
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A case report of entrapped angioplasty balloon in circumflex coronary artery
Mateusz Surowiec; Sławomir Żurek; Maciej Kolowca; Monika Kosiorowska; Janusz Bąk; Marcin Rak; Kazimierz Widenka*
Szpital Wojewódzki N2, Oddział Kardiochirurgii, Rzeszów, Poland.
*Corresponding Author: Kazimierz Widenka
Szpital Wojewódzki N2, Oddział Kardiochirurgii,
Rzeszów, Poland.
Email: kazw@poczta.onet.pl
Received : May 11, 2021
Accepted : Jun 23, 2021
Published : Jun 29, 2021
Archived : www.jcimcr.org
Copyright : © Widenka K (2021).
Abstract
Entrapment of coronary angioplasty hardware during coronary artery interventions is rare but in most cases requires prompt treatment. This article reported a case of 65-year-old woman who underwent a percutaneous transluminal coronary angioplasty to the circumflex artery.
A ruptured angioplasty balloon was entrapped in the circumflex artery with proximal end of the guidewire placed in the descending aorta. The patient underwent surgical removal of the foreign body and coronary artery bypass grafting. The case and the management are discussed.
Keywords: Angioplasty; coronary artery bypass; equipment failure; angioplasty balloon.
Citation: Widenka K, Surowiec M, Żurek S, Kolowca M, Kosiorowska M, et al. A case report of entrapped angioplasty balloon in circumflex coronary artery. J Clin Images Med Case Rep. 2021; 2: 1206.
Introduction
Entrapment, retention or fracture of a coronary angioplasty hardware such as stent, coronary balloon shaft, femoral arterial sheath, and guidewire is a rare but serious complication of coronary interventions. Loss or entrapment of device can result in intracoronary or systemic embolization, thrombus formation, emergent coronary artery bypass graft surgery, or death [1].
The frequency of such incidents is estimated from 0,21% to 0,8% [4-6]. These patients could be treated with Percutaneous methods of retrieval with success, but in half of cases, when intervention was performed, surgery was required [3].
We report a case of the patient with an entrapped guidewire during PCI, which was retrieved successfully from theCcircumflex artery (Cx) and the aorta through the aortotomy followed by coronary artery bypass grafting to the circumflex artery using the patient’s saphenous vein.
Case report
A 65-year-old female, hypertensive, obese, diabetic was admitted to a department of invasive cardiology. Her medical history included Non ST Elevation Myocardial Infarction (NSTEMI) followed by angioplasty of the anterior interventricular branch of the left coronary artery (left anterior descending – LAD) with Drug-Eluting Stent (DES) implantation in 2009, and a repeat LAD angioplasty with DES implantation (2010).
On admission the patient presented with severe chest pain of acute onset and shortness of breath.
Diagnostic cardiac catheterization showed a critical stenosis in the proximal segment of the circumflex artery and subcritical restenosis in the proximal segment of (LAD).
The patient underwent angioplasty and stenting of the circumflex artery.
A drug-eluting stent was implanted in the proximal part of the circumflex artery with jailed balloon technique. The origin of the obtuse marginal artery (OM) was covered with stent and was followed by immediate chest pain.
An attempt to dilate the stent with coronary angioplasty balloon catheter was made but the balloon ruptured and guidewire entrapment occurred.
The patient’s condition was stable. After a consultation, the patient was transferred to a reference center.
In the catheterisation laboratory the unsuccessful attempt to withdraw the angioplasty balloon, resulted in the fracture of the wire with its proximal end placed in descending aorta. The patient’s condition remained stable again stable.
The patient was then transferred to a cardiac surgery department and the emergency surgical removal of entrapped angioplasty balloon was performed.
Procedure was done on cardiopulmonary bypass using standard technique. Antegrade Del Nido cardioplegia was administered to arrest the heart.
