a dasatinib-induced bilateral pleural and pericardial effusion. The final Naranjo score is then calculated at 7 points, making the adverse drug reaction probable. Thus, the patient received oxygen supply, aerosols of ipratropium/ salbutamol, and 50 mg of Prednisone for 5 days. The treatment by dasatinib was stopped. The clinical evolution was good after the thoracentesis, without any further needs of oxygen supply or new thoracocentesis. The patient could leave the hospital after 3 days.
She remained asymptomatic at the two-month control by her haematologist. The chest x-ray showed a small remaining bilateral effusion. In the end, nilotinib treatment never started, because BCR-ABL was still undetectable. Instead, it was decided to monitor her BCR-ABL transcript levels.
Discussion
TKI have changed the prognostic of CML but have also been associated to several important side effects. The case illustrates a bilateral pleural and pericardial effusion under dasatinib. To collect information on prevalence, risk factors, treatment strategy and prognosis, we performed a literature search in Medline using the keywords (((dasatinib)[Title] AND pleural effusion [Title]). We retrieved 15 relevant article out of 24, mostly case series/reports (n=6), and phase III trial (n=3). Overall, the available evidence included 623 PE in 2397 patients (Table 1).
Prevalence and associated factors
In two phase 3 trials that evaluated patients with CML and Philadelphia chromosome-positive acute lymphoblastic leukaemia treated with dasatinib (the DASISION and the 034/Doseoptimization study), the drug-induced PE was found in 28% and 33% of patients [1,2]. PE prevalence could range between 22% [3] to as high as 69% [4], depending on the population studied, age, drug dosage, and length of follow-up. PE can occur any time after the introduction of dasatinib (Table 1), but the risk increases with the duration of the treatment [2,5]. In DASISON study, the annual incidence of 8% was steady over time [2]. PE is bilateral in two third [6] to three quarter [7] of cases. Associated cardiac effusion is found in 8 to 29% of cases [7,8].
The main risks factors commonly accepted to develop PE under dasatinib are: Age over 65 years [1], duration of the treatment, and the daily dose of dasatinib. There are also other risk factors that have been identified by authors (detailed in Table 1). Daily dose of 140 mg or higher compared to 100 mg or less are associated with an increased risk of PE (Figure 1). The standard daily dose acceptable for the chronic phase is 100 mg once daily, but higher dose (140 mg) can be given during the accelerate or blastic phase [1]. In addition, if dasatinib is taken twice daily (regardless of the dose), it seems to increase the risk to develop a PE [9,10]. Finally, lymphocytosis seems to be a risk factor for the development of PE but it is also associated with good response to treatment [11]. The risk of PE exists with most of the TKIs currently approved for both first and second line CMLCP (chronic myeloid leukemia in chronic phase) treatment, but is much higher with dasatinib [12]. Further studies are needed to determine the exact mechanism of PE in human and understand the difference in TKI risk.
The mechanism of “Primary” PE remains unclear. A recent animal study suggests that dasatinib alters endothelial barrier integrity, which result in increased pulmonary vascular endothelial permeability, eventually leading to PE [13]. Other studies pointed an immune-mediated mechanism, since the pleural liquid is an exudate containing high lymphocyte counts and that pericardial effusion is associated to PE in 26% of patients (Table 1) [14]. In the DASISION trial, pleural effusion developed more often in patients with lymphocytosis (like in our case), although this difference was not statistically significant (1). Mustjoski et al. suggested that dasatinib, through TK inhibition, may induce a reversible state of aberrant autoimmune reactivity with anti-leukemic and anti-host effect [15]. This is consistent with an early and deep molecular response of patients with PE compared to the rest of the cohort [16]. Beside “Primary” dasatinib-induced PE, which is by far the most frequent, dasatinib can be associated with “Secondary” PE through drug related heart failure, nephrotic syndrome, increased risk of pulmonary embolism and infection.
Treatment and prognosis
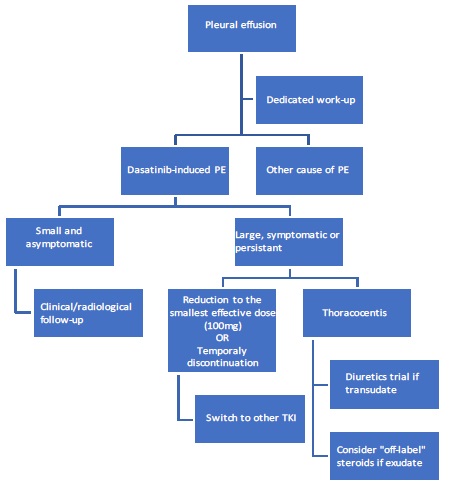
There is no consensus on the management of dasatinib-induced PE. Specialized centres manage it with a great heterogeneity [16]. We propose here (Figure 1) a pragmatic strategy, based on published evidence.
