
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An analysis of eight family cluster cases in Wuhan, China: Peripheral blood lymphocyte count may predict Covid-19 mortality
Wenzhu Wang1; Dandan Cui1; Lijuan Zhang1; Xiwen Zhu1; Heng Fan1; Jiarui Wang2; Jian Wang3*; Rui Chen1*
1 Department of Integrated Traditional and Western Medicine, Union hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
2 Keieger School of Arts and Sciences, The Johns Hopkins University, Baltimore, MD, USA.
3 Department of Human Anatomy, College of Medical Sciences, Zhengzhou University, Zhengzhou, China.
*Corresponding Author: Jian Wang1
& Rui Chen2
1
Department of Human Anatomy, College of Medical
Sciences, Zhengzhou University, Zhengzhou, China.
Email: jianwang2020@outlook.com
2
Department of Integrated Traditional and Western
Medicine, Union hospital, Tongji Medical College,
Huazhong University of Science and Technology, Wuhan
China.
Email: 2001xh0669@hust.edu.cn
Received : May 05, 2021
Accepted : Jun 21, 2021
Published : Jun 25, 2021
Archived : www.jcimcr.org
Copyright : © Wang J & Chen R (2021).
Abstract
Background: Since December 2019, a novel coronavirus (SARSCoV-2) causing COVID-19 has spread across the world in a global pandemic. Tens of thousands of people were infected, several thousand patients died. However, key risk factors for predicting mortality remain unclear. This study aims to analyze the differences in mortal risk factors between fatal and non-fatal cases within each family, to identify the key risk factors for COVID-19 mortality.
Method: Retrospective, randomly selected eight family clusters consisting of 21 individual cases who had been confirmed positive for SARS-CoV-2 and admitted to the Wuhan Union Hospital, Wuhan, China, from February 6 to March 3, 2020. Clinical characteristics and demographic data were tracked up to March 3.
Results: Among all 8 family cluster cases, 4 families had death cases. All deaths were elderly individuals (range, 77-88 years), all ICU and severe cases were also elderly individuals (72-88 years). Patient 2-M1, who was the oldest of all cases and first confirmed with COVID-19 on January 10, had four critical comorbid conditions including colon cancer, COPD, hypertension, and coronary disease. But he remains in stable condition after more than 50 days of inpatient treatment. We observed that the absolute count of peripheral blood lymphocyte dropped to less than 0.8G/L of all death and ICU cases, ranging from 0.22 G/L to 0.81 G/L.
Conclusions: We found that elderly age is one of the main risk factors for mortality, comorbidities were not predictive of mortality due to COVID-19, although they may extend disease duration. Importantly, we discovered that within our study population the absolute count of peripheral blood lymphocyte is a predictive risk factor for mortality due to COVID-19, establishing that it may be a very important factor for judging a patient’s prognosis.
Keywords: COVID-19; Family clusters; Mortality; Risk factors.
Citation: Wang J, Chen R, Wang W, Cui D, Zhang L, et al. An analysis of eight family cluster cases in Wuhan, China: Peripheral blood lymphocyte count may predict Covid-19 mortality. J Clin Images Med Case Rep. 2021; 2(3): 1196.
Background
On December 8, 2019, the case of “pneumonia of unknown etiology” was reported in Wuhan, Hubei Province, China. A rapidly increasing rate of patient intake was reported in the fever clinics of almost every hospital of this city. At end of December 2019, a novel coronavirus (SARS-CoV-2) has been proven to be the chief source of this public health emergency [1]. The coronavirus disease 2019 (COVID-19) diffused around the country and resulted in a national outbreak at the end of January. According to the Word Health Organization (WHO) [2], on January 31, 9720 cases of COVID-19 were confirmed in China with 213 deaths; 106 confirmed cases were reported outside of China with 19 countries having been affected. On Feb 27, 2020 the WHO reported that China had 78630 confirmed cases (including 439 new cases in the past 24 hr period) resulting in 2747 (29 new) deaths; outside of China, there were 3664 cases (including 746 new cases) affecting 46 countries and resulting in 57 (13 new) deaths [2]. For the first time, there have been more new cases reported from countries outside of China than from China itself. COVID-19 has caused a global pandemic, and Novel Coronavirus–Infected Pneumonia (NCIP) has led to major health challenges throughout the world.
