
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Effects of electroacupuncture on the premenstrual syndrome: A randomized clinical trial
Hongying Kuang1ϯ; Jing Lin2ϯ; Li Zhang3; Mushan Li4; Fan Gao5; Zhenxia Shao6; Kexin Ma7; Jingjing Chen8; Ziyu Yang9; Simao Shi1; Xiaoling Feng1*
1 Second Department of Gynecology, The 1st Affiliated Hospital to Heilongjiang University of Traditional Chinese Medicine, Harbin, China.
2 Traditional Chinese Medicine Department, The 2nd Affiliated Hospital of Harbin Medical University, Harbin, China.
3 Graduate School, Hebei University of Chinese Medicine, Shijiazhuang, China.
4 Graduate School, Heilongjiang University of Traditional Chinese Medicine, Harbin, China.
5 First Department of Oncology, Heilongjiang Infectious Disease Prevention and Control Hospital, Harbin, China.
6 Department of Gynecology, Shaoxing No. 2 Hospital Medical Community General Hospital, Shaoxing, China.
7 Obstetrics and Gynecology Department, Zhaoqing Dinghu District Hospital of Traditional Chinese Medicine, Zhaoqing, China.
8 Second Zone of Gynecological Tumor, The Second People’s Hospital of JiaoZuo, JiaoZuo, China.
9 Acupuncture Department, Shenzhen Pingle Orthopedic Hospital (Shenzhen Pingshan Hospital of Traditional Chinese Medicine), Shenzhen, China.
*Corresponding Author: Xiaoling Feng
Second Department of Gynecology, The 1st Affiliated
Hospital to Heilongjiang University of Traditional
Chinese Medicine, Harbin, China.
Email: doctorfxl@163.com
Received : Jul 06, 2021
Accepted : Jul 08, 2021
Published : Jul 12, 2021
Archived : www.jcimcr.org
Copyright : © Feng X (2021).
Abstract
Objective: The purpose of this study was to evaluate the effect and possible mechanism of electroacupuncture on Premenstrual Syndrome (PMS).
Method: From May 2018 to December 2018, 60 participants who met the criteria were selected and divided randomly into either the Electroacupuncture (EA) group or the Placebo (PA) group. Three courses of treatment were provided. During the treatment, the main symptoms and signs of moderate and severe PMS in each menstrual cycle were recorded by filling in DRSP, HAMA, and HAMD. The hormone levels were detected in the luteal phase.
Results: Compared with the PA group, the scores of symptoms and sign dimension and influence dimension changed significantly from the first cycle in the EA group; the scores of emotion dimension and the total score changed significantly from the second cycle in the EA group. The total effective rate of the EA group was significantly higher than that of the PA group. The level of Progesterone (P) and allopregnanolone increased significantly in the EA group. 1,25-(OH)2D decreased significantly in the EA group after treatment. Corticotropin Releasing Hormone (CRH) and Adrenocorticotropic Hormone (ACTH) decreased significantly in the EA group after treatment. Dopamine (DA), 5-Hydroxytryptamine (5-HT), Noradrenaline (NA), beta Endorphin (β-EP), Gamma Aminobutyric Acid (GABA), Glutamate (Glu) and Glu/GABA changed significantly in the EA group after treatment. Prostaglandin F2α (PGF2α) and Prostaglandin E2 (PGE2) had significant changes after treatment in the EA group.
Conclusion: Electroacupuncture is effective to treat PMS, which may be alleviated by regulating P, allopregnanolone, 1,25-(OH)2D, CRH, ACTH, 5-HT, DA, NA, β – EP, GABA, Glu, Glu/GABA, PGF2 α and PGE2.
Keywords: Premenstrual syndrome; electroacupuncture; DRSP; serum hormone.
Citation: Feng X, Kuang H, Lin J, Zhang L, Li M, et al. Effects of electroacupuncture on the premenstrual syndrome: A randomized clinical trial. J Clin Images Med Case Rep. 2021; 2(4): 1228.
Introduction
Premenstrual Syndrome (PMS) is a common disease in women at childbearing age [1]. It is a collection of periodic symptoms of cognition, emotion, physiology, and behavior that occur in the luteal phase of the menstrual cycle [2]. Back joint and muscle pain are the most common symptoms, followed by abdominal heaviness and discomfort [3]. PMS disappears at the beginning of menstruation or within a few days after menstruation, which has a significant negative impact on women’s quality of life [4]. Most of the symptoms are moderate, and severe, and severe ones are rare [5].
Some studies have shown that about 80-90% of women go through at least one experience of PMS; among about 2.5-3% of women, this syndrome has a very serious impact on their personal activities and social interaction [6]. According to different investigations on the prevalence of PMS, the frequency of PMS varies greatly according to the methods and evaluation tools used [7,8]. Overall, the results show that up to 90% of women of childbearing age experience premenstrual symptoms ranging from mild to severe; about 20-40% of women experience premenstrual syndrome, and 2-8% of women suffer from Premenstrual Dysphoric Disorder (PMDD) [9].