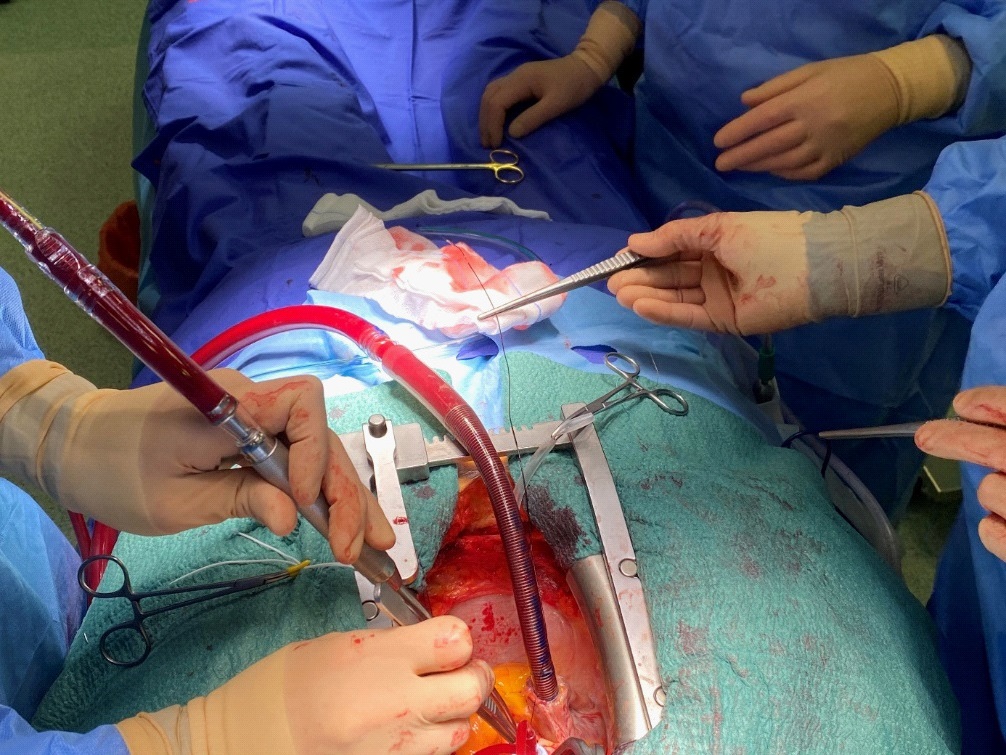
The ascending aorta was opened, and the guidewire was removed from the aorta under visual control (Figure 1).
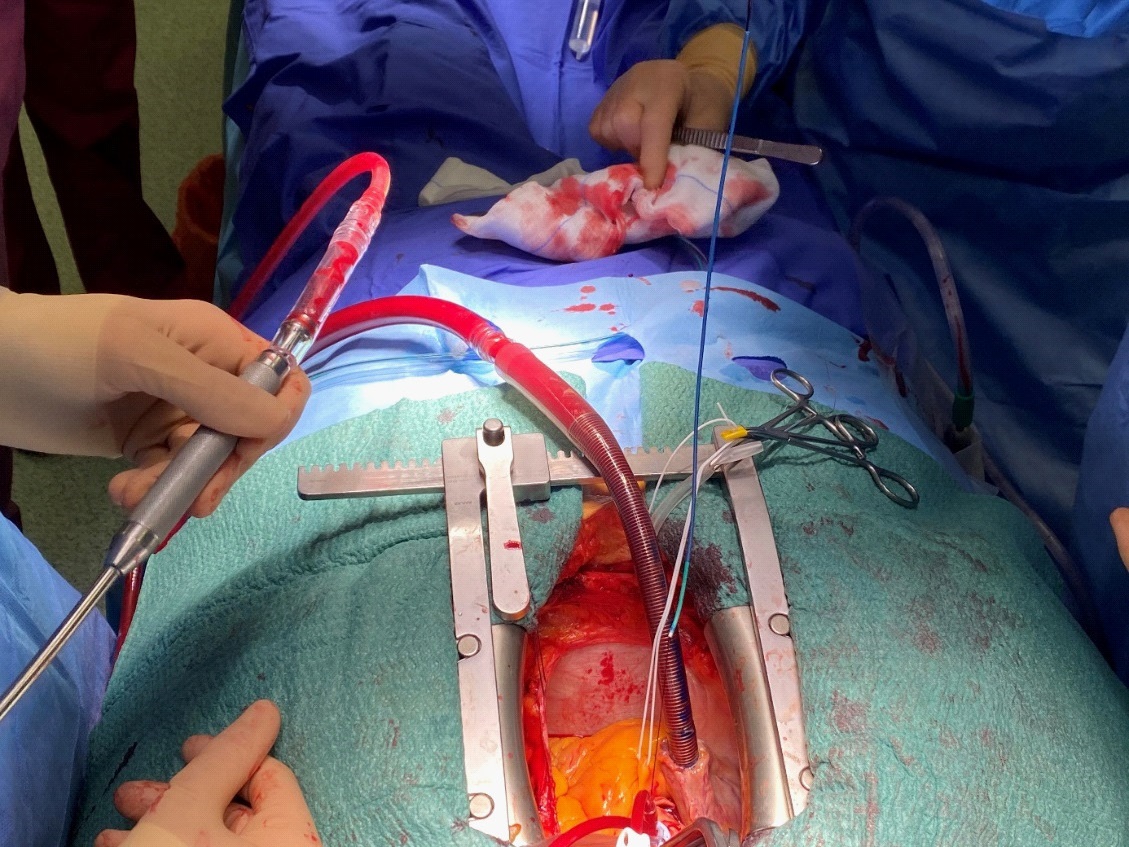
Subsequently, Judkin’s right catheter was inserted over the guidewire to the point of entrapped balloon (Figure 2).
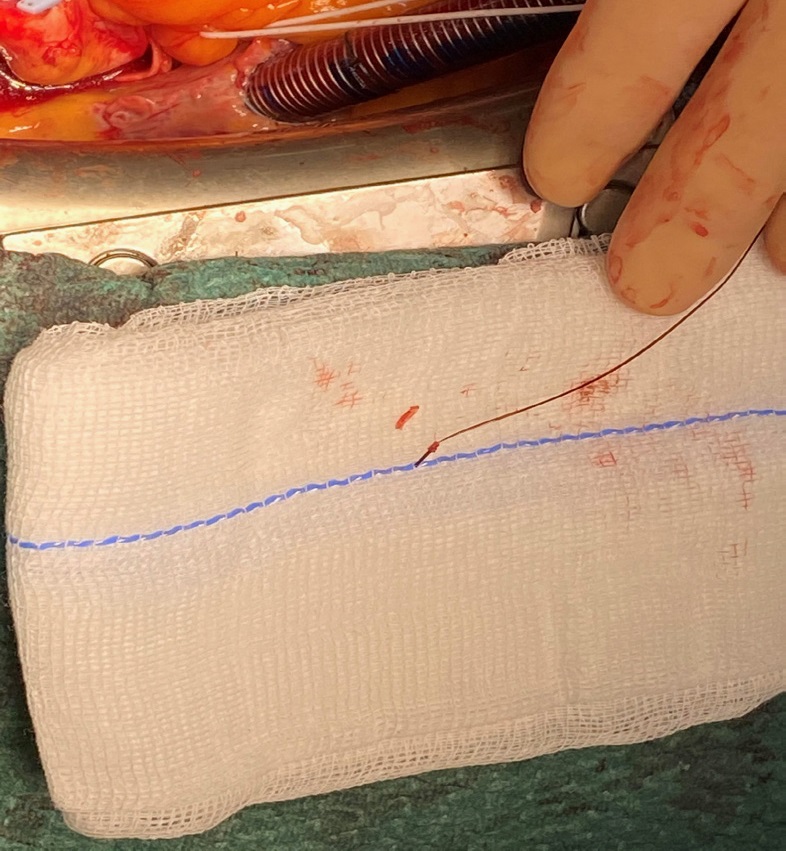
Then angioplasty balloon was then gently moved forward with the Judkins catheter in order to unjam the entrapped balloon. After this manoeuvre, both angioplasty balloon and Judkin’s right catheter were removed from the circumflex artery (Figure 3).
The aortocoronary bypass graft was then performed using the patient’s saphenous vein in view of the potential risk of stent occlusion due to removal of the angioplasty balloon.
The patient had an uneventful recovery and was transferred to the cardiac rehabilitation center on the fifth postoperative day.
Discussion
Retained foreign bodies within the coronary vessels present a serious medical problem. The incidence of fragmentation, loss or entrapment of hardware device during or after PCI various from 0,2% to 0,8% [4-6], however in one publication it was as high as high as 8,3% [2].
