
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Axonal neuropathy immune-mediated by SARS-CoV2 (COVID-19): Report of two cases
Carvalho BM1; Silva MA1; Ferreira WSM1; Bentes RGL1; Bonsi VM1; Salzedas HT1; Schmid MF1; Freitas LF2; Marussi VHR2; Veiga VC3*; Prats JAG4; Baeta AM1
1 Department of Neurology, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
2 Department of Neuroradiology, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
3 Department of Neurointensivist, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
4 Department of Infectology, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil.
*Corresponding Author: Viviane Cordeiro Veiga
Department of Neurointensivist, BP - A Beneficência
Portuguesa de São Paulo, São Paulo, Brazil.
Email: viviane.veiga@bp.org.br
Received : May 31, 2021
Accepted : Jul 05, 2021
Published : Jul 08, 2021
Archived : www.jcimcr.org
Copyright : © Veiga VC (2021).
Keywords: COVID-19; Axonal neuropathy; Guillain-Barré syndrome; Neuronography
Citation: Veiga VC, Carvalho BM, Silva MA, Ferreira WSM, Bentes RGL, et al. Axonal neuropathy immune-mediated by SARSCoV2 (COVID-19): Report of two cases. J Clin Images Med Case Rep. 2021; 2(4): 1223.
Introduction
In 2020, the World Health Organization declare a SARS-CoV-2 pandemic. There are currently more than 10 million people infected. Mao et al [1] demonstrated that 36.4% of hospitalized patients diagnosed with Covid-19 have presented neurological manifestations, where the most severe patients are more likely to develop said manifestations, with a percentage of them having presented the neurological alteration as the initial manifestation of COVID-19.
Among the neurological manifestations of the disease already described, some authors have reported cases of GuillainBarré syndrome and its variants.
In this article, we will report on two cases of axonal neuropathy mediated by SARS-Cov2.
Case reports
Case 1
A 50-year-old woman started to develop a dry cough and a fever, associated with hyposmia and altered taste, and was diagnosed with COVID-19 by a PCR test. About two weeks after the infection, she developed horizontal diplopia and paresthesia in the mandibular region.
At the initial physical examination, she presented with hypoesthesia in bilateral trigeminal territory (V2 and V3), predominantly on the left, and paralysis of the VI cranial nerve. Tactile and painful sensitivity decreased in the distal extremity of upper limbs and overall areflexia. Motor strength was preserved in all 4 limbs.
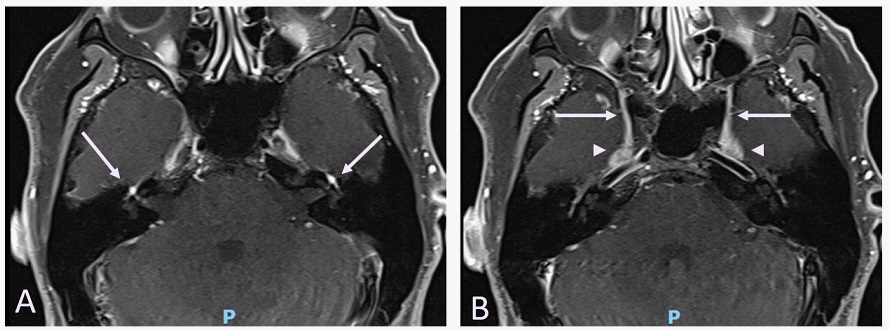
Magnetic resonance imaging of the brain (Figure 1) showed bilateral and symmetrical impregnation of the trigeminal nerves in the round and oval foramina, and of the facial nerves at the bottom of both the internal auditory canal, labyrinthine, tympanic segments and the geniculate ganglia. The imaging of the upper limbs showed thickening of the bilateral brachial plexus.
The CSF examination resulted in albumin-cytological dissociation (1.0 cells and 51 proteins). The anti Gq1b and Ganglioside antibodies were negative.
Electroneuromyography found axonal neuropathy with acute evolution, affecting the facial nerve bilaterally, more accentuated on the left, with signs of active denervation in muscles supplied by this nerve. In the upper and lower limbs, affecting sensitive and motor fibers with a predominantly symmetrical pattern and not dependent on length, suggesting a diagnosis of acute sensitive and motor axonal neuropathy (AMSAN).
She was treated with human immunoglobulin intravenous (0.4 g/kg) for 5 days. There was global clinical improvement resulting in the resolution of the diplopia, pain and paresthesia.
Case 2
A 27-year-old male was admitted due to symptoms of gastroparesis associated with gait disorders. Some 24 days before the evaluation he presented upper respiratory symptoms, hyposmia and a positive RT-PCR for COVID-19.