In the first step, workup of PE should look for a congestive heart failure, sign of infection, presence of thromboembolic disease, or other dasatinib unrelated PE aetiology. If there is no obvious alternative diagnosis, the patient is asymptomatic and the size of the effusion is small (Figure 1), a simple follow up by a chest x-ray could be appropriate. Nevertheless, PE that persists or is suggestive of an alternative diagnosis, deserve diagnostic thoracocenthesis. If the effusion is moderate, and/or symptomatic, dasatinib should be temporarily stopped until PE resolution, and then rechallenged at a lower dose. Maintenance of the same doses, doses reduction and treatment holiday has been associated respectively with a 100%, 60%, and 75% recurrence of PE in an observational study [16]. There is a minimal impact on patient survival or response rate with a temporary drug cessation or a diminution of the daily dose [16]. Drug dosage alteration (50 mg) or cessation can be directed by plasma drug concentration [17]. In one small study, dose reduction (50 mg) was associated with an effective PE management and disease control [17]. Drug monitoring could also play a role in PE prevention and choice of the lower effective drug dosage [17]. In a randomized study, patients with a high [C]min had dasatinib dose reduced (by 20 mg every 2 weeks to a minimum dosage of 40 mg/day) to obtain a plasma [C]min of < 3/nmol/L. Patients randomized with this strategy had lower risk of PE at 3 years (11% versus 45%) but also less drug discontinuation (13% versus 27%) compared to the control group with equivalent disease control [17].
When a thoracocentesis is performed, the fluid analysis is usually exudative and contains high lymphocyte count. Diuretic and corticoid have frequently been given, but their efficacity is unproven in this context. Despite this, in the case of transudative PE, diuretic should be considered. For exudative PE and persistent/recurrent PE despite other measure, corticoid trials remains a possible option. A recent study has shown that a treatment by tolvaptan, an orally vasopression V2-receptor antagonist, may be useful [18]. Despite an adequate management with dose reduction, recurrent drug-related PE occurred in around 60% of the cases [1,12]. Nilotinib treatment should be considered when the above measures are ineffective or when the PE is recurrent [4,5,9,11,19].
PE has no impact on disease specific survival, since 96% of these patients achieve a complete cytogenic remission and 82% achieve a major molecular response (BCR-ABL1 <0.1%, main goal of the treatment of chronic myeloid leukaemia) [2].
Conclusion
Dasatinib is an effective and generally well-tolerated second generation TKI for the treatment of CML. Dasatinib-induced pleural effusion is a frequent (and frequently overlooked) complication of the treatment. Mechanisms related to its development and treatment modalities deserve to be further explored. When a large or symptomatic pleural effusion occurs, temporal treatment alteration is safe. In case of recurrent effusion, treatment switch to nilotinib should be considered.
Conflict of interest: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Hughes TP, Laneuville P, Rousselot P, Snyder DS, Rea D, et al. Incidence, outcomes, and risk factors of pleural effusion in patients receiving dasatinib therapy for Philadelphia chromosome-positive leukemia. Haematologica. 2019; 104: 93–101.
- Cortes JE, Saglio G, Kantarjian HM, Baccarani M, Mayer J, et al. Final 5-Year Study Results of DASISION: The Dasatinib Versus Imatinib Study in Treatment-Naïve Chronic Myeloid Leukemia Patients Trial. J Clin Oncol Off J Am Soc Clin Oncol. 2016; 34: 2333–2340.
- Porkka K, Khoury HJ, Paquette RL, Matloub Y, Sinha R, et al. Dasatinib 100 mg once daily minimizes the occurrence of pleural effusion in patients with chronic myeloid leukemia in chronic phase and efficacy is unaffected in patients who develop pleural effusion. Cancer. 2010; 116: 377–386.
