
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Aggressive behavior of peripheral giant cell granuloma: A case report
Nadia Fathy Hassabou*; Yasmine Alaa Eldin; Amina Fouad Farag
Oral and Maxillofacial Pathology, Faculty of Dentistry, October 6 University, Giza, Egypt.
*Corresponding Author: Nadia Fathy Hassabou
Oral Pathology Department, Faculty of Dentistry,
October 6 University, Al Mehwar Al Markazi, In front
of 6 October Club, October 6 City, Giza Governorate,
Egypt.
Email: dr_nadia_hassabou@hotmail.com
Received : May 04, 2021
Accepted : Jul 02, 2021
Published : Jul 06, 2021
Archived : www.jcimcr.org
Copyright : © Hassabou NF (2021).
Abstract
Background: Peripheral Giant Cell Granuloma (PGCG) considered one of the commonest oral giant cell lesions and gingival epulis. It is probably a non neoplastic lesion but rather reactive in nature which originates from the periodontal membrane or the periosteum as a reaction to chronic trauma or local irritation. This article reports a case of PGCG in a 6 years old male patient complaining of massive gingival swelling associated with looseness of related teeth which is highly unlikely to occur with such lesions, that may lead to misdiagnosis.
Material and method: Surgical excision followed by histopathological examination was performed and confirmed using CD34 and CD45 for detection and confirming the origin of multinucleated giant cells (MNGCs).
Results: Immunopositivity for CD34 was demonstrated only as cytoplasmic reaction of endothelial cells lining blood vessels while negative reaction was observed in MNGCs or in stromal mononuclear cell. Moreover, cytoplasmic immunoreactivity for CD45 was revealed in MNGCs and few stromal cells.
Conclusion: Correlating clinical, radiographic and histopathologic examination reaching definite and early diagnosis is mandatory for management of such lesions thus eliminating potential risk of damaging to adjacent hard tissue structures.
Keywords: Peripheral giant cell granuloma; multinucleated giant cells; CD34; CD45.
Citation: Hassabou NF, Eldin YA, Farag AF. Aggressive behavior of peripheral giant cell granuloma: A case report. J Clin Images Med Case Rep. 2021; 2(4): 1218.
Introduction
Peripheral Giant Cell Granuloma (PGCG) is one of the most common oral giant cell lesions which does not represent a true neoplasm rather than hyperplastic reactive nature which originates from the interdental tissues either periosteum or periodontal membrane. PGCG in oral cavity appearing as purplish-red extra-osseous soft tissue nodule consisting of Multinucleated Giant Cells (MNGCs) in a background of extravasated red blood cells and mononuclear stromal cells. Lesions can arise anywhere on the gingival or alveolar mucosa mostly anterior to the molar teeth [1,2]. The initiating stimulus has been believed to be due to local irritation or trauma, but the cause is not certainly known. PGCG has been termed “Reparative” granuloma, however it is reparative in fact has not been established and its osteoclastic activity nature appears as a questionable theory.
It has a membrane receptors for calcitonin demonstrated by immunohistochemistry also, its osteoclastic activity is evidences that the lesions are osteoclastic in nature when cultured in vitro [3,4]. In contrast, other authors have suggested that the lesion is originated from cells of the mononuclear phagocytic system [5]. The PGCG revealed a close microscopic similarity to the central giant cell granuloma and some researchers believe that it may represent a soft tissue counterpart of the intraosseous lesion. Case reports of PGCG in children have been documented in literatures to be more aggressive, with infiltration inside the interproximal crest area, with displacement or looseness of the adjacent teeth and multiple recurrences [6].
The aim of this case report is to illustrate an instance aggressive behavior of PGCG and to discuss reasonable differential diagnosis, based on the patient history, which is clinically significant in deciding the proper therapeutic management.
Case history
A 6-years-old male patient reported to the Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, October 6 University. He complained of massive lower gingival swelling in the past 5 months. History revealed that the swelling started as a small one and progressively increased to the present size over this duration. It was associated with pain on biting. There was no history of trauma, loss of appetite, loss of weight, fever or any neurological deficit. There was no similar swelling present in any other part of the body. The patient was medically free.