Acupuncture and the use of meridians have long been used to treat various pathological conditions. Acupuncture needle, whether operated manually or stimulated with low current and frequency, has been proved to be the neurophysiological basis for regulating peripheral and central nerve pathway activities [10]. In recent years, the discovery of the acupuncture mechanism reveals that acupoints are rich in sensory receptors [11]. Acupuncture has a history of traditional use in China for women’s health conditions including PMS [12], but its effectiveness for this condition remains unclear. Some systematic reviews suggest that the overall effect of acupuncture on PMS is better than that of sham acupuncture and related drugs, and acupuncture has a higher effective rate on PMS. The most commonly used acupoints in the treatment of PMS are SP6, LR3, and RN4 [13-15].
At present, the pathophysiology of PMS is still unclear. Some researchers believe that the fluctuation of female reproductive hormones can lead to PMS [16]. Some people think that the secretion of some neurotransmitters, such asγ - aminobutyric acid and catecholamine, leads to PMS [17,18]. Others think that insufficient secretion of adrenal hormones and imbalance of body electrolytes are the causes of these symptoms [19].
However, the effect and the possible mechanism of electroacupuncture on PMS are unclear. The purpose of this study was to evaluate the effect and the possible mechanism of electroacupuncture on PMS, and to compare Electroacupuncture (EA) with Placebo Acupuncture (PA) in treating PMS.
Methods
Design and process.
From May 2018 to December 2018, 60 college students and teachers who underwent university-wide, outpatient physical examination in Harbin, China, and who met the eligibility criteria were recruited. They were divided randomly into the EA group and PA group according to the ratio of 1:1. The EA group received dialectical acupuncture treatment. The PA group was treated with sham acupuncture. Before treatment, in every treatment cycle and two months after treatment, the scales were filled in and blood samples were collected. The two groups of participants were treated separately by appointment to ensure that they did not know each other’s efficacy and observation indicators, and that only acupuncture doctors and statisticians knew the grouping of the participants. The participants were followed up two months after treatment. Finally, all data were reviewed and verified for completeness and accuracy.
Recruitment of participants
From May 2018 to December 2018, the teachers and students were advertised to join the experiment voluntarily in Heilongjiang University of Traditional Chinese Medicine. Those who met the inclusion and exclusion criteria of the experiment were randomly divided into the EA or PA group with a proportion of 1:1. After a detailed introduction, they signed the informed consent form. A copy of the signed consent was provided.
Inclusion criteria were as follows: 1) Women aged between 18 and 35, who met the diagnostic criteria of moderate and severe PMS. 2) The regularity of menstrual cycle is 28-35 days. 3) Voluntarily participate in the experiment and sign the informed consent. 4) The total score of Daily Record of Severity of Problems (DRSP ) in the first five days of two consecutive menstrual cycles is greater than or equal to 130 points.
Exclusion criteria are as follows: 1) suffering from serious heart, brain, and kidney diseases, hypertension, diabetes, and so on. 2) Past six months of treatment for PMS. 3) Receiving other drugs in the past month. 4) It is anticipated that during the study period, patients with more than one menstrual cycle need to be discontinued. Unwilling for being followed up as required (telephone or e-mail follow-up). 5) Participated with other clinical researchers in the past month. 6) Received psychiatric drugs or other medications affecting the study in the past six months. 7) Pregnant or planning pregnancy. 8) Pelvic ultrasound had any organic lesions. 9) Had a history of mental illness including alcohol and drug abuse, attempted suicide, and severe personality disorders. Alcohol abuse is defined as > 14 cups per week or binge drinking. 10) Took analgesics in the past month. 11) Acupuncture was given in the past six months.
Criteria for elimination and abscission of the clinical trial are as follows: 1) Those who cannot continue with treatment. 2) Those with severe side effects. 3) Those with severe complications and adverse events. 4) Those who had worsened symptoms and needed emergency treatment during treatment. 5) Those who requested to withdraw from the trial. 6) Those who failed to complete at least 70% of the treatment within the prescribed time (less than four times in a course). 7) Those who used the treatment prohibited in this study exclusion criteria. 8) Those who changed the treatment method by themselves.
Acupressure
Electroacupuncture group: The main points are Zhongji (CV3), Guanyuan (CV4), Zusanli (ST36), Sanyinjiao (SP6), Taichong (LR3), Hegu (LI4), Baihui (GV20) and Shenmen (HT7). More than two acupoints should be needled at a time, and the specific acupoint selection should be changed according to the doctor’s clinical judgment and syndrome differentiation (Table 1).
