
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Role of Sodium Thiosulphate in Calciphylaxis
Meshal Qaiser*; Arora Kanwardeep
Griffin Hospital, Derby, CT, 130 Division Street, 06418, USA.
*Corresponding Author: Meshal Qaiser
Griffin Hospital, Derby, CT, 130 Division Street, 06418,
USA.
Email: mqaiser@griffinhealth.org
Received : May 20, 2021
Accepted : Jun 28, 2021
Published : Jun 30, 2021
Archived : www.jcimcr.org
Copyright : © Qaiser M (2021).
Abstract
Calciphylaxis, also known as Calcific Uremic Arteriolopathy (CUA), is a rare condition often but not exclusively seen in end stage renal disease. Current literature recommends trial of Sodium Thiosulphate (STS) in all CUA patients. The long - term use of STS is limited by the adverse effect of Anion Gap Metabolic Acidosis (AGMA) which can be managed timely to maximize the benefits of STS.
Citation: Qaiser M, Kanwardeep A. Role of sodium thiosulphate in calciphylaxis. J Clin Images Med Case Rep. 2021; 2(3): 1214.
Case report
An 86-year-old obese female with medical history of CKD V, DM- II, hypertension and atrial fibrillation on warfarin presented to the hospital with non-healing ulcers on lower extremity.
Patient reported a tender black eschar on her right thigh which developed three months prior to admission. Initial lesion was thought to be an insect bite; ulcer continued to worsen despite debridement, antibiotic therapy and close follow up at wound care center. She reported no fever, chills or systemic symptoms.
On admission, physical examination revealed extremely painful, foul smelling, necrotic ulcer, draining purulent discharge on the right medial thigh. Left thigh and calf also had tender, violaceous non-ulcerating skin changes. Labs revealed leukocytosis, BUN/creatinine- 110/5.1 mg/dl, normal anion gap, INR of 4.23, PTH 600 pg/dl, calcium 8.9 mg/dl and phosphate 7.4 mg/dl with high Ca×Phosphate product of 65.86.
Due to the presence of risk factors (obesity, female gender, ESRD, diabetes mellitus, warfarin use) and after exclusion of other differentials, clinical diagnosis of Calciphylaxis was made. Concerns for introducing an infection and supratherapeutic INR precluded skin biopsy. Warfarin induced skin necrosis was excluded as the patient was taking the medication for many years with no issues. Also, peripheral vascular disease was ruled out as the patient had good distal pulses.
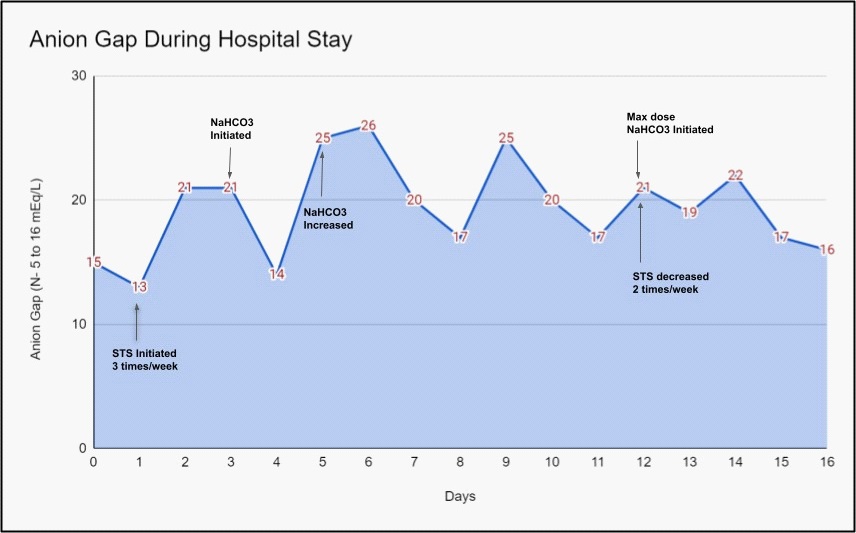
Multidisciplinary management was pursued with wound care, antibiotics (later discontinued) and appropriate analgesia. Her warfarin was switched to apixaban. Her calcium acetate was switched to Sevelamer for hyperphosphatemia and Cinacalcet was added to manage her hyperparathyroidism with a goal PTH of 150-300. Patient was also initiated on STS 25 g IV thrice weekly. Patient’s anion gap increased from normal to 26 after two doses of STS, which directly correlated with STS initiation (Figure 1), prompting dosage reduction to twice weekly. Sodium bicarbonate was initiated and had to be titrated up to the maximum allowed dose with subsequent resolution of anion gap.
