
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A giant juvenile fibroadenoma in a 12-year-old girl: Case report and brief literature review
Ekhlas S Bardisi1,4*; Ann Smeets1; Giuseppe Floris2; Chantal Van Ongeval3; Machteld Keupers3; Ines Nevelsteen1
1 Department of Surgical Oncology, UZ-Leuven, Leuven, Belgium.
2 Department of Pathology, UZ-Leuven, Leuven, Belgium.
3 Department of Radiology, UZ-Leuven, Leuven, Belgium
4 Department of Surgery, KAU, Jeddah, KSA.
*Corresponding Author: Ekhlas S Bardisi
Department of Surgical Oncology, UZ-Leuven, Leuven,
Belgium.
Department of surgery, KAU, Jeddah, KSA.
Email: e--s--b@hotmail.com
Received : Jun 15, 2021
Accepted : Jul 15, 2021
Published : Jul 20, 2021
Archived : www.jcimcr.org
Copyright : © Bardisi ES (2021).
Abstract
Juvenile fibroadenoma is the most common breast mass in adolescents accounting for 0.5–4% of all cases of fibroadenomas. Giant fibroadenomas are rare variants and represent only 0.5% of all fibroadenomas, usually occurring in girls between the ages of 10 and 18.
They are characterized by massive and rapid enlargement of a rubbery, mobile, and non-tender mass and defined as being larger than 5 cm or weighing more than 500 g. The aetiology is not well understood and is believed to be an increased sensitivity to normal oestrogen level.
We present a 12-year-old Asian girl treated at the age of 8 for idiopathic precocious puberty, without known family history of breast masses or cancers, who developed spontaneous giant fibro-adenoma measuring 15cm X 17 cm. The patient was further evaluated via ultrasonography showing a sole large lesion of 15 X 17 cm in the left breast. Surgical excision with conservation of the developing breast parenchyma and nipple-areolar complex under general anaesthesia was performed. Histopathological findings after the surgical excision were suggestive of juvenile fibroadenoma. The patient has a normal breast development throughout 4 years follow-up.
The rapid growth of a breast mass in such young patients can be of great concern causing a considerable impact on these patients’ psychological and emotional condition. One of the most important concerns is the impact on potential future mammary gland development. Therefore, it is crucial to promptly rule out malignant processes or phyllodes tumors and educate young patients and their families on treatment options that fit their concerns. In addition, the final cosmetic result is essential after the surgical excision; although the primary cause of asymmetrical breast enlargement is a benign mass, early surgical excision is efficient concerning the best possible cosmetic outcome.
Keywords: Breast mass; juvenile fibroadenoma; giant fibroadenoma.
Citation: Bardisi ES, Smeets A, Floris G, Ongeval CV, Keupers M. A Giant juvenile fibroadenoma in a 12-year-old girl: Case report and brief literature review. J Clin Images Med Case Rep. 2021; 2(4): 1235.
Introduction
Fibroadenomas are the most common type of breast tumor diagnosed in young women. Juvenile fibroadenoma is a rare disorder accounting for 0.5–4% of all cases of fibroadenomas, they occur most frequently in adolescent girls or young women [1]. It is described as a well-circumscribed, firm, and rubber-like breast mass presenting as a large mass. They may be characterized as giant fibroadenoma when they are larger than 5 cm or weigh more than 500 g [2,3]. The peak age has been reported between the ages of 17 and 20, with less than 5% of these in patients less than 18-years-old [4]. They have been more frequently reported in black patients [1]. These benign tumors incline rapid growth resulting in embarrassment and anxiety; this is known to result in unpleasant interactions with their peers and significantly impact these patients’ psychological and emotional condition [20]. Exceedingly large fibroadenomas may additionally cause skin ulceration and vascular congestion [2,5,6].
Histologically, juvenile fibroadenomas are characterized by a prevalent pericanalicular growth pattern with a moderate increase of stromal cellularity without atypia and associated with gynaecomastoid type of epithelial hyperplasia [1].