According to a Chinese Center for Disease Control and Prevention (CDC) report on March 3, 2020 [3], most patients present with non-severe cases, however 3.71% of cases ultimately resulted in death. There is a question as to why some patients presented with milder clinical symptoms and signs, while some cases manifested in organ dysfunction (shock, Acute Respiratory Distress Syndrome (ARDS), acute cardiac injury, and acute kidney injury) and even died. At this moment studies of the phylogenomic traits viral virulence still have reached no certain conclusion [4]. For this study we analyzed the clinical characteristics and predisposing factors of 8 family clustered NCIP cases, including cases in which NCIP resulted in death, in order to identify risk factors for elevated rates of mortality.
Method
This study was approved by the institutional ethics board of the Wuhan Union Hospital of Huazhong University of Science and Technology (2020.0089). The Wuhan Union Hospital is responsible for treating critically ill patients with NCIP and is one of the closest major hospitals to the Huanan seafood market to which many early cases of COVID-19 were associated. On February 6, 2020, we started to participate in treating hospital patients with severe SARS-CoV-2–infected viral pneumonia who were admitted to Wuhan Union Hospital. During our work we found that there are many cases within family clusters, with patients of each family having nearly the same onset date, same living environment, and same diet. However, while some members presented with severe cases resulting in death, others presented with non-severe cases. We collected 8 families (21 cases) as the focus for the study. Oral consent was obtained from family members. All patients were diagnosed with NCIP by their pulmonary CT images and were SARS-CoV-2 positive in throat swab samples confirmed by RT-PCR. Diagnostic criteria were based on recommendations by the Chinese National Institute for Viral Disease Control and Prevention [5]. Clinical characteristics and demographic data were tracked up to March 3.
According to the diagnostic and treatment guidelines for COVID-19 issued by the Chinese National Health Committee (Version 3-7) [5], cases of severe NCIP were defined based on the following criteria: Respiratory frequency ≥30/min, oxygen saturation ≤93% or oxygenation index ≤300 mmHg. The patients who required ICU care met one of the following criteria: Respiratory failure requiring ventilation, development of shock, and/ or complications resulting in organ failure. The onset date was identified as the date when patients first noticed symptoms. A detailed analysis of case records was carried out.
Results
The study population included 21 patients within 8 families with confirmed cases of NCIP. The demographic and clinical characteristics are shown in Table 1. Among all 8 family cluster cases, 4 families had death cases (bold in Table 1). All deaths were elderly individuals (range, 77-88 years), all ICU and severe cases were also elderly individuals (72-88 years). These cases had nearly the same age range. In addition, the onset of every group of family cases occurred within the same period. Members from each family were infected by SARS-CoV-2 with virtually identical virulence, however younger patients generally presented as non-severe cases while all deaths occurred in elderly patients over the age of 70.
Table 1: Baseline Characteristics of Cases infected With SARS-CoV-2.
