
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Multidrug-resistant klebsiella pneumoniae-induced sepsis with multiple abscesses: A case report
Ye Xiong; Jianrong Huang*
State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, China
*Corresponding Author: Jianrong Huang
State Key Laboratory for Diagnosis and Treatment
of Infectious Diseases, The First Affiliated Hospital,
Zhejiang University School of Medicine, 79 Qingchun
Road, Hangzhou, 310003, China
Email: hzhuangchina@zju.edu.cn
Received : May 31, 2021
Accepted : Jul 06, 2021
Published : Jul 10, 2021
Archived : www.jcimcr.org
Copyright : © Huang J (2021).
Keywords: Multidrug-resistant klebsiella pneumonia; sepsis; multiple abscesses; comprehensive treatment.
Citation: Xiong Y, Huang J. Multidrug-resistant Klebsiella pneumoniae-induced sepsis with multiple abscesses: A case report. J Clin Images Med Case Rep. 2021; 2(4): 1226.
Introduction
Klebsiella pneumoniae, a Gram-negative bacillus which exists widely in nature, is generally colonized in the human intestine and oral cavity and does not cause disease [1]. However, the emergence and global expansion of hypervirulent and multidrug-resistant clones of K. pneumoniae have been increasingly reported in community-acquired and nosocomial infections. Management of antimicrobial resistance in multi-drug-resistant-K. pneumoniae (MDR-KP) is a major challenge for clinicians [2]. The optimal treatment option for MDR-KP infections is still not well established, which brings huge challenges to clinical treatment [2].
Here, we report a case of septicemia caused by MDR-KP with hibateral perirenal abscesses, hibateral psoas abscesses and right posterior abdominal wall abscess in a 70-year-old man who are treated for a long time.
Case report
A 70-year-old man who had a 15-year history of hypertension controlled with oral anti-hypertension agents was admitted to a local hospital for fever up to 40 with chills. Laboratory tests revealed a raised white blood cell count (129700 /ml) with 89% neutrophils, a hemoglobin level of 84 g/L, and a platelet count of 95000 /ml. Blood analysis did reveal an increase in C-reactive protein (185.82 mg/L) and procalcitonin (6.37 ng/ml). Blood cultures were positive for K. pneumoniae, which was found to be multi-drug-resistant strains and sensitive to sulfamethamine. Other detailed information about bacterial cultures and antibiotic treatments in the local hospital was unavailable. The patient was diagnosed with sepsis induced by MDR-KP, and only received treatment with intravenous antibiotic and oral antibiotic without other treatments. During this period, the patient still had a low fever. Five months later, he had a recurrence of fever up to 39 with chills and declined oxygen saturation and blood pressure transient. Therefore, the patient was transferred to our hospital for further treatment.
Upon admission (September 5, 2019), physical examination of the patient showed poor mental status with a body temperature of 38.4°C, a blood pressure of 96/58 mmHg, a pulse rate of 100 beats/min, and a respiration rate of 20 breaths/min. The genital examination revealed a mass in the right groin, which was fluctuating with obvious tenderness.
Blood analysis showed signs of inflammation: a C-reactive protein (CRP) level of 244 mg/L, a procalcitonin level of 1.28 ng/ml and an Erythrocyte Sedimentation Rate (ESR) level of 53 mm/h. The white blood cell count raised to 16100/ml with 79.6% neutrophils, a hemoglobin level of 87 g/dL, and a platelet count of 85000 /ml. His Laboratory test results of liver function revealed a total protein of 57.3 g/L, an albumin of 33.5 g/L, and an increased glutamyltranspetidase (394 U/L). Urine testing showed an increase in leukocytes (65.3 /UL) and epithelial cells (16.8 /UL). Renal ultrasound revealed multiple cystic dark areas in the renal parenchyma suggesting multiple renal cysts. Ultrasound of the right groin showed a strip-shaped, hybrid-echoic mass.