Table 1: Locations of main acupoints.
Acupoint |
Location |
Zhongji (CV3) |
The lower abdomen, on the anterior midline, is 4 inches below the middle of the umbilicus. |
Guanyuan (CV4) |
The lower abdomen, on the anterior midline, is 3 inches below the middle of the umbilicus. |
Zusanli (ST36) |
On the anterolateral side of the leg, 3 inches below the Dubi (ST35), a transverse finger (middle finger) from the front of the tibia. |
Sanyinjiao (SP6) |
On the inner side of the leg, 3 inches above the tip of the inner ankle of the foot and behind the medial margin of the tibia. |
Taichong (LR3) |
On the dorsolateral side of the foot, the posterior depression of the first metatarsal space. |
Hegu (LI4) |
On the back of the hand, between the first and second metacarpals, at the midpoint of the radial side of the second metacarpal. |
Baihui (GV20) |
In the head, 5 inches straight up the middle of the front hairline, or the middle of the line between the two ear tips. |
Shenmen (HT7) |
At the wrist, the ulnar end of the carpometacarpal transverse line and the radial depression of the flexor carpi ulnaris tendon. |
Acupuncture and moxibustion were used for participants with abdominal cold accompanied by dysmenorrhea. For headache and dizziness, add Yintang (Ex-HN03), Baihui (DU20), and Hegu (LI04); For those with large emotional fluctuation and insomnia, add Neiguan (PC06), Sishencong (Ex-HN01), Tongli (HT05) and Daling (PC07); For breast distension, hypochondriac pain, chest tightness and shortness of breath, the participants are treated with Qi Men (LR14), Qu Ze (PC03), Shangqiu (SP05); Edema plus Yinlingquan (SP09), Water (RN09), Sun (SP04); Diarrhea plus Zhongwan (RN12) and Tianshu (ST25); For fever participants, Dazhui (DU14) and Quchi (LI11) are added.
Participants in the EA group will receive 21 sessions of acupuncture during 3 menstrual cycles, implemented by finding the gather and knot of positive reaction, the points of both stress concentration and neurogenic stimulation according to TCM theory and modern biomechanical principles of soft tissue. Using a 0.30 mm × 0.40 mm filiform needle, and then entering the needle to make sure of getting Deqi, doctors connect the electric acupuncture instrument (Huatuo brand SDZ-II electronic acupuncture instrument), take the density wave, and keep the needle for 20-30 min.
Placebo acupuncture group: This group was non-meridian non-acupoint shallow needling, and the acupoint selection site was 1 inch away from the acupoint selection in the treatment group. The superficial layer of acupoint skin was 0.5 cm, and no manipulation was allowed after the skin was punctured. The acupuncture needle was connected with the electroacupuncture instrument, and the special power cord and electrode were connected (one end of the power cord was cut off as the special power cord, the appearance was consistent with the normal power cord; there was no current output).
Every 3 days before menstruation to the 4th day of menstruation, acupuncture treatment was carried out. One menstrual cycle was one course of treatment. This whole study had 3 courses of treatment.
Observation indicators and methods
DRSP questionnaire: DRSP was divided into three dimensions: emotional change dimension, symptom and sign dimension, and influence dimension. DRSP scores were evaluated at 5 time points: before treatment, after the first treatment cycle, after the second treatment cycle and after the third treatment cycle, and 2 months after the end of treatment. The total score of 5 days before menstruation that was more than 130 points was diagnosed as moderate premenstrual syndrome, more than 180 points as severe premenstrual syndrome, and more than 230 points as extremely severe premenstrual syndrome.
Hamilton Anxiety (HAMA): HAMA was used to evaluate the anxiety level of participants. All patients filled in HAMA scale twice (before and after treatment). Total score ≥ 29 was severe anxiety, total score ≥ 21 and < 29 was moderate anxiety, total score ≥ 14 and <21 was mild anxiety, and total score ≥ 7 might have anxiety
Hamilton Depression (HAMD): HAMD was used to evaluate the depression degree of the participants. All participants filled in HAMD scale twice (before and after treatment). The total score of HAMD ≥ 24 was severe depression, the total score ≥ 17 and <24 was moderate depression, and the total score ≥ 8 and < 17 was mild depression
Serum hormone: Before and after treatment, 5 ml blood of the participants was collected in the luteal phase (the 21st-25th day of menstruation), and centrifuged after standing. The upper serum was separated and stored in - 80o C refrigerator. The levels of E2, P, allopregnanolone, 1,25-(OH)2D, PRL, CRH, ACTH, PTH, 5-HT, DA, NA, β-EP, GABA, Glu, PGF2α, PGF1α, PFE1, PGE2, TXB2 were measured by enzyme-linked immunosorbent assay (with the assistance of the isotope Department of the First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine).