The differential diagnosis for a rapidly growing breast mass in an adolescent includes giant fibroadenoma, virginal hypertrophy, inflammatory processes such as a breast abscess and phyllodes tumor [3,21]. Breast cancer in children is rare; however, it has been reported and is also part of the differential diagnosis [2,8]. Breast cancer concomitant with juvenile fibroadenoma has also been observed [9,10]. A family history of breast cancer has been linked in 26–58% of patients with juvenile fibroadenoma [10,12]. Some patients have developed breast cancer eight to nine years after diagnosing and treating juvenile fibroadenoma [12]. However, this risk of malignant degeneration of a fibroadenoma is less than 0.3% [6].
Surgical excision is usually needed if the mass continues to grow, causes considerable pain, distortion of the breast parenchyma or cosmetic concerns; complete local excision with sparing of breast tissue is often the treatment of choice [21-23]. Numerous surgical techniques, such as conventional local excision, reduction mammoplasty, or inframammary excision, have been reported to excise the giant fibroadenoma [21-22].
Case report
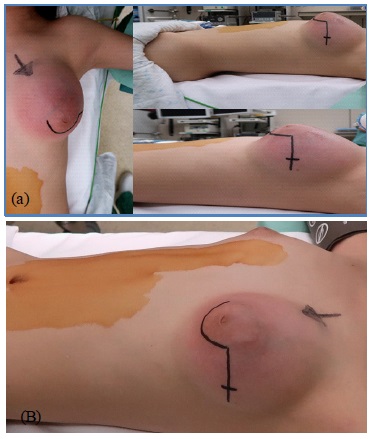
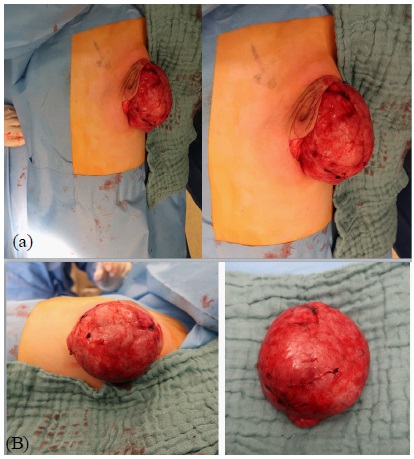
We report a 12-year-old Asian girl treated at the age of 8 with 12 weeks of Decapeptyl for idiopathic precocious puberty. She presented at the age of 12 with a one-month history of rapidly growing left breast. Over one month, the left breast had continued growing, becoming hard and warm. She was taken to the family physician, who treated her for a suspected infection with antibiotics and referred her to the paediatrician, who in turn stopped the antibiotics and consulted us for further advice. The patient did not have any family history of breast cancer, breast masses, or other cancers. On physical exam, the left breast was considerably larger than the right with signs of congestion. Palpation showed a palpable, mobile round mass that was tender to touch, measuring approximately 15 cm X 17 cm (Figure 1), not attached to the skin or the thorax, with no palpable lymphadenopathies. Ultrasound revealed on the left breast an enormous, homogenous, and hypo-echogenic mass measuring 15 cm with subtle vascularity and no calcifications (Figure 2). On the contralateral breast, there was also a small, sharply delineated hypo-echogenic nodular lesion (5 mm) on 3-4 o’clock suggested for fibrocystic changes or fibroadenoma. Core biopsy of the left mass was performed, and the histopathology of the specimen suggested a differential diagnosis between cellular and juvenile fibro-adenoma. Surgical excision of the left mass via a lateral radial incision on 3 o’clock with an extended incision peri- areolar from 3 to 9 o’clock was performed (Figure 3a,b), (Figure 4a,b). Histopathological findings of the resected specimen were consistent with the diagnosis of a giant juvenile fibro-adenoma.


The patient was well on a one-month follow-up with excellent wound healing and no dominant masses noted on both breasts (Figure 5). However, ultrasound on six-month follow-up showed a volume-increase of the known mobile mass in the right breast, located supra-areolar, sharp, homogenous, and hypo-echogenic measuring 2,7 X 1,3 X 2,4 cm compared to the previous measurements six months ago (1,1 X 0,9 X 0,5 cm). Because of the doubling in size of the fibroadenoma in a 6-month period, surgical excision via peri-areolar incision was performed after a discussion with the patient and the family. Histopathological examination confirmed the diagnosis of fibroadenoma with a diameter of 2.6 cm.

