
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Openness to discuss cancer: Not only a matter of medical communication
Anne-Frédérique Naviaux2,3* Pascal Janne4; Alan Bradish5; Maximilien Gourdin1,2
1 Université catholique de Louvain, Département d’Anesthésiologie, CHU UCL Namur, Yvoir, Belgium, USERN.
2 Faculté de Medecine, Université catholique de Louvain, Avenue Emmanuel Mounier 50, B-1200 Woluwé-Saint-Lambert, Belgium, USERN.
3 College of Psychiatrists of Ireland, Health Service Executive (HSE) Summerhill Community Mental Health Service, Summer Hill, Wexford, W35 KC58, Ireland, USERN.
4 Faculté de Psychologie, Université catholique de Louvain, Place Cardinal Mercier 10, 1348 Ottignies-Louvain-la-Neuve, Belgium, USERN.
5 University College, (HONS°) Belfield, Dublin 4, www.near.ie, RCN 20205453.
*Corresponding Author: Anne-Frédérique Naviaux
Université catholique de Louvain, Département
d’Anesthésiologie, CHU UCL Namur, Yvoir, Belgium, USERN.
Email: annefrederique.naviaux@hse.ie
Received : May 31, 2021
Accepted : Jul 05, 2021
Published : Jul 08, 2021
Archived : www.jcimcr.org
Copyright : © Naviaux AF (2021).
Citation: Naviaux AF, Janne P, Bradish A, Gourdin M. Openness to discuss cancer: Not only a matter of medical communication. J Clin Images Med Case Rep. 2021; 2(4): 1224.
Introduction
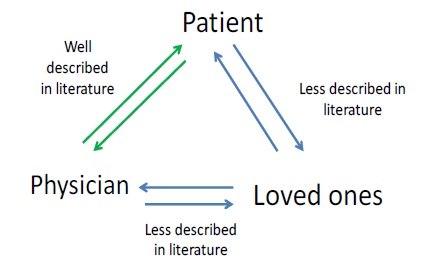
Though many studies have been made - sometimes even blaming - to optimize the communication between doctor-patient-caregiver in oncology, very little work is focused on the intra-familial aspects of the communication [1-5].
Clinical experience shows us how much communication between cancer patients and their loved ones can also be impacted by cancer: We will refer to this phenomenon as “Communicative Cancer”. In fact, as soon as the communication of the diagnosis is made, perverse effects can quickly occur due to at least two mechanisms: the defense mechanisms of the patient and his entourage and the significant deterioration of communication between the patient and his loved ones [6,7].
While various articles have blamed, sometimes perhaps rightly so, the way the oncologist communicates with his/her patient (s), it is seldom mentioned how difficult and strenuous communicating with his patient and those around him, can be for the physician: In fact the frequency of denial mechanisms in the patient ranges from 4 to 47% on the diagnosis, from 8 to% to 70% on the impact and from 18 to 42% on the affects [7,8].
There is little work available about the consequent communicational disturbances between the patient and his relatives.
Here are a few examples
A man is bedridden in hospital; his wife and children come to
visit him. Before entering the room, the visitors dry their tears, come in and tell the patient: “You look good” and develop mundane conversations, deliberately omitting the fact that the son
has just had an accident with the family car (which has to be
repaired) and the bad school results of the daughter.
On his side, the patient does his best not to show how he really feels as he does not want to burden his family with his own issues.
And so appears communicational cancer: The sake of mutual protection generates, most of the time, both a distortion of communication and a concealing of information; which kills communication and by transitivity contributes to exclude the patient from access to real life (like a plant that no longer has access to light). The communication is afflicted both digitally (words, vocabulary) and by analog means (non-verbal, expressions and attitudes): Looks are avoided... and touch is reduced. Hell is paved with good intentions...
Some families can become too close to the therapeutic/ treating team where others decide to question the quality of care.
Secrets are sometimes generated between different family members, including the patient who can decide to hide parts of his communication with the doctor. Telephone communications and emails can be dangerous, especially when the family contacts the doctor behind the patient’s back in order to either get or provide additional information about the patient.
Therefore we can conclude:
a) That optimizing doctor-patient communication is no easy
task,
b) That the doctor is confronted with an iceberg of which he
can only see the top, and
c) That a great deal of research has incriminated the doctor’s way of communicating without taking these hidden
parameters into account.
One way to prevent these misunderstandings is to “Metacommunicate” - that is, to communicate about the relationship - by asking the patient if he has provided all information he intended to or by proceeding to a virtual circular questioning of the patient, for example: If your wife was there, what would she say about you?.
References
- Doyon K, Reblin M, Ellington L. An Exploration of Questions from Informal Family Caregivers of Cancer Patients in Home Hospice (RP418). Journal of Pain and Symptom Management. 2020; 60: 224-225.
- Goldsmith J, Wittenberg E, Platt CS, Iannarino NT, Reno J. Family caregiver communication in oncology: Advancing a typology. Psychooncology. 2016; 25: 463-470.
- Meier F, Cairo Notari S, Bodenmann G, Revenson TA, Favez N. We are in this together - Aren’t we? Congruence of common dyadic coping and psychological distress of couples facing breast cancer. Psychooncology. 2019; 28: 2374-2381.
- Noordman J, Schulze L, Roodbeen R, Boland G, van Vliet LM, et al. Instrumental and affective communication with patients with limited health literacy in the palliative phase of cancer or COPD. BMC palliative care. 2020; 7: 19: 152.
- Zettl S. How couples and families speak about that which they cannot say. Deutsche Zeitschrift fur Onkologie. 2016; 48: 178- 181.
- Gros A-M, Duffaud F, Dudoit É, Favre R. Déni ou… relégation. Le cancer: Approche psychodynamique chez l’adulte. Toulouse: ERES. 2004; 179-186.
- Vos MS, de Haes JC. Denial in cancer patients, an explorative review. Psychooncology. 2007; 16: 12-25.