Data analysis
Before the study began, the study coordinators received uniform training. The scale scoring data before and after treatment were stored in a computer, and SPSS22.0 statistical software was used. Descriptive statistics were presented for median (interquartile spacing), mean (standard deviation), and proportion (95% confidence interval of the exact binomial). Paired t-test was used before and after treatment, Chi square test was used for measurement data, and Kruskal-Wallis test was used for a single sequence combination table, with p < 0.05 being statistically significant and P>0.05 being not statistically significant.
Results
Factors related to PMS
The sample includes 48 participants who completed treatment and follow-up and were included in the analysis. There were no significant differences in the two groups regarding age, BMI, course, menstrual cycles, marital status, condition. (P>0.05) (Table 2).
Table 2: Comparison of groups in terms of factors related to PMS (n=48).
Factors related to PMS |
Groups |
P |
|
EA Group(n=25) |
PA Group(n=23) |
||
Mean levels (X(—)±SD) |
|
|
|
Age/years |
0.537 |
||
Body mass index/(kg•m-2) |
20.19 ± 0.84 |
20.24 ± 0.93 |
0.963 |
Course/months |
0.352 |
||
Menstrual cycle/days |
29.83 ± 2.11 |
29.41 ± 0.92 |
0.457 |
Frequencies (n) |
|
|
|
Marital status |
|
|
|
Married |
3 |
2 |
|
Unmarried |
22 |
21 |
|
Condition |
|
|
|
Moderate |
21 |
20 |
|
Severe |
4 |
3 |
|
Scores of PMS, depression, and anxiety
After the first cycle treatment, the total score and every dimension score decreased in the two groups (P<0.05), except the symptom and sign dimension in the EA group and the influence degree dimension score in the PA group. Besides, the influence degree dimension score in the EA group decreased significantly compared with that in the PA group (P<0.05) (Figure 1A).
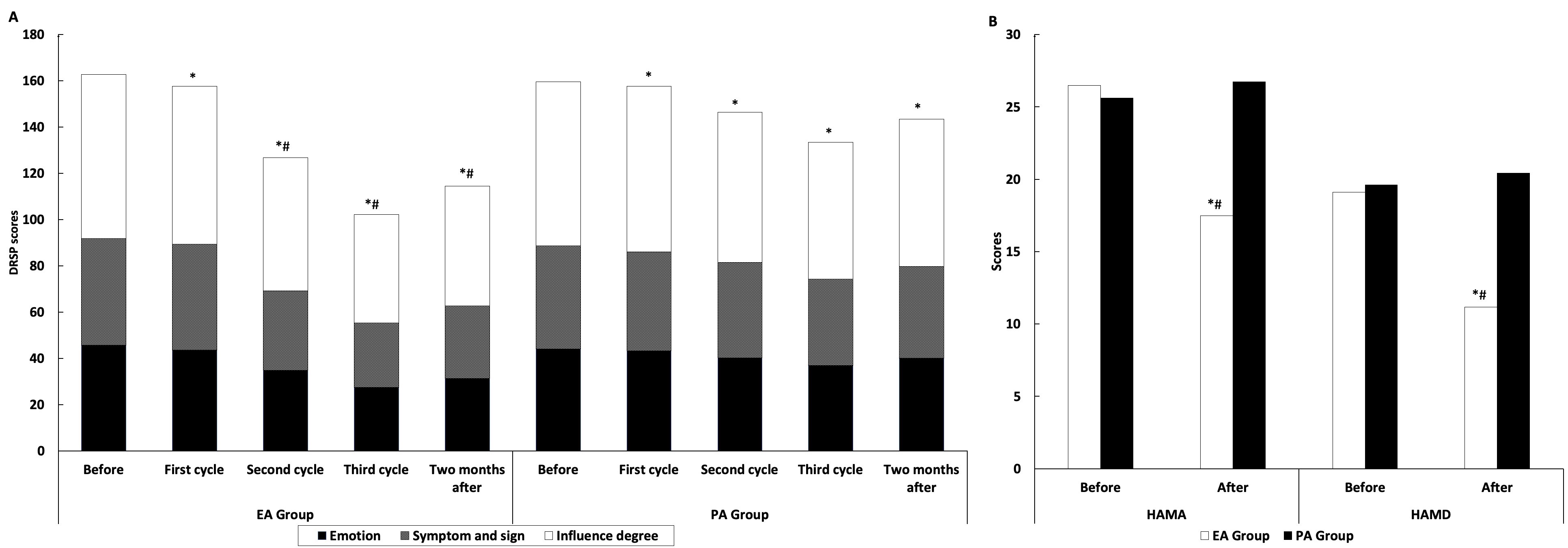
After the second, third cycle treatment, the total score and every dimension score decreased in the two groups (P<0.05). In the EA group, the total score and every dimension score decreased significantly compared with that in the PA group (P<0.05) (Figure 1A).