Family |
Member |
Age ranges |
Sex |
Onset of symptoms |
Chest CT images |
Comorbid factor(s) |
Disease (Duration) |
Disease severity |
1 |
(M1) Father |
80-89 |
M |
1/31/2020 |
Bilateral patchy shadowing |
None |
30 |
Death |
(F1) Mother |
80-89 |
F |
1/26/2020 |
Local patchy shadowing |
Hypertension, Deep vein thrombosis |
34 |
Severe |
|
(M2) Son |
50-59 |
M |
1/29/2020 |
Ground-glass opacity |
None |
24 |
Non-severe |
|
2 |
(M1) Father* |
90-95 |
M |
1/10/2020 |
Local patchy shadowing |
COPD, Hypertension, Coronary Disease, Colon Cancer |
52 |
Non-severe |
(M2) Son |
60-69 |
M |
2/13/2020 |
Ground-glass opacity |
None |
17 |
Non-severe |
|
3 |
(M1) Grand-Father |
80-89 |
M |
2/6/2020 |
Local patchy shadowing |
Prostate cancer |
30 |
ICU to Non-severe |
(M2) Father |
60-69 |
M |
1/29/2020 |
Ground-glass opacity |
None |
26 |
Non-severe |
|
(F1) Mother |
60-69 |
F |
1/28/2020 |
Local patchy shadowing |
None |
35 |
ICU to Non-severe |
|
(F2) Daughter |
30-39 |
F |
2/2/2020 |
Ground-glass opacity |
None |
23 |
Non-severe |
|
4 |
(M1) Father |
70-79 |
M |
1/26/2020 |
Local patchy shadowing |
Hypertension, Coronary Disease, Heart bypass |
37 |
ICU |
(F1) Mother |
70-79 |
F |
1/25/2020 |
Ground-glass opacity |
Hypertension, Coronary Disease |
38 |
Severe |
|
(M2) Son |
40-49 |
M |
1/21/2020 |
Bilateral patchy shadowing |
None |
38 |
Non-severe |
|
5 |
(M1) Husband |
70-79 |
M |
1/28/2020 |
Local patchy shadowing |
None |
15 |
Death |
(F1) Wife |
80-89 |
F |
1/18/2020 |
Ground-glass opacity |
Arteriosclerosis |
44 |
Severe |
|
6 |
(M1) Husband |
70-79 |
M |
1/25/2020 |
Bilateral patchy shadowing |
Hypertension, Coronary Disease |
37 |
ICU |
(F1) Wife |
60-69 |
F |
2/6/2020 |
Bilateral patchy shadowing |
Endometrial cancer |
24 |
Non-severe |
|
7 |
(F1) Mother |
80-89 |
F |
2/6/2020 |
Bilateral patchy shadowing |
Hypertension, Coronary Disease chronic bronchitis |
25 |
Non-severe |
(F2) Daughter |
50-59 |
F |
1/31/2020 |
Ground-glass opacity |
Hyperthyroid |
37 |
Non-severe |
|
8 |
(M1) Father |
80-89 |
M |
2/2/2020 |
Bilateral patchy shadowing |
COPD |
16 |
Death |
(F1) Mother |
80-89 |
F |
1/28/2020 |
Bilateral patchy shadowing |
Coronary disease Diabets |
33 |
Death |
|
(F2) Daughter |
50-59 |
F |
2/9/2020 |
Ground-glass opacity |
None |
22 |
Non-severe |
Out of the 12 patients with comorbid conditions (Table 1 and Figure 1), 2 resulted in deaths, 3 resulted in ICU, 3 resulted in severe cases, and 4 resulted in non-severe cases. In family 1 and 5, each couple had the same onset time, and while both husbands had no comorbid conditions, their wives both had chronic diseases. However, both male patients died while the female patients were still alive after more than 30 days of treatment. In family 4, the elderly parents (4-F1 and 4-M1) became symptomatic on nearly the same date and have the same chronic diseases. However the condition of 4-M1 worsened and he was transferred to the ICU while 4-F1 remained stable. Patient 2-M1, who was the oldest of all cases and first confirmed with COVID-19 on January 10, had four critical comorbid conditions including colon cancer, COPD, hypertension, and coronary disease. But he remains in stable condition after more than 50 days of inpatient treatment.