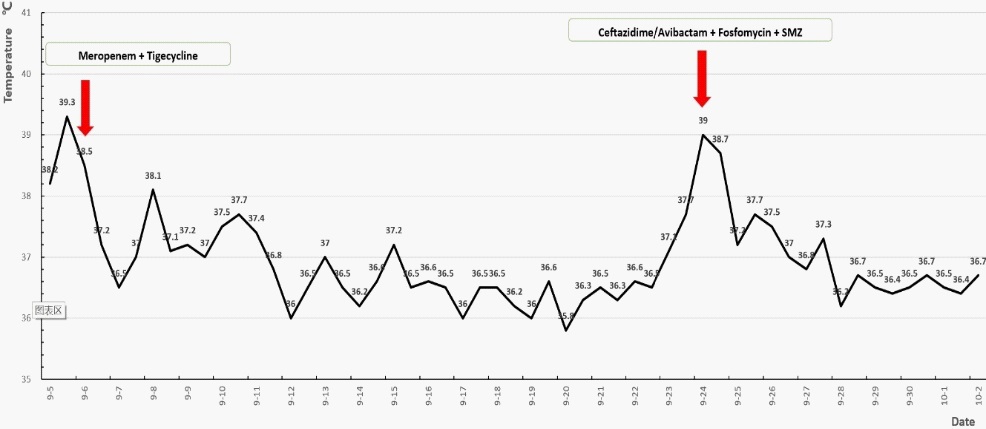
On day 2 (September 6, 2019), the patient started receiving treatment with meropenem (500 mg, q6h, intravenous drip [i. v. D]) combined with tigecycline (50 mg, q12h, i. v. D). Meanwhile, he received thymic peptide and parenteral nutrition to improve his immunity. The inguinal mass was punctured and drained. Culture of drainage fluid indicated the growth of K. pneumoniae, which was resistant to all routinely tested antibiotics except tigecycline (Table 1). Owing to the results of drug susceptibility testing, we started to treat the patient with tegacycline (50 mg, q12h, i. v. D). After five days of treatment with tegacycline, his fever resolved and the inflammatory biomarkers continuously decreased. The inguinal mass decreased significantly. Therefore, the drainage tube was later removed. But the treatment of antibiotics continued.
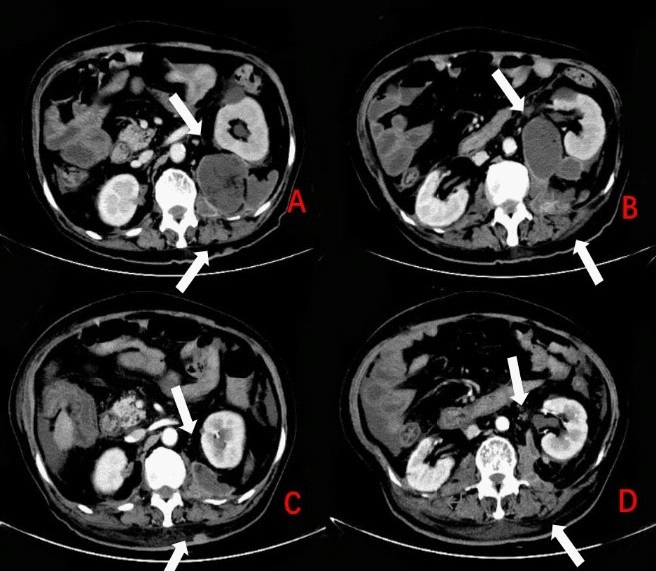
However, on day 20 (September 24, 2019) after admission, the patient had a recurrence of fever up to 38.7o C (Figure 1). Laboratory findings revealed an increased white blood cell count (11300 /ml) with 94.4% neutrophils, a hemoglobin level of 73 g/L, and a platelet count of 43000 /ml, CRP level of 184.71 mg/L, and a procalcitonin level of 2.49 ng/ml. A Computed Tomographic (CT) scan of the abdomen detected irregular liquid accumulation and hibateral perirenal abscesses, hibateral psosa abscesses and right latissimus dorsi abscess (Figure 2A, Figure 2B). The hibateral renal abscesses were drained under ultrason ographic guidance. Gram stain and cultures of pus showed presence of K. pneumoniae, which was only sensitive to SulfaMethoxazole (SMZ) (Table 1). Based on the results of antibiotic susceptibility tests and persistent reduction of platelet count, the initial antibiotic regimen was changed to ceftazidime/avibactam (2.5 g qd, i.v.D) and SMZ (0.96 g bid, Oral administration). To prevent the occurrence of circulatory failure, urinastatin was used to improve immunity. His symptoms improved gradually. Ultimately, the drainage of kidneys remained in place for about four weeks and the patient was treated with a total course of two months of antibiotic therapy, which resulted in a relief of symptoms. Patient was discharged from hospital. A month later, during the outpatient follow-up, the abdominal CT showed that the abscesses and empyema were obviously absorbed (Figure 2C,D). After 10 months of follow-up, the patient regained his health eventually.