Two months after the whole treatment, the total score and every dimension score increased in the two groups (P<0.05). However, the total score and every dimension score in the EA group were still lower than those in the PA group (P<0.05). (Figure 1A).
Figure 1B shows that HAMA score and HAMD score decreased significantly after treatment in the EA group (P<0.05). However, in the PA group, no significant difference in HAMA score and HAMD score after treatment (P>0.05). The HAMA score and HAMD score after treatment in the EA group were lower than those in the PA group (P<0.05) (Figure 1B).
Clinical effect
The therapeutic effect is divided into cured, markedly effective, effective, and invalid. The clinical effects of the two groups are shown in Table 3. The total effective rate of the EA group was significantly higher than that of the PA group (P<0.05) (Table 3).
Table 3: Most relevant blood results at presentation.
Group |
Cured |
Markedly effective |
Effective |
Invalid |
Total effective rate |
EA Group |
3 |
3 |
16 |
3 |
88% # |
PA Group |
0 |
0 |
12 |
11 |
52.1% |
# Compared with PA Group, P<0.05.
Changes of serum hormones
In steroid hormones, there was no significant change of E2 in both groups (P>0.05). The levels of allopregnanolone and P increased significantly after treatment in the EA group (P<0.05). The levels of allopregnanolone and P were more significant than those in the PA group after treatment (P<0.05). The level of 1,25-(OH)2D decreased significantly in EA groups after treatment (P<0.05), which was more significant than that in the PA group after treatment (P<0.05) (Figure 2A).

In peptides and protein hormones, there was no significant difference in PRL and PTH between the two groups before and after treatment (P>0.05). The CRH and ACTH decreased significantly in the EA group after treatment (P<0.05). The CRH and ACTH in the EA group were more significant than those in the PA group after treatment (P<0.05) (Figure 2B).
In amino acid derivatives hormones, 5-HT, DA, NA, and Glu/ GABA decreased in the EA group after treatment (P<0.05). β - EP, GABA, and Glu increased significantly in the EA group after treatment (P<0.05). And all amino acid derivatives hormones in the EA group after treatment were definitely meaningful compared with those in the PA group (P<0.05) (Figure 2C).
In eicosanoid hormones, PGF2α and PGE2 had significant changes-PGF2α diminishing and PGE2 raising-after treatment in the EA group (P<0.05), while PGF1 α, PFE1 and TXB2 had no significant changes before and after treatment in two groups (P>0.05). PGF2α and PGE2 in the EA group after treatment were definitely meaningful compared with those in the PA group (P<0.05) (Figure 2D).
Discussion
Premenstrual syndrome is widely defined as a group of emotional, physiological, and behavioral symptoms that appear at the end of the luteal phase and disappear briefly with or after menstruation [20,21]. Some studies show that it is associated with the diets and activities [4,22]. The purpose of this study is to investigate the clinical effect and possible mechanism of electroacupuncture on PMS. By comparing the scores of DRSP, HAMA, and HAMD of electroacupuncture group and placebo group in different periods, we can judge the therapeutic effect. Through the changes of serum hormone before and after treatment, we can judge the mechanism of electron acupuncture on PMS.
Studies have shown that premenstrual syndrome is characterized by an increase in the severity of DRSP before and after menstruation, and an increase in the scores of the main DRSP dimensions, such as depression, physical symptoms, breast tenderness, appetite and anxiety [23,24]. The findings of this study demonstrated significant effects of electroacupuncture and placebo acupuncture on the reduction of PMS symptoms and among menstrual cycles (first cycle, second cycle, third cycle and two months after). The DRSP scores of EA group are significantly lower than that of PA group, implying that electroacupuncture is better than placebo acupuncture in treating PMS and indicating that psychology plays an important role in this disease. HAMA and HAMD were used to detect the degree of anxiety and depression [25,26]. The experimental results show that electroacupuncture can reduce the degree of anxiety and depression. The total effective rate of the EA group was significantly higher than that of the PA group, indicating that electroacupuncture has a definite and significant effect on PMS.
Some research results show that the negative emotions of adolescent women may be related to diet and specific food [27]. The supplement of microelements and vitamin D can lighten the symptoms of PMS patients [28], and selective 5-HT reuptake inhibitors, prostaglandin inhibitors and oral contraceptives can also alleviate the symptoms of PMS patients. Studies have confirmed that the level of vitamin D in PMS patients is low [11]. In vivo, cholesterol is converted to progesterone by cholesterol side chain lyase P450(P450scc), 3 β - hydroxysteroid dehydrogenase (3 β - HSD), and then metabolized to Allopregnanolone by 5 α - reductase and 3 β – HSD [29]. The results showed that the rise of progesterone after electroacupuncture might be caused by the above reaction chain. The increase of the two may have a negative feedback effect on the hypothalamus and pituitary, resulting in the decrease of adrenergic releasing hormones, such as ACTH, CRH, and 1,25-(OH)2D, while PRL, and E2 are not affected.