- Krauth M-T, Herndlhofer S, Schmook M-T, Mitterbauer-Hohendanner G, Schlögl E, et al. Extensive pleural and pericardial effusion in chronic myeloid leukemia during treatment with dasatinib at 100 mg or 50 mg daily. Haematologica. 2011; 96: 163–166.
- Cortes JE, Jimenez CA, Mauro MJ, Geyer A, Pinilla-Ibarz J, Smith BD. Pleural Effusion in Dasatinib-Treated Patients With Chronic Myeloid Leukemia in Chronic Phase: Identification and Management. Clin Lymphoma Myeloma Leuk. 2017; 17: 78–82.
- Kim D, Goh H-G, Kim S-H, Cho B-S, Kim D-W. Long-term pattern of pleural effusion from chronic myeloid leukemia patients in second-line dasatinib therapy. Int J Hematol. 2011; 94: 361–371.
- Quintás-Cardama A, Kantarjian H, O’brien S, Borthakur G, Bruzzi J, et al. Pleural effusion in patients with chronic myelogenous leukemia treated with dasatinib after imatinib failure. J Clin Oncol Off J Am Soc Clin Oncol. 2007; 25: 3908–3914.
- Latagliata R, Breccia M, Fava C, Stagno F, Tiribelli M, et al. Incidence, risk factors and management of pleural effusions during dasatinib treatment in unselected elderly patients with chronic myelogenous leukaemia. Hematol Oncol. 2013; 31: 103–109.
- Quintás-Cardama A, Kantarjian H, O’brien S, Borthakur G, Bruzzi J, et al. Pleural effusion in patients with chronic myelogenous leukemia treated with dasatinib after imatinib failure. J Clin Oncol Off J Am Soc Clin Oncol. 2007; 25: 3908–3914.
- Kim D, Goh H-G, Kim S-H, Cho B-S, Kim D-W. Long-term pattern of pleural effusion from chronic myeloid leukemia patients in second-line dasatinib therapy. Int J Hematol. 2011; 94: 361–371.
- Maral S, Bakanay SM, Kucuksahin O, Dilek I. Lupus-like symptoms with anti-RNP/Sm and anti-nuclear antibodies positivity: An extremely rare adverse event of dasatinib. J Oncol Pharm Pract Off Publ Int Soc Oncol Pharm Pract. 2019; 1078155219863469.
- Iurlo A, Galimberti S, Abruzzese E, Annunziata M, Bonifacio M, et al. Pleural effusion and molecular response in dasatinibtreated chronic myeloid leukemia patients in a real-life Italian multicenter series. Ann Hematol. 2018; 97: 95–100.
- Phan C, Jutant E-M, Tu L, Thuillet R, Seferian A, et al. Dasatinib increases endothelial permeability leading to pleural effusion. Eur Respir J. 2018; 51.
- Latagliata R, Breccia M, Fava C, Stagno F, Tiribelli M, et al. Incidence, risk factors and management of pleural effusions during dasatinib treatment in unselected elderly patients with chronic myelogenous leukaemia. Hematol Oncol. 2013; 31: 103–109.
- Breccia M, Alimena G. Pleural/pericardic effusions during dasatinib treatment: incidence, management and risk factors associated to their development. Expert Opin Drug Saf. 2010; 9: 713–721.
- Fox LC, Cummins KD, Costello B, Yeung D, Cleary R, et al. The incidence and natural history of dasatinib complications in the treatment of chronic myeloid leukemia. Blood Adv. 2017; 1: 802–811.
- Mizuta S, Sawa M, Tsurumi H, Matsumoto K, Miyao K, et al. Plasma concentrations of dasatinib have a clinical impact on the frequency of dasatinib dose reduction and interruption in chronic myeloid leukemia: an analysis of the DARIA 01 study. Int J Clin Oncol. 2018; 23: 980–988.
- Aoyama R, Ishikawa J, Harada K. The efficacy of tolvaptan in treating dasatinib-induced pleural effusions in patients with chronic myelogenous leukemia. J Cardiol. 2019.
- Fox LC, Cummins KD, Costello B, Yeung D, Cleary R, et al. The incidence and natural history of dasatinib complications in the treatment of chronic myeloid leukemia. Blood Adv. 2017; 1: 802–811.
- Nakaya A, Fujita S, Satake A, Nakanishi T, Azuma Y, et al. Clinical significance of dasatinib-induced pleural effusion in patients with de novo chronic myeloid leukemia. Hematol Rep. 2018; 10: 7474.