Table 1: Klebsiella pneumoniae isolates antibiotic susceptibility tests at different dates
|
Antibiotic |
Phenotype |
MIC ug/ml |
|
Antibiotic |
Phenotype |
MIC ug/ml |
|
September 6th , 2019 |
Ampicillin |
R |
6 |
September |
Ceftriaxone |
R |
≥64
|
|
|
|
|
|
|
|
|
|
|
Discussion
Since the advent of the first antibiotic penicillin in 1940s, the clinical application of antibiotics has ushered in a new era in the treatment of infectious diseases and saved countless lives [3]. However, due to the changes of pathogens and the abuse of antibiotics, many bacteria have developed severe resistance to antimicrobial drugs [3]. In this case report, we described a case of septicemia, which induced systemic, multiple abscesses. The treatment period of the patient was very long and his condition was severe and repeated. The causative organism was MDR-KP, in which drug resistance developed rapidly [3]. Relevant literature points out that because of the limited choice of treatment, infections caused by Multi-Drug-Resistant Organisms (MDROs) are especially troublesome [3,4]. For patient with a sepsis caused by MDR-KP, measures must be taken to prevent the occurrence of a wide range of infections. The patient should be treated in isolation. Medical staffs must follow strict hand hygiene principles. Besides, specialized cleaning appliances should be equipped to clean and disinfect the isolation wards and the patient's medical waste should be strictly managed. Importantly, the therapeutic regimen should be comprehensive. Antibiotic treatment, drainage of abscesses, enhancement of immunity and nutrition of patients are all very crucial for the recovery of patients. Susceptibility testing results are significant and predictive. The combination of antibiotics needs to be adjusted according to the antimicrobial susceptibility test results, assessment of the illness, and therapeutic effect of the antibiotics in vivo [5]. Drainage must be evaluated in patients with multiple abscesses. In this case, the patient’s body temperature returned to normal after the initial antibiotic treatment, but the presence of abscesses went unnoticed in the imaging. Consequently, the fever recurred and the condition was even more severe than before. When dealing with MDR-KP induced sepsis, imaging of organs is of great importance in discovering the abscesses, draining the lesions timely, and therefore substantially alleviating the inflammatory state of patients. Patients with sepsis have poor physique, severe symptoms, and the course of the disease can last for a long time, especially when the pathogen is multi-drug resistant bacteria. Therefore, while applying sensitive antibacterial treatment, attention should also be paid to replenish thymic peptide and albumin to enhance the immunity of patients and reduce the occurrence of bacterial translocation. Supplementation of enteral nutrition can build up patient’s resistance to diseases.
Conclusion
Here, we shared a case of comprehensive treatment of MDR-KP. Nowadays, although cases caused by MDR-KP are not uncommon, this case provides a concept of comprehensive treatment integrating therapeutic regimen of selected sensitive antibiotics and supplements of thymic peptide and parenteral nutrition, which is beneficial to the recovery of patients. This case report also emphasizes the importance of the guidance of antibiotic susceptibility tests, imaging results and isolation measurements.
Acknowledgments: We thank the radiological technicians and the staffs of Department of Infectious Diseases for their efforts in the clinical diagnosis and management of the patient.
Author contributions: YX performed the clinical assessments and drafted the manuscript. JH was responsible for clinical care of the patient, assisted in drafting and revised the manuscript. Both authors read and approved the final version of the manuscript.
Ethics statement: Written consent for case publication was obtained from the patient.
References
- Qian Y, Wong CC, Lai SC, et al. Klebsiella pneumoniae invasive liver abscess syndrome with purulent meningitis and septic shock: A case from mainland China. World J Gastroenterol. 2016; 22: 2861-2866.
- Bassetti M, Righi E, Carnelutti A, Graziano E, Russo A. Multidrugresistant Klebsiella pneumoniae: Challenges for treatment, prevention and infection control. Expert Rev Anti Infect Ther. 2018; 16: 749-761.
- Qu J, Huang Y, Lv X. Crisis of antimicrobial resistance in China: Now and the future. Front Microbiol. 2019; 10: 2240.
- Babady NE. Hospital-Associated Infections. Microbiol Spectr. 2016; 4.
- Wang B, Zhang P, Li Y, Wang Y. Klebsiella pneumoniae-induced multiple invasive abscesses: A case report and literature review. Medicine. 2019; 98: e17362.