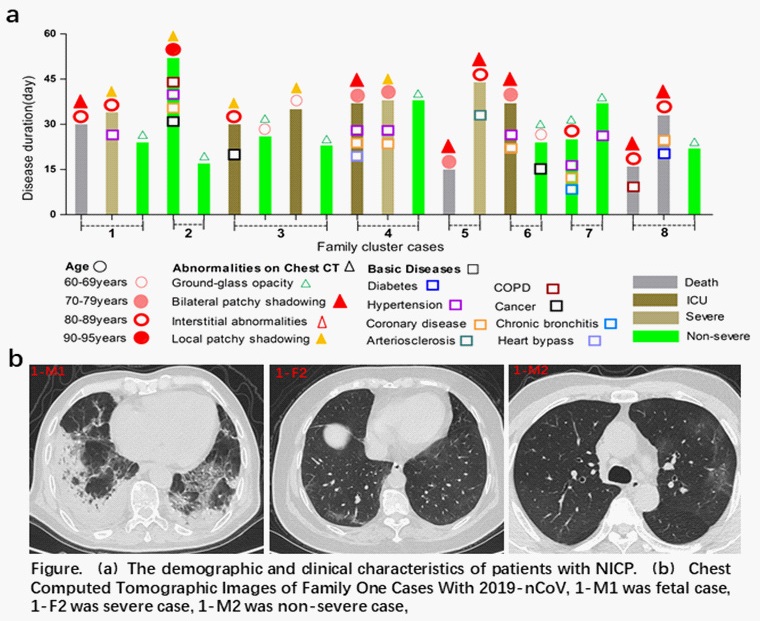
From these cases, it seems that comorbid conditions are not a major risk factor for mortality, but it most likely to be a key factor that extends the disease duration. Old age is a main risk factor for mortality, but is still not directly related to death of COVID-19. Moreover, although every family has a common living environment, similar dietary structure, same viral infectious condition, and similar onset date, women generally have slower disease progression and stronger living ability.
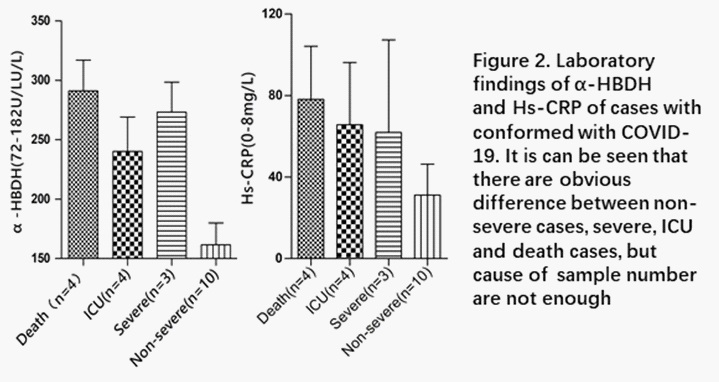
At the time of admission we collected all patients’ blood routine test results and biochemistry and C-reactive Protein (HsCRP) results (Table 2). By comparison, we found there were 20 patients with elevated levels of α-hydroxybutyrate dehydrogenase (α-HBDH) and 14 cases of increased Hs-CRP. The level of α-HBDH had a tendency to be elevated in fatal, ICU, and severe cases, however we could not analyze this due to a small sample size.
Table 2: Laboratory Results of The Familiar Cluster Conformed with COVID -19.