Allopregnanolone may mainly bind to the α and β subunits of GABAA receptor and then produce anti-anxiety effect [30]. PMS is related to the periodic changes of ovarian hormones in vivo, but its biological mechanism needs to be mediated by neurotransmitters (including β-ET, 5-HT, and even the adrenergic nervous system), to form neuroendocrine disorders [31,32]. The disorder of regulating hormone secretion, such as thyroxine, adrenocortical hormone, and sex hormones, can lead to emotional changes [33,34]. Through the intravenous injection of allopregnanolone in healthy women and women with PMDD, it was found that allopregnanolone can reduce the DRSP negative emotional score and the total DRSP score. It is speculated that allopregnanolone is the inducement of negative emotional symptoms in PMDD patients, and allopregnanolone can antagonize the effect of the GABAA receptor on progesterone, to improve the symptoms [35]. Some studies have shown that Shuyu capsule can inhibit the imbalance of Glu/GABA in the central nervous system of rats with PMS depression and effectively improve the corresponding symptoms of rats with PMS depression [36]. In this study, we found that β - ET, 5-HT, DA, NA, and Glu/ GABA decreased, but GABA and Glu increased after treatment, which may mitigate a series of changes of mental emotion in the premenstrual period, and then alleviate the premenstrual syndrome.
Prostaglandins are closely related to inflammation and pain [37,38]. PGF2 α and TXB2 can promote vasoconstriction, while PGE1, PGE2, and PGF1 α can relax the blood vessels [39]. Their interaction makes blood vessels in a normal state of balance. The plasma concentration of PGF2 alpha in the late luteal phase was significantly lower in patients with PMS, and the plasma concentrations of PGE in the middle follicular phase and middle luteal phase, PGE2 alpha in the middle follicular phase and TXB2 in the middle and late luteal phase were significantly higher [40]. A disturbance of PG metabolism may contribute to the etiology of PMS. The results showed that PGF2 α and PGE2 had obvious changes after electroacupuncture, which made them in a state of balance again and alleviated the premenstrual syndrome.
In this experiment, due to the limited number of participants, geographical limitations, and the study population (mostly college students), the experimental results may have limited generalizability. In the future experiment, we should further expand the scope of the experiment, to better explore the experimental efficacy. We should pay attention to the molecular mechanism of electroacupuncture in the treatment of premenstrual syndrome in the future, to provide a more reliable basis for electroacupuncture in the treatment of this disease.
Conclusion
Electroacupuncture is effective in the treatment of premenstrual syndrome, which may be alleviated by regulating P, allopregnanolone, 1,25-(OH)2D, CRH, ACTH, DA, NA, 5-HT, β–EP, GABA, Glu, Glu/GABA, PGF2 α and PGE2.
Date availability: Data to support the results of this study are available from the authors.
Conflicts of interests: The authors declare that they have no conflicts of interests.
Funding: The study was supported by the First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine Scientific Research Fund Project (JDZX2015056).
Authors' contributions: Hongying Kuang, and Jing Lin contributed equally to this work. Hongying Kuang is responsible for drafting and revising the manuscript. Jing Lin revised some manuscripts. Li Zhang, Mushan Li, and Jing Lin participated in the design and conception of the experiment. Simao Shi is responsible for regulating the progress of the experiment. Zhenxia Shao and Fan Gao are responsible for recruiting and treating patients. Kexin Ma, Jingjing Chen and Ziyu Yang participated in the data collection. Xiaoling Feng was ultimately responsible for the decision to submit the data for publication. All authors have read and approved the final manuscript.
Acknowledgements: Thanks for the support of the First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine.
Ethics approval and consent to participate: Ethical approval of the study was obtained from First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine (batch No. HZYLLKY201600802), and has been registered in the China Clinical Trial Registry (NO.ChiCTR1900024093). Researchers introduced the specific intervention and the participants’ rights during the study to the participants verbally and using an informed consent form. Before being included in the study, all participants must provide written informed consent. All participants have the right to withdraw from the study at any time, and it will not affect their subsequent treatment. Moreover, all their information will remain confidential.
Consent for publication: All authors have approved the manuscript for publication.
References
- Heidari H, Amani R, Feizi A, Askari G, Kohan S, et al. Vitamin D Supplementation for Premenstrual Syndrome-Related inflammation and antioxidant markers in students with vitamin D deficient: A randomized clinical trial. Scientific reports. 2019; 9: 14939.
