
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Papillary carcinoma arising from thyroglossal duct cyst with cervical lymph node metastasis
Hadi Eslami1; Seyed Ali Hossein Zahraei2; Mandana Saberi3*
1 Associated Professor, Department of Otolaryngology, Head and Neck Surgery, Kerman University of Medical Sciences, Kerman, Iran.
2 Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran.
3 Resident of ENT, Department of Otolaryngology, Head and Neck Surgery, Kerman University of Medical Sciences, Kerman, Iran.
*Corresponding Author: Mandana Saberi
Resident of ENT, Department of Otolaryngology,
Head and Neck Surgery, Kerman University of
Medical Sciences, Kerman, Iran.
Email: mandana.saberi1991@gmail.com
Received : May 28, 2021
Accepted : Jul 05, 2021
Published : Jul 08, 2021
Archived : www.jcimcr.org
Copyright : © Saberi M (2021).
Abstract
Thyroglossal duct cyst carcinoma is uncommon. Its prevalence is less than one percent. Papillary carcinoma is the most common pathologic finding of the thyroglossal duct cyst carcinoma. Metastasis of the cervical lymph node is less common. Its prevalence is less than 8%. A 38-year-old woman presented with a complaint of painless mass in the midline of the neck. Ultrasonography of the neck revealed a solid cystic mass, measuring 5.5 × 2.5 cm in the submental area. Ultrasonography of the neck additionally revealed suspicion lymph node at bilateral level Ib. A preoperative Computed Tomography (CT) showed a 4 cm size MIX heterogeneous lesion in the anterior left-sided hyoid bone. The patient underwent sistrunk surgery, which was the result of the patient’s frozen section papillary carcinoma arising from the thyroglossal duct cyst. The patient had local metastasis to the neck, so she underwent total thyroidectomy and central N-D surgery and bilateral modified radical N-D.
Diagnosis of thyroglossal duct cyst carcinoma before surgery is unusual. The definitive diagnosis is often after surgery and is based on the patient’s histopathological findings.
The best surgical procedure is sistrunk. But if the patient has local metastasis to the neck, total thyroidectomy and modified radical N-D are performed.
Citation: Eslami H, Zahraei SAH, Saberi M. Papillary carcinoma arising from thyroglossal duct cyst with cervical lymph node metastasis. J Clin Images Med Case Rep. 2021; 2(4): 1222.
Introduction
Thyroglossal Duct Cysts (TDCs) is a common congenital anomaly during thyroid Gland development. This cyst is the most common midline neck mass in children. It is estimated that 7% of the population have this remnant in the thyroglossal duct. Most of the thyroglossal duct remnants are benign and the median age of involvement is 10 years [1,2].
TDC carcinoma is relatively rare and comprises 1% of all cases of thyroglossal duct cysts [3]. The median age of onset of this carcinoma is 40 years, and it is more prevalent in women than men in the ratio of 3 to 2 [4,5]. TDC carcinoma is clinically similar to benign thyroglossal duct cyst and is often an enlarging asymptomatic neck mass [6]. It may not be clinically distinguishable from benign thyroglossal cysts. It is often diagnosed at random after surgery.
In literature review, 250 cases of thyroglossal cyst carcinomas were reported. Percentage of different types of neoplasms included 1-papillary carcinoma 81.7% 2-papillary follicular carcinoma 6.9% 3- squamous cell carcinoma 5.5% 4-follicular adenocarcinoma 5% epidermoid and anaplastic carcinoma accounts for 0.9% [7].
The regional metastasis of the cervical node are less common prevalent in papillary carcinoma of the thyroglossal duct cyst than in the papillary carcinoma of the thyroid tissue that is primarily involved. Its prevalence is less than 8% [8]. The standard treatment is sistrunk surgery.
Case presentation
The patient is a 38-year-old woman with complaints of midline neck mass from three years ago with progressively incremental growth that presented and progressed rapidly within 2 to 3 months prior to presentation. The mass has been painless. The patient with it has no complaints of dysphonia, dysphagia, odynophagia and dyspnea. No complaints of fever and weight loss have previous radiation therapy.
On clinical examination, there is a firm, mobile mass that measured 2 × 4 cm in the midline and anterior neck, the mass moved with swallowing as well as on tongue protrusion. tongue mobility was intact. Thyroid function tests are normal.