Family |
Member |
Lymphocyte (1.1-3.2G/L) |
Lymphocyte% (20-50%) |
Leucocyte (3.5-9.5G/L) |
Creatine Kinase (24-170U/L) |
CK-MB (0-25U/L) |
a-HBDH (72-182U/L) |
Hs-CRP (0-8mg/L) |
1 |
(M1) Father |
0.73 |
20.3 |
3.61 |
92 |
10 |
216 |
77.53 |
(F1) Mother |
2.23 |
33.6 |
6.64 |
171 |
25 |
235 |
6.8 |
|
(M2) Son |
1.45 |
35.2 |
4.11 |
438 |
14 |
206 |
4.11 |
|
2 |
(M1) Father* |
1.55* |
24.1 |
6.43 |
45 |
8 |
176 |
83.33 |
(M2) Son |
1.2 |
25.1 |
4.77 |
43 |
11 |
67 |
0.1 |
|
3 |
(M1) Grand-Father |
0.65 |
16.9 |
3.84 |
63 |
10 |
184 |
76.65 |
(M2) Father |
1.36 |
25.6 |
5.3 |
686 |
21 |
146 |
34.76 |
|
(F1) Mother |
0.81 |
29.7 |
2.74 |
326 |
21 |
235 |
37.92 |
|
(F2) Daughter |
1.58 |
34.1 |
4.63 |
88 |
8 |
133 |
17.19 |
|
4 |
(M1) Father |
0.66 |
17.2 |
3.85 |
886 |
26 |
221 |
2.63 |
(F1) Mother |
1.23 |
29.2 |
4.21 |
271 |
17 |
264 |
26.82 |
|
(M2) Son |
2.1 |
31 |
3.51 |
74 |
21 |
109 |
23 |
|
5 |
(M1) Husband |
0.68 |
12.7 |
3.45 |
981 |
30 |
325 |
152 |
(F1) Wife |
1.27 |
20.6 |
6.16 |
78 |
14 |
85 |
32.68 |
|
6 |
(M1) Husband |
0.22 |
17.5 |
12.83 |
582 |
25 |
321 |
145.55 |
(F1) Wife |
1.31 |
25.9 |
5.07 |
145 |
39 |
283 |
22.97 |
|
7 |
(F1) Mother |
1.8 |
26.5 |
6.81 |
57 |
9 |
146 |
3.52 |
(F2) Daughter |
2.03 |
35 |
5.78 |
230 |
10 |
182 |
0.96 |
|
8 |
(M1) Father |
0.72 |
13.8 |
9.24 |
663 |
39 |
325 |
44.86 |
(F1) Mother |
0.34 |
7.9 |
4.34 |
173 |
14 |
299 |
38.38 |
|
(F2) Daughter |
0.76 |
22.3 |
3.42 |
43 |
5 |
169 |
0.1 |
Interestingly, we observed that the absolute count of peripheral blood lymphocyte dropped to less than 0.8 G/L of all death and ICU cases , ranging from 0.22 G/L to 0.81 G/L. Except in one non-severe case, the other cases were all within normal range (1.1-3.2 G/L). According to case records, one non-severe (8-F2) patient in family 8, whose count of lymphocyte fell to 0.76 G/L, had her levels return to normal (1.15 G/L) at one week after admission. Furthermore, the aforementioned 94 years old patient with multiple comorbid conditions, was defined as a non-severe case, and remained stable after 52 days of inpatient treatment. His absolute count of peripheral blood lymphocyte was normal (1.55 G/L). In summary, we have identified a decrease in the absolute count of peripheral blood lymphocyte to less than 0.8 G/L as one of the key risk factors for COVID-19 mortality, and this factor has been identified as having a direct relationship with disease progression and prognosis.
All 21 cases had received CT scans on admission. The results showed that COVID-19 had caused varying degrees of destruction to every patients’ lungs. All non-severe and some severe patients’ pulmonary CT presented mild to moderate injury, including local patchy shadowing or ground-glass opacity. All 4 deceased patients’ CT images had displayed bilateral patchy shadowing. The patients with reductions in absolute count of peripheral blood lymphocyte also demonstrated large area bilateral patchy shadowing, as well as declining health (Figure 2).