After the surgeries, follow-up up to 4 years demonstrated breasts that were almost equal in size with cosmetic results to the patient’s satisfaction.
Discussion
The presence of breast lesions in children and adolescent females is rare, including benign and malignant tumors such as fibroadenomas, phyllodes tumors, and breast carcinoma. Juvenile fibroadenomas, composed of epithelium and/ or stroma of the terminal lobule of the breast, represent only 0.5% of all fibroadenomas [15,20]. Although the aetiology of the lesion is still not known, hormonal factors have been implicated. Excessive oestrogen stimulation, increased oestrogen receptor sensitivity, or decreased oestrogen antagonist sensitivity are thought to be major contributing factors to the disease [13]. In our case the patient had a history of idiopathic precocious puberty and already treated at the age of 8, no previous studies were available to show the link between idiopathic precocious puberty and the development of benign or malignant breast masses. A case of giant fibroadenoma in a 12-year-old female resulting from trauma has been previously reported [14]. Although they are benign neoplasms, giant fibroadenomas can compress surrounding tissue and alter lobule structure due to their increased size and vascularity [15,16].
Superficial manifestations of giant fibroadenomas can be similar to malignant processes, such as ulceration, skin dimpling, and nipple inversion [15]. Because of these complications and potential risks, early detection, diagnosis, and treatment of giant juvenile fibroadenomas is important. Ultrasonography is the most common primarily diagnostic method for breast masses in children and more specifically for fibroadenomas [17]. Ultrasound is preferred over other imaging modalities such as mammography, computed tomography, and magnetic resonance imaging due to concerns of excessive radiation exposure to young patients. Furthermore, ultrasound studies identify masses in fibroglandular breasts, such as those of adolescent females, better than in fatty breasts [18,19].
Large masses (3 cm or larger) are more likely to be diagnosed as phyllodes tumors, although they are rare in young patients, about 20 cases have been reported in children [24].
Fibroadenomas and phyllodes tumors share many common features. Clinically and histologically, so both can be grouped as “Fibroepithelial lesions”. Preoperative diagnosis carrying a diagnostic difficulty, as fine needle aspiration cytology and core needle biopsy may not be able to distinguish a phyllodes tumor from a fibroadenoma [25].
Additionally, due to core needle biopsy's psychological and emotional effects in young patients, it is not uncommon to proceed with excisional biopsy as a diagnostic and therapeutic method. There is little evidence to support observation as a valid medical option since diagnosis might be difficult to ascertain without histological confirmation. Yet if this is the choice of the patient and family, a tissue diagnosis via a core needle biopsy has to be obtained to exclude malignancy [20] as performed in our case.
Because of the patient's young age and potential for further breast development, the goal is not only a complete excision of the tumor but also a special surgical consideration is placed on the preservation of the areola and nipple, maintaining lactation ability, preservation of breast parenchyma and achievement of symmetrical breasts with good cosmetic results [16,21].
It was thought that reconstructive methods are usually needed after removing large breast lesions to attain symmetrical breasts bilaterally. Nevertheless, a systematic review showed that it is uncommon to proceed with reconstructive surgery in giant fibroadenomas [21]. A simple mastectomy might be needed if the breast is too small and is almost totally occupied by the lesion.
Conclusion
Giant juvenile fibroadenoma should be considered a differential diagnosis in paediatric or adolescent patients with rapidly growing breast mass, confirmed by ultrasound and histological analysis. The rapid growth of a breast mass can be of great concern to young patients whose breasts are in the early formative stages. Therefore, ruling out malignant processes or phyllodes tumors and educating young patients and their families on treatment options that fit their unique concerns and circumstances is crucial.
Complete excision of the mass with conservation of nippleareola complex is indicated to make a definitive diagnosis and relieve the normal breast tissue compression.
When planning surgical excision, the final cosmetic result is essential, and we believe that an early surgical excision is efficient concerning the best possible cosmetic outcome.
Ethical approval: Ethics Committee informed that approval was not required for this study.