Thyroid appearance is normal on ultrasound. The image of a solid cystic, hypoechoic mass with a specified size of 2.5 × 5.5 cm is seen in the submental area. Ultrasonography of the neck image shows three oval shape, hypo echoic with central echoic lymph nodes in the right and left submandibular area, the largest of which is 2.1 × 9 cm on the left. And on the right is 1.7 × 8 cm. Suspected cystic lymph node with an internal solid component of 2.6 × 1.6 cm is found in the right middle chain in the SCM muscle line, and cystic heterogeneous mass approximately 49 × 25 × 44 in the upper midline of the calcified thyroid cartilage. FNA was performed from the lateral neck mass. FNA metastatic carcinoma response was reported.
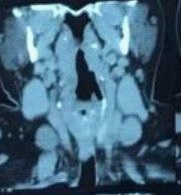
In Computed Tomography (CT), the thyroid lobes have normal. An image of a mixed lesion with a density heterogeneous is approximately 2 × 4 cm in the left anterior hyoid bone soft tissue (Figure 1,2).

The patient underwent sistrank surgery. During surgery, the entire cystic mass was removed along with the strap muscles and the body of the hyoid bone. The mass had adhesion to the infra-hyoid muscle around it. The frozen section of the patient's PTC thyroglossal duct cyst was reported. The patient had local metastasis to the neck, so the patient underwent total thyroidectomy and central Neck Dissection and bilateral modified Radical Neck Dissection performed.
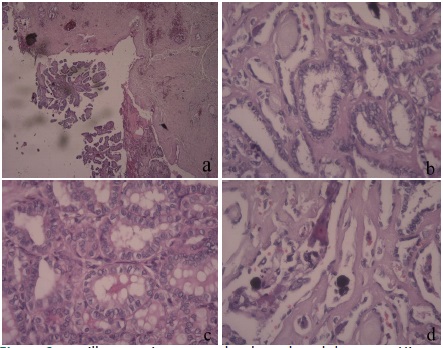
Pathologic findings confirmed the diagnosis of papillary carcinoma of the thyroglossal duct and thyroid gland. The dissected neck lymph nodes revealed metastatic papillary carcinoma. Microscopic analysis of the cystic lesion showed that the mass originated from the wall of the thyroglossal duct. The mass contains malignant cells with papillary arrangement and invades adjacent skeletal muscles (Figure 3).
The patient underwent iodine therapy following surgery and was re-treated 6 months and 12 months after surgery. There was no clinical or laboratory evidence of recurrence, and the patient's thyroglobulin level, finding ultra sonography was normal.
Discussion
During the third fetal week, the thyroid gland descends from the floor of the pharynx, where the foramen is called the cecum, and within a few weeks, the gland returns to its normal location in the anterior trachea. The epithelial interface between the thyroid gland and the foramen cecum of the thyroglossal duct is said to normally recede during embryonic development week 8-10. If this duct is not completely destroyed, the residual secretory epithelium may become a thyroglossal duct cyst [9].
The thyroglossal duct cyst is seen as a painless, growing mass in the midline in children and young adults, moving upward with tongue movement and swallowing [6,10-12].
Conversion of thyroglossal duct cysts to thyroglossal duct carcinomas is uncommon, with a prevalence rate of 0.7% to 1% of all thyroglossal duct cysts [12-14]. The most common pathologic finding of thyroglossal duct carcinoma are papillary carcinoma (75-80%) [15].
Preoperative evaluation of thyroglossal duct carcinoma includes physical examination, imaging findings, and FNA. The clinical findings of this carcinoma are very similar to benign thyroglossal cysts. However, a rapid increase in mass growth, firm and fix is more helpful in the diagnosis of thyroglossal duct cyst carcinoma. FNA is not always helpful in diagnosis. The sample size may not be sufficient so it may be useful in some patients.
In the management of patients with thyroglossal duct carcinoma prior to surgery, it is important to know whether the thyroid is in its normal location and whether the thyroid function is normal. Therefore, thyroid scan and thyroid function evaluation should be considered before surgery [16-18]. Imaging findings (ultrasound, CT, and MRI) can characterize the lesion (cystic or solid, capsulated, and vascularized) with invasive features and spread to surrounding tissue, assist in defining tumor stage, determining treatment planning are Useful [19]. The definitive diagnosis of thyroglossal duct cyst carcinoma is by microscopic evaluation of tissue specimen after surgical excision [20].
Sistrunk surgery is now used as treatment plan for all benign thyroglossal duct cysts in children [8]. In a reference study, there were many similarities between PTC thyroglssal duct cyst and thyroid PTC. These similarities are in multifocal, cervical lymph node metastasis and prognosis. Therefore, sistrank surgery recommended in PTC is less than one centimeter in size, and total thyroidectomy to the sistrunk operation did not have significant differents on recurrence and survival. total thyroidectomy and central ND are recommended for larger tumors and lateral ND in cases of cervical metastasis [12,21].