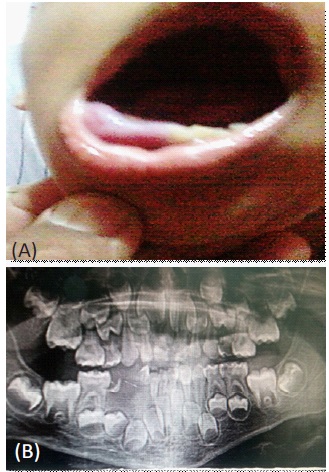
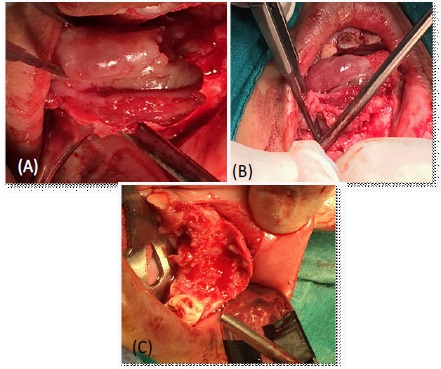
On clinical inspection, a single, diffuse swelling was seen on the right side of the mandible started from lower left central incisor crossing midline to lower right second molar. The swelling measured about 30 × 20 × 14 mm. The swelling was soft in consistency and bluish in colour, and the overlying mucosa was intact with no tendency of bleeding (Figure 1 A, B). No previous history of medical intervention was reported. Panoramic x-ray revealed just saucerisation of the alveolar bone. Surgical excision was performed under local anesthesia. Lesion was separated from the adjacent tissue by blunt dissection and removed in one piece (Figure 2A,B,C). All the related teeth were extracted due to their mobility. The specimen was sent for diagnosis through histopathologic examination.
Diagnosis
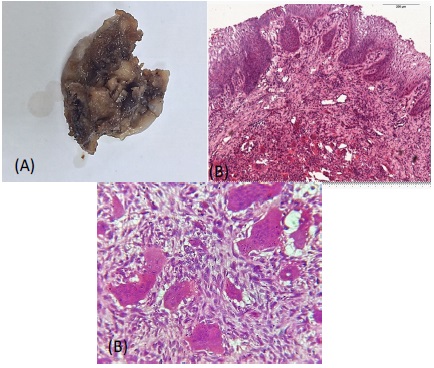
Gross examination of biopsy revealed oval whitish brown mass, soft in consistency and measuring about 25 × 16 × 10 mm in dimension. Histopathological examination revealed highly cellular connective tissue stroma consisting of proliferating plump fibroblasts in addition to unevenly distributed numerous giant cells of various shapes and sizes containing 8–15 nuclei, proliferating dilated endothelial lined blood capillaries and extravasated Red Blood Cells (RBCs). The covering mucosa was intact with some hyperplastic changes (Figure 3A,B,C).
Immunohistochemical analysis
Due to large size of the lesion, immunohistochemical study was performed by assessment the expression of CD34 as vascular endothelial marker and CD45 as osteoclastic marker to understand the nature & origin of these MNGCs.
Immuohistichemical results
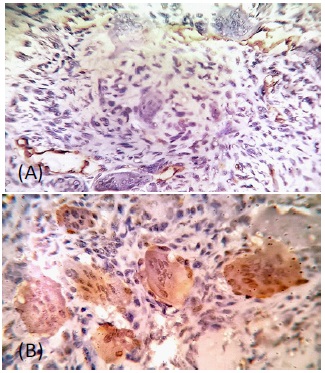
Immunopositivity for CD34 was seen in the cytoplasm of endothelial cells of blood vessels while negative expression was reported in MNGCs and stromal cells. On the other hand, cytoplasmic immunoreactivity for CD45 was observed in the MNGCs and few stromal cells (Figure 4 A,B).