- Abeje A, Berhanu Z. Premenstrual syndrome and factors associated with it among secondary and preparatory school students in Debremarkos town, North-west Ethiopia, 2016. BMC research notes. 2019; 12: 535.
- Bhuvaneswari K, Rabindran P, Bharadwaj B. Prevalence of premenstrual syndrome and its impact on quality of life among selected college students in Puducherry. The National medical journal of India. 2019; 32: 17-19.
- Hashim M, Obaideen A, Jahrami H, Radwan H, Hamad H, et al. Premenstrual Syndrome Is Associated with Dietary and Lifestyle Behaviors among University Students: A Cross-Sectional Study from Sharjah, UAE. Nutrients. 2019; 11.
- Chumpalova P, Iakimova R, Stoimenova-Popova M, Aptalidis D, Pandova M, et al. Prevalence and clinical picture of premenstrual syndrome in females from Bulgaria. Annals of general psychiatry. 2020; 19 :3.
- Crow E, Jeannot E. Premenstrual Syndrome: Symptomatic and Diagnosed Prevalence, Dualistic Treatment Approach - A CrossSectional Study in Ukraine. International journal of preventive medicine. 2017; 8: 66.
- Reuveni I, Dan R, Segman R, Evron R, Laufer S, et al. Emotional regulation difficulties and premenstrual symptoms among Israeli students. Archives of women’s mental health. 2016; 19: 1063-1070.
- Matsumoto T, Asakura H, Hayashi T. Biopsychosocial aspects of premenstrual syndrome and premenstrual dysphoric disorder. Gynecological endocrinology: The official journal of the International Society of Gynecological Endocrinology. 2013; 29: 67-73.
- Zhou W, Benharash P. Effects and mechanisms of acupuncture based on the principle of meridians. Journal of acupuncture and meridian studies. 2014; 7: 190-193.
- Chen H, Chen M, Hsieh C, Wu S, Hsu H, et al. TRPV1 is a Responding Channel for Acupuncture Manipulation in Mice Peripheral and Central Nerve System. Cellular physiology and biochemistry: International journal of experimental cellular physiology, biochemistry, and pharmacology. 2018; 49: 1813-1824.
- Fatemi M, Allahdadian M, Bahadorani M. Comparison of serum level of some trace elements and vitamin D between patients with premenstrual syndrome and normal controls: A cross-sectional study. International journal of reproductive biomedicine. 2019; 17: 647-652.
- Armour M, Ee C, Hao J, Wilson T, Yao S. Acupuncture and acupressure for premenstrual syndrome. The Cochrane database of systematic reviews. 2018; 8: CD005290.
- Kim S, Park H, Lee H, Lee H. Acupuncture for premenstrual syndrome: a systematic review and meta-analysis of randomised controlled trials. BJOG: An international journal of obstetrics and gynaecology. 2011; 118: 899-915.
- Cho S, Kim J. Efficacy of acupuncture in management of premenstrual syndrome: a systematic review. Complementary therapies in medicine. 2010; 18: 104-111.
- Zhang J, Cao L, Wang Y, Jin Y, Xiao X, et al. Acupuncture for Premenstrual Syndrome at Different Intervention Time: A Systemic Review and Meta-Analysis. Evidence-based complementary and alternative medicine: eCAM. 2019; 2019: 6246285.
- Itsekson A, Yonit B, Ze’ev I, Matitiyahu Z, Shmuel K. Safety and value of skin test to sex hormones and sex hormone sensitivity desensitization in women with premenstrual syndrome. The World Allergy Organization journal. 2019; 12: 100041.
- Wei S, Geng X, Li Z, Xu K, Hu M, et al. A forced swim-based rat model of premenstrual depression: effects of hormonal changes and drug intervention. Aging. 2020; 12: 24357-24370.
- Shang L, Pin L, Zhu S, Zhong X, Zhang Y, et al. Plantamajoside attenuates isoproterenol-induced cardiac hypertrophy associated with the HDAC2 and AKT/ GSK-3β signaling pathway. Chemicobiological interactions. 2019; 307: 21-28.
- Choi S, Hamidovic A. Association Between Smoking and Premenstrual Syndrome: A Meta-Analysis. Frontiers in psychiatry. 2020; 11: 575526.
- Ismaili E, Walsh S, O’Brien P, Bäckström T, Brown C, Dennerstein L, et al. Fourth consensus of the International Society for Premenstrual Disorders (ISPMD): Auditable standards for diagnosis and management of premenstrual disorder. Archives of women’s mental health. 2016; 19: 953-958.
- Appleton S. Premenstrual Syndrome: Evidence-based Evaluation and Treatment. Clinical obstetrics and gynecology. 2018; 61: 52-61.