In this case, since we had a 4 cm mass and a lymph node involvement based on examination and imaging findings, sistrunk surgery, total thyroidectomy and central ND and bilateral modified radical ND were performed. The treatment plan for the patient after surgery is radioactive iodine therapy. The patient's prognosis is good after surgery. Six months after surgery, the patient underwent a clinical examination and ultrasound, with no evidence of recurrence, and a normal thyroglobulin level.
Conclusion
Thyroglossal duct cyst carcinoma is rare and one of the less common clinical symptoms is metastasis to the cervical lymph nodes. The best surgical procedure for thyroglossal duct carcinoma is sistrunk, but if the patient has concurrent local metastasis to the neck, a thyroidectomy with neck dissection is performed. Although the prognosis of the disease is good, patients need to be up-to-date to rule out recurrence.
Ethics approval: Due to there are no images of the patients to show their identity and also their names are anonymous, this process had not need any ethics approval ID.
References
- Fumarola A, et al. Thyroid papillary carcinoma arising in ectopic thyroid tissue within a neck branchial cyst. World journal of surgical oncology. 2006; 4: 24.
- Chao CS, et al. Thyroglossal duct cyst with papillary carcinoma. Chinese Medical Journal-Taipei. 2002; 65: 183-186.
- Motamed M, McGlashan JA. Thyroglossal duct carcinoma. Current opinion in otolaryngology & Head and Neck Surgery. 2004; 12: 106-109.
- Doshi SV, Cruz RM, Hilsinger RL. Thyroglossal duct carcinoma: Alarge case series. Annals of Otology, Rhinology & Laryngology. 2001; 110: 734-738.
- Asti J, et al. Coincidence of thyroid tumor and thyroglossal duct remnants. Review of literature and presentations of 3 cases. Tumori. 2003; 89: 314-320.
- Davenport M. ABC of general surgery in children: lumps and swellings of the head and neck. BMJ. 1996; 312: 368-371.
- Weiss S, Orlich C. Primary papillary carcinoma of a thyroglossal duct cyst: Report of a case and literature review. British journal of surgery. 1991; 78: 87-89.
- Allard RH. The thyroglossal cyst. Head & neck surgery. 1982; 5: 134-146.
- Patten B. Human Embryology.–Ed. 3. 1968, New York.–Mc GrawHill.–1968.
- Telander RL, Deane SA. Thyroglossal and branchial cleft cysts and sinuses Symposium on Head and Neck Surgery II. Surgical Clinics of North America. 1977; 57: 779-791.
- Telander RL, Filston HC. Review of head and neck lesions in infancy and childhood. Surgical Clinics of North America. 1992; 72: 1429-1447.
- Yang SI, Park KK, Kim JH. Papillary carcinoma arising from thyroglossal duct cyst with thyroid and lateral neck metastasis. International journal of surgery case reports. 2013; 4: 704-707.
- Heshmati HM. et al. Thyroglossal duct carcinoma: report of 12 cases. in Mayo Clinic Proceedings. Elsevier. 1997.
- Fernandez JF. et al. Thyroglossal duct carcinoma. Surgery. 1991; 110: 928-935.
- Vuuren PV. et al. Carcinoma arising in thyroglossal remnants. Clinical Otolaryngology & Allied Sciences. 1994; 19: 509-515.
- Kazemi M. et al. Primary papillary carcinoma in a thyroglossal duct cyst. Hellenic journal of nuclear medicine. 2006: 39-40.
- Chakeres D, Augustyn M. CT and MR Imaging of the Whole Body. Ohio: Mosby. Temporal bone. Haaga JR., Lanzieri CF, Gilkeson RC. 2003; 495-512.
- Aghaghazvini L. et al. Invasive thyroglossal duct cyst papillary carcinoma: A case report. Journal of medical case reports. 2009; 3: 9308.
- Gebbia V, Di Gregorio C, Attard M. Thyroglossal duct cyst carcinoma with concurrent thyroid carcinoma: A case report. Journal of medical case reports. 2008; 2: 132.
- Gordini L, et al. Tall cell carcinoma arising in a thyroglossal duct cyst: A case report. Annals of medicine and surgery. 2015; 4: 129-132.
- Hartl DM, et al. High rate of multifocality and occult lymph node metastases in papillary thyroid carcinoma arising in thyroglossal duct cysts. Annals of surgical oncology. 2009; 16: 2595-2601.