Due to clinical improvement, STS was continued and the patient was discharged with careful monitoring of anion gap. Patient was eventually initiated on hemodialysis and STS was continued with dialysis sessions. Post discharge follow up revealed significant healing of wounds (Figure 2) and marked improvement in pain.

Discussion
CUA is a rare disorder with high morbidity and estimated sixmonth mortality of approximately 60 percent. Exact pathogenesis is unclear and risk factors include female gender, obesity, ESRD, hyperphosphatemia, hypercalcemia, medications like warfarin, calcium-based phosphate binders etc [1].
Patients present with skin ischemia and necrosis with histological features of calcification of arterioles and capillaries in dermis and subcutaneous adipose tissue. Diagnosis is usually clinical and can be confirmed by skin biopsy [2]. Management entails multidisciplinary approach with attention to analgesia, wound care, and mitigation of risk factors [3]. This involves discontinuation of medications that may contribute to calciphylaxis (vitamin D, calcium-based phosphate binders, warfarin and iron). Correction of hypercalcemia and hyperphosphatemia is also warranted along with optimization of PTH to goal levels of 150-300.
All patients with CUA are warranted a trial of STS for 3-4 weeks to ascertain if they will benefit from its continuation. Evidence for its use is mostly derived from retrospective studies and case reports due to the rarity of the disease [4,5]. STS, commonly known as antidote for cisplatin and cyanide toxicity, is thought to reduce pain and heal wounds due to its antioxidative properties via Glutathione, vasodilatory effect by H2S (Hydrogen Sulfide) and interference with calcium deposition in adipose and vascular tissue by Calcium thiosulphate [5].
AGMA has been recognized as the most common and dose limiting adverse effect of STS, which is thought to be caused by the metabolite of STS (Hydrogen Sulfide-H2S) [5,6]. Excess of Hydrogen Sulfide can lead to extreme lactic acidosis via inhibition of mitochondrial ATP production. Other possible mechanisms include formation of thiosulphuric acid in vivo and oxidative stress from sulfide-containing compounds.
Conclusion
Our patient responded extremely well to STS but also developed concurrent AGMA requiring maximum dose of sodium bicarbonate administration to counteract the acidosis. This case highlights the role of STS and its adverse effects of AGMA. Careful monitoring of anion gap and prompt initiation of treatment can ameliorate the side effect allowing patients to obtain maximum benefits of wound healing and pain control in CUA patients.
References
- Nigwekar SU. et al. Caliciphylaxis. N Engl J Med. 2018; 378: 1704 -1714.
- Prohic N, et al. Calciphylaxis - Case Report. Med Arch. 2020; 74: 233–235.
- Baldwin C, et al. Multi-intervention management of calciphylaxis: A report of 7 cases. Am J Kidney Dis. 2011; 58: 988-991.
- Nigwekar SU, et al, Calciphylaxis: Risk Factors, Diagnosis, and Treatment. Am J Kidney Dis. 2015; 66: 133–146.
- Mao M, Lee S, Kashani K, Albright R, Qian Q. Severe Anion Gap Acidosis Associated with Intravenous Sodium Thiosulfate Administration. J Med Toxicol. 2013; 9: 274–277.
- Hunt GM, Ryder HF. Metabolic acidosis after sodium thiosulfate infusion and the role of hydrogen sulfide. Clin Case Rep. 2018; 6: 1595-1599.