Discussion
At this point in time, COVID-19 has been sweeping the globe for many weeks. We found it useful to look at family cluster cases which have the same viral infectious condition, common living environments, and similar dietary structures. Accounting for external risk factors, the mortal risk factors between fatal and non-fatal cases within each family could be better analyzed. Overall, 4 deaths and 4 ICU patients from 6 families were all elderly parents, with ages ranging from 72 to 88 years. Advanced age is one of the main risk factors for COVID-19 mortality. According to the work of Wu and McGoogan [6] (the largest population-based analysis of COVID-19), out of a total of 44672 confirmed cases, there were 1023 cases that resulted in death. 50.83% (508 of 1023) of fatal cases occurred in patients aged >70 years old. These results are consistent with our family cluster cases.
We note that 2 out of 4 fatal cases had no comorbid factors. 12 patients from 8 families had comorbid factors, however there was no obvious direct correlation between comorbidities and disease severity. Patient 2-M1 remained in stable condition, representing how we can see that comorbidities are not necessarily not the key risk factor for elevated mortality in COVID-19 patients. It is more likely to merely be a factor that extends disease duration. In Dr. Wang’s study [7] it was found that the number of cases requiring ICU or non-ICU treatment did not differ based on underlying comorbidities.
Out of 9 cases where the absolute count of peripheral blood lymphocyte dropped to under 0.81 G/L, 4 cases were fatal and 4 were hospitalized in the ICU. 1 case from family 8 had backed to normal after 7 days in hospital. All other cases had normal levels of peripheral blood lymphocyte. Referring again to 94 year old patient 2-M1, although he would be expected to be at high risk for COVID-19 he did not experience a severe drop in blood lymphocyte levels and remained stable. These findings are supported by a study from Zhou [8] at el. which also found obvious changes in lymphocyte count in COVID-19 death cases.
Conclusions
This study may be one of the first out of the Wuhan epicenter to focus on family clusters of COVID-19 cases. In line with other research, we found that elderly age is one of the main risk factors for mortality, but we did not prove a directly causal relationship between age and death. We also found that comorbidities were not predictive of mortality due to COVID-19, although they may extend disease duration. Importantly, we discovered that within our study population the absolute count of peripheral blood lymphocyte is a predictive risk factor for mortality due to COVID-19, establishing that it may be a very important factor for judging a patient’s prognosis.
Declarations
Ethics approval and consent to participate: This study was approved by the institutional ethics board of the Wuhan Union Hospital of Huazhong University of Science and Technology (2020.0089). Oral consent was obtained from all family members.
Consent for publication: Not Applicable.
Availability of data and material: The datasets generated and/or analysed during the current study are not publicly available due to protect patient privacy, but are available from the corresponding author on reasonable request.
Competing interests: None of the authors have any conflict of interest to declare. These patients have not been reported in any other submission by you or anyone else.
Funding: This work was supported by grants from NSFC (No. 81904023 to Wenzhu Wang).
Author contributions: Drs WZ. Wang and Chen had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Idea, design and concept: Drs WZ Wang, D Cui and J Wang; Analysis, interpretation of data and draft manuscript writing: W Wang; Patients’ information and clinical record collection: WZ Wang, D Cui, L Zhang, X Zhu, H Fan, R Chen; Critical revision of the manuscript for important intellectual content: JR Wang and J Wang.
References
- Zhu N, Zhang D, Wang W, Li X, Yang B, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. New England Journal of Medicine. 2020; 382: 727-733.
- Coronavirus disease (COVID-2019) situation reports [https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200131-sitrep-11-ncov. pdf?sfvrsn=de7c0f7_4]
- Distribution of COVID-19 in China [http://2019ncov.china cdc.cn/2019-nCoV/]
- Geoghegan JL, Holmes EC: The phylogenomics of evolving virus virulence. Nature Reviews Genetics 2018; 19: 756- 769.
- Chinese Center for Disease Control and Prevention [http://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/ jszl_11815/202003/t20200305_214142.html]
- Wu Z MJ: Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. Jama. 2020.
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. Jama. 2020.
- Fei Zhou TY, Ronghui Du, Guohui Fan, Ying Liu, Zhibo Liu, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. lancet. 2020.