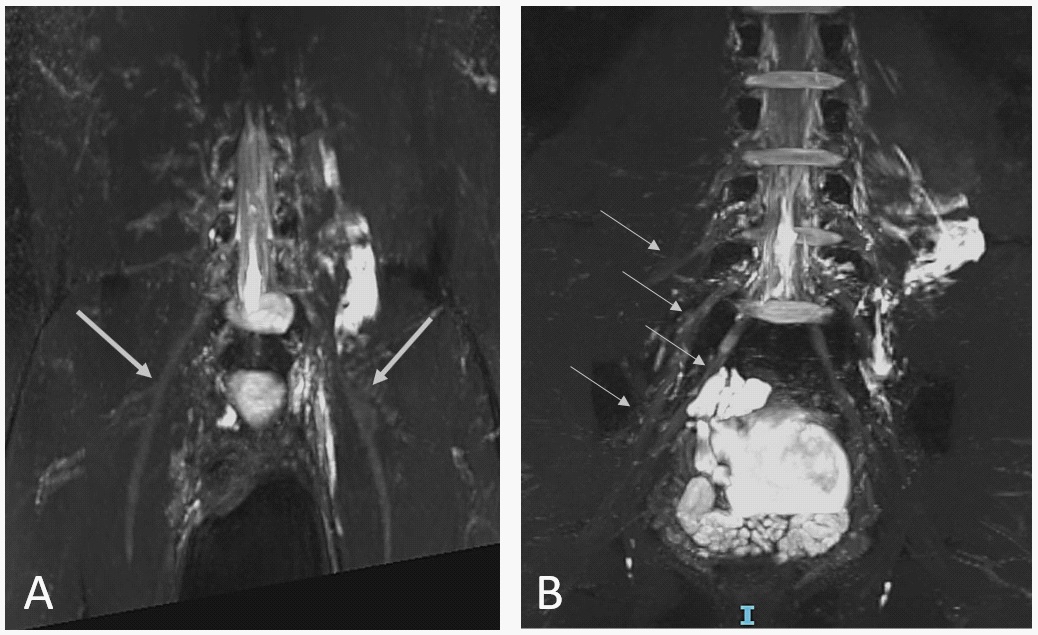
At the physical examination, he presented motor strength of 4+/5 according to MRC scale on proximal lower limbs and 4-/5 on distal. During hospitalization, he presented progressive worsening of motor symptoms, mainly in the proximal lower limbs and global hyperreflexia. The lumbosacral spine MRI showed diffuse thickening of the bilateral femoral nerves. CSF analysis was unremarkable. Electroneuromyography of the lower limbs was compatible with the diagnosis of acute axonal motor neuropathy of the lower limbs in a symmetrical pattern, suggesting Acute Motor Axonal Neuropathy (AMAN).
He was treated with human immunoglobulin intravenous (0.4 g/kg) for 5 days. After therapy, he presented partial improvement in neurological symptoms, being discharged with motor strength grade 4+/5 in his lower limbs.
Discussion
Ganglioside compounds are present in the pathogenesis of axonal immune mediated neuropathies and GBS [2], since the infection, induction of the production of anti-ganglioside IgG antibodies (GM1, GD1a and GD1b) is reported, injuring of Ranvier nodes and/or paranodal regions, being clinically associated with the presentations of AMAN, AMSAN, Miller Fisher and its variants [3,7].
Regarding COVID-19, it has been reported that the virus adheres to the cell membrane by the viral protein spike (S) that binds to the ACE 2 receptor and sialic acid - present in the glycoproteins and gangliosides on cell surfaces [4,5].
Possibly, the axonal neuropathy is immune-mediated by cross-reactivity, since the gangliosides present in the peripheral nerves exhibit conformation compatible with the N terminal of protein S, which the virus uses for neural invasion. However, it cannot be ruled out that this axonal dysfunction is also due to a direct viral injury. This is due to the fact that a proportion of the patients present hyposmia due to the direct cytopathic effects and may persist with this symptom despite treatment or as the only a neurological manifestation.
These two cases described show that we still need to better understand the pathophysiology of GBS associated with COVID-19. As both patients presented hyposmia and prolonged cases of peripheral nerve affection, it is necessary to define if the pathological mechanism is only immune-mediated or if the cellular invasion has a determining role in the mechanism by which these neurological complications occur.
References
- Mao L, Wang M, Chen S, He Q, Chang J, et al. Neurological Manifestations of Hospitalized Patients with COVID-19 in Wuhan, China: A retrospective case series study. MedRxiv. doi: https:// doi.org/10.1101/2020.02.22.20026500
- Yuki, N. Guillain–Barré syndrome and anti-ganglioside antibodies: a clinician–scientist’s journey. Proc. Jpn Acad. Ser. B Phys. Biol. Sci. 2012; 88: 299–326.
- Chiba A, Kusunoki S, Obata H,et al. Ganglioside composition of the human cranial nerves, with special reference to pathophysiology of Miller Fisher syndrome. Brain Res. 1997; 743: 32–36.
- Yuki K, Jufiogi M, Koutsogiannaki S. COVID-19 pathophysiology: A review. Clin Immunol 2020; 215: 108427.
- Fantini J, Scala CD, Chahinian H, et al. Structural and molecular modeling studies reveal a new mechanism of action of chloroquine and hydroxychloroquine against SARS- CoV-2 infection. Int J Antimicrob Agents. 2020; 105960.
- Dalakas MC. Guillain–Barré Syndrome: The first documented COVID19-triggered autoimmune neurological disease. Neurol Neuroimmunol Neuroinflamm. 2020.
- Gutierre-Ortiz C, Mendez A, Rodrigo-Rey S, et al. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology. 2020.