The presence of entrapped devices in a coronary arteries could lead to potentially fatal complications such as acute embolization, acute coronary thrombosis, coronary rupture leading to tamponade and myocardial infarction [7].
Prompt management is imperative if patient becomes hemodynamically unstable or developed acute coronary event. On the other hand small parts of devices left in distal, small or occluded coronary arteries can be managed conservatively [8,9].
Percutaneous retrieval of entrapped hardware can be successful, but when procedure is performed inappropriately, vigorous traction of guidewire can lead to further damage of the of endothelium with subsequent vessel thrombosis or its rupture [3,10].
After failed attempt of percutaneous removal of entrapped hardware, surgical intervention should be undertaken, especially if foreign body remains in aortic root, ascending aorta or aortic arch, due to significant risk of systemic embolic events, including cerebral vascular embolization [11].
The wire can be withdrawn through aortotomy, both from aorta and from the coronary vessel. If entrapped catheter or wire cannot be withdrawn, its amputation as near to coronary ostium as possible should be considered as last option. Alternative option is arteriotomy, but it can lead to further vessel injury or can result in complications due to the presence of atherosclerotic disease or previously implanted stents including left main injury.
After removal of foreign body from aortotomy site, simple bypass grafting seems to be reasonable due to possible risk of coronary occlusion and the inability to inspect the patency of the vessel [3,7].
Conclusion
Guide wire entrapment is a rare complication, but with increasing number of percutaneous intervention, the number of incidents is going to rise. In our case we present that surgical removal of foreign body from coronary artery that can be safe and efficient. It is important for interventional cardiologists and cardiac surgeons to carefully chose optimal, percutaneous or surgical, technique for catheter removal.
References
- Ahmad T, Chithiraichelvan S, Patil TA, Jawali V. Surgical retrieval of entrapped coronary angioplasty guidewire from the aorta. Asian Cardiovascular and Thoracic Annals. 2014; 24: 81–84.
- Tamci B, Okan T, Gungor H, Ozturk V, Cam F. Stent entrapment and guide wire fracture during percutaneous coronary intervention in the same patient. Advances in Interventional Cardiology. 2013; 2; 190–193.
- Chang TM, Pellegrini D, Ostrovsky A, Marrangoni AG. Surgical management of entrapped percutaneous transluminal coronary angioplasty hardware. Tex Heart Inst J. 2002; 29: 329-332.
- Hartzler GO, Rutherford BD, McConahay DR. Retained percutaneous transluminal coronary angioplasty equipment components and their management. Am J Cardiol. 1987; 60: 1260- 1264.
- Lotan C, Hasin Y, Stone D, Meyers S, Applebaum A, et al. Guide wire entrapment during PTCA: A potentially dangerous complication. Cathet Cardiovasc Diagn. 1987; 13: 309-312.
- Steffenino G, Meier B, Finci L, et al. Acute complications of elective coronary angioplasty: A review of 500 consecutive procedures. Br Heart J. 1988; 59: 151-158.
- Ahmad T, Chithiraichelvan S, Patil TA, Jawali V. Surgical retrieval of entrapped coronary angioplasty guidewire from the aorta. Asian Cardiovasc Thorac Ann. 2016; 24: 81-84.
- Singh J, Thingnam SK, Das D, Singh H, Sharma R, et al. Surgical removal of entrapped and broken percutaneous transluminal coronary angioplasty balloon catheter. Interact Cardiovasc Thorac Surg. 2007; 6: 94-96.
- Alexiou K, Kappert U, Knaut M, Matschke K, Tugtekin SM. Entrapped coronary catheter remnants and stents: Must they be surgically removed? Tex Heart Inst J. 2006; 33: 139-142.
- Karabay KO, Bagirtan B. Broken guidewire fragment. Int J Angiol. 2012; 21: 241-242.
- Domaradzki W, Sanetra K, Skwarna B, Król M, Kuczera M, et al. Surgical removal of entrapped guidewire fragment following direct circumflex artery angioplasty and stenting. Kardiochir Torakochirurgia Pol. 2015; 12: 242-245.