- Maged A, Abbassy A, Sakr H, Elsawah H, Wagih H, et al. Effect of swimming exercise on premenstrual syndrome. Archives of gynecology and obstetrics. 2018; 297: 951-959.
- Roomruangwong C, Carvalho A, Comhaire F, Maes M. Lowered Plasma Steady-State Levels of Progesterone Combined With Declining Progesterone Levels During the Luteal Phase Predict Peri-Menstrual Syndrome and Its Major Subdomains. Frontiers in psychology. 2019; 10: 2446.
- Henz A, Ferreira CF, Oderich CL, Gallon CW, Castro JRS, et al. Premenstrual Syndrome Diagnosis: A Comparative Study between the Daily Record of Severity of Problems (DRSP) and the Premenstrual Symptoms Screening Tool (PSST). (1806-9339 (Electronic)).
- Kasper S, Müller W, Volz H, Möller H, Koch E, et al. Silexan in anxiety disorders: Clinical data and pharmacological background. The world journal of biological psychiatry: The official journal of the World Federation of Societies of Biological Psychiatry. 2018; 19: 412-420.
- Carney C, Edinger J, Kuchibhatla M, Lachowski A, Bogouslavsky O, et al. Cognitive Behavioral Insomnia Therapy for Those With Insomnia and Depression: A Randomized Controlled Clinical Trial. Sleep. 2017; 40.
- Bu L, Lai Y, Deng Y, Xiong C, Li F, et al. Negative Mood Is Associated with Diet and Dietary Antioxidants in University Students During the Menstrual Cycle: A Cross-Sectional Study from Guangzhou, China. Antioxidants (Basel, Switzerland). 2019; 9.
- Retallick-Brown H, Blampied N, Rucklidge J. A Pilot Randomized Treatment-Controlled Trial Comparing Vitamin B6 with BroadSpectrum Micronutrients for Premenstrual Syndrome. Journal of alternative and complementary medicine (New York, NY). 2020; 26: 88-97.
- Schumacher M, Mattern C, Ghoumari A, Oudinet J, Liere P, et al. Revisiting the roles of progesterone and allopregnanolone in the nervous system: Resurgence of the progesterone receptors. Progress in neurobiology. 2014; 113: 6-39.
- Follesa P, Porcu P, Sogliano C, Cinus M, Biggio F, et al. Changes in GABAA receptor gamma 2 subunit gene expression induced by long-term administration of oral contraceptives in rats. Neuropharmacology. 2002; 42: 325-336.
- Hantsoo L, Epperson C. Premenstrual Dysphoric Disorder: Epidemiology and Treatment. Current psychiatry reports. 2015; 17: 87.
- Marjoribanks J, Brown J, O’Brien P, Wyatt K. Selective serotonin reuptake inhibitors for premenstrual syndrome. The Cochrane database of systematic reviews. 2013: CD001396.
- Maayan R, Fisch B, Galdor M, Kaplan B, Shinnar N, et al. Influence of 17beta-estradiol on the synthesis of reduced neurosteroids in the brain (in vivo) and in glioma cells (in vitro): possible relevance to mental disorders in women. Brain research. 2004; 1020: 167-172.
- Mize A, Alper R. Acute and long-term effects of 17beta-estradiol on G(i/o) coupled neurotransmitter receptor function in the female rat brain as assessed by agonist-stimulated [35S]GTPgammaS binding. Brain research. 2000; 859: 326-333.
- Bixo M, Johansson M, Timby E, Michalski L, Bäckström T. Effects of GABA active steroids in the female brain with a focus on the premenstrual dysphoric disorder. Journal of neuroendocrinology. 2018; 30.
- Gao X, Sun P, Qiao M, Wei S, Xue L, Zhang H. Shu-Yu capsule, a Traditional Chinese Medicine formulation, attenuates premenstrual syndrome depression induced by chronic stress constraint. Molecular medicine reports. 2014; 10: 2942-2948.
- Robinson D, Dayer J, Krane S. Prostaglandins and their regulation in rheumatoid inflammation. Annals of the New York Academy of Sciences. 1979; 332: 279-294.
- Haidari F, Homayouni F, Helli B, Haghighizadeh M, Farahmandpour F. Effect of chlorella supplementation on systematic symptoms and serum levels of prostaglandins, inflammatory and oxidative markers in women with primary dysmenorrhea. European journal of obstetrics, gynecology, and reproductive biology. 2018; 229: 185-189.
- Rehal S, von der Weid P. Experimental ileitis alters prostaglandin biosynthesis in mesenteric lymphatic and blood vessels. Prostaglandins & other lipid mediators. 2015: 37-48.
- Koshikawa N, Tatsunuma T, Furuya K, Seki K. Prostaglandins and premenstrual syndrome. Prostaglandins, leukotrienes, and essential fatty acids. 1992; 45: 33-36.