Discussion
To provide appropriate treatment, the knowledge of the possible origin and nature of PGCG is very important, which remains uncertain. Previously, several hypotheses had been postulated to clarify the nature of MNGCs, including the explanation that they were osteoclasts, which left from reaction to injury to periosteum or physiological resorption of teeth. Strong evidence that these cells are osteoclasts have been shown as they retain receptors for calcitonin and were able to resorb bone in vitro [7]. Our results support the hypothesis of osteoclastic origin due to strong expression of CD45 in MNGCs. While PGCG occurs mostly in adults, some cases have been described in children where a more aggressive clinical behavior has been observed [8]. In the current work, positive expression of vascular endothelial marker CD34 may explain the rapid growth of the lesion. In children, it appears that PGCG similar to other reactive oral lesions have a rapid growth rate, be more aggressive with infiltration of adjacent tissues and bone resorption also, it may interfere with the eruption of adjacent teeth producing tooth displacement and have multiple recurrences [9]. Radiographic examinations are necessary for confirming the oral mucosa origin of the lesion and declining a central bony origin with cortical perforation and extending to soft tissues. Recurrence of PGCG is rare 5–11% but consequent loss of the adjacent teeth is a possible complication [10]. In the present case, rapid growth may be explained by proliferation of numerous blood vessels while loss of the related teeth may be explained by behavioral aggressiveness of the lesion due to osteoclastic origin.
Conclusion
Early and definite diagnosis correlating clinical, radiographic, and histopathologic examination especially in children is important for conservative management of such lesion thus eliminating potential risk of damage to adjacent teeth and tissues.
Conflict of interest: All authors declare that they have no conflict of interest.
Funding: This current work did not receive any grant from funding agencies or not for profit sector.
Ethical approval: This study was performed and approved by Research Ethics Committee at Faculty of Dentistry, October 6 University, Giza, Egypt (No. RECO6U/1-2021) and following the principles of the Declaration of Helsinki.
Consent: Written informed consent was received from the patient guardian explaining the entire surgical procedures and for publication involving the images.
References
- Kashyap B, Reddy SP, Desai R, Puranik RS, Vanaki SS. Computer assisted histomorphologic comparision and the expression of AgNORs in the central and peripheral giant cell lesions of the oral cavity and giant cell tumor of the long bone. J Oral Maxillofac Pathol. 2014; 18: 54–59.
- Lester SR, Cordell KG, Rosebush MS, Palaiologou AA, Maney P. Peripheral giant cell granulomas: A series of 279 cases. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014; 118: 475–482.
- Bonetti F, Pelosi G, Martignoni G, Mombello A, Zamboni G, et al. Peripheral giant cell granuloma: Evidence for osteoclastic differentiation. Oral Surg Oral Med Oral Pathol. 1990 ; 70: 471–475.
- Liu B, Yu SF, Li TJ. Multinucleated giant cells in various forms of giant cell containing lesions of the jaws express features of osteoclasts. J Oral Pathol Med. 2003; 32: 367–375.
- Abu Gharbyah AZ, Assaf M. Management of a peripheral giant cell granuloma in the esthetic area of upper jaw: A case report. Int J Surg Case Rep. 2014; 5: 779–782.
- Peacock ZS, Jordan RCK, Schmidt BL. Giant cell lesions of the jaws: Does the level of vascularity and angiogenesis correlate with behavior? J oral Maxillofac Surg Off J Am Assoc Oral Maxillofac Surg. 2012; 70: 1860–1866.
- Kfir Y, Buchner A, Hansen LS. Reactive lesions of the gingiva. A clinicopathological study of 741 cases. J Periodontol. 1980; 51: 655–661.
- Nekouei A, Eshghi A, Jafarnejadi P, Enshaei Z. A review and report of peripheral giant cell granuloma in a 4-year-old child. Case Rep Dent. 2016; 2016.
- Pandolfi PJ, Felefli S, Flaitz CM, Johnson J V. An aggressive peripheral giant cell granuloma in a child. J Clin Pediatr Dent. 1999; 23: 353–355.
- Fortes N, Bonne R, Manhique B. Peripheral giant cell granuloma - Case report. Rev Port Estomatol Med Dent e Cir Maxilofac. 2018; 59: 225–230.