Consent: Written parental or guardian consent is confirmed for the publication of this case report and accompanying images as the patient is only 12 years old. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
References
- Jayasinghe Y, Simmons PS, Fibroadenomas in adolescence, Curr Opin Obstet Gynecol. 2009; 21: 402–406.
- Raganoonan C, Fairbain JK, Williams S, Hughes LE, Giant breast tumours of adolescence, Aust N Z J Surg. 1987; 57: 243–247.
- Greydanus DE, Matytsina L, Gains M, Breast disorders in children and adolescents, Prim Care. 2006; 33: 455–502.
- Umekita Y, Yoshida H, Immunohistochemical study of hormone receptor and hormone-regulated protein expression in phyllodes tumour: comparison with fibroadenoma, Virchows Arch. 1998; 433: 311–314.
- Arowolo OA, Akinkuolie AA, Adisa AO, Obonna GC, Olasode BJ, Giant fibroadenoma presenting like fungating breast cancer in a Nigerian teenager, Af Health Sci. 2013; 13: 162–165.
- Kaur N, Saini S, Somasekhar S, Gupta A, Bilateral florid juvenile fibroadenomas of the breast in an adolescent: a rare indication for subcutaneous mastectomy, J Pediatr Adolesc Gynecol. 2015; 28: e135–e137.
- Kier LC, Hickey RC, Keettel WC, Womack NA, Endocrine relationships in benign lesions of the breast, Ann Surg. 135: 782–787.
- Davis C, Patel V, Surgical problems in the management of giant fibroadenoma of the breast, Am J Obstet Gynecol. 1985; 152: 1010–1015.
- Rosen PP, Lyngholm B, Kinne DW, Beattie EJ, Juvenile papillomatosis of the breast and family history of breast carcinoma, Cancer. 1982; 49: 2591–2595.
- Bazzocchi F, Santini D, Martinelli G, Piccaluga A, Taffurelli M, et al. Juvenile papillomatosis (epitheliosis) of the breast: A clinical and pathologic study of 13 cases, Am J Clin Pathol. 1986; 86: 745–748.
- Vidal M, Peg V, Galv´an P et al. Gene expression-based classifications of fibroadenomas and phyllodes tumours of the breast,, Mol Oncol. 2015; 9: 1081–1090.
- Rosen PP, Kimmel M, Juvenile papillomatosis of the breast: A follow-up study of 41 patients having biopsies before 1979, Am J Clin Pathol. 1990; 93: 599–603.
- Greydanus DE, Parks DS, Farrell EG, Breast disorders in children and adolescents, Pediatr Clin North Am. 1989; 36: 601–638.
- Izadpanah A, Karunanayake M, Izadpanah A, Sinno H, Gilardino M, An atypical growth of a giant fibroadenoma after trauma, J Pediatr Adolesc Gynecol. 2012; 25: e115–e117.
- Park CA, David LR, Argenta LC, Breast Asymmetry: Presentation of a Giant Fibroadenoma, Breast J. 2006; 12: 451–461.
- Matz D, Kerivan L, Reintgen M et al. Breast preservation in women with giant juvenile fibroadenoma, Clin Breast Cancer. 2013; 13: 219–222.
- Chung EM, Cube R, Hall GJ et al. Breast masses in children and adolescents: Radiologic-pathologic correlation, RadioGraphics. 2009; 29: 907–931.
- Greenberg R, Skornick Y, Kaplan O, Management of breast fibroadenoma, J Gen Intern Med. 1998; 13: 640–645.
- Boothroyd A, Carty H, Breast masses in childhood and adolescence, Pediatr Radiol. 1994; 24: 81–84.
- Sosin M, Pulcrano M, Feldman ED et al. Giant juvenile fibroadenoma: A systemic review with diagnostic and treatment recommendations, Gland Surg. 2015; 4: 312–321.
- Chang DS, McGrath MH, Management of benign tumors of the adolescent breast, Plast Reconstr Surg. 2007; 120: 13e–19e.
- Naraynsingh V, Maharaj D, Rampaul R. “Swiss-roll” operation for giant fibroadenomas. Breast J. 2002; 8: 45e46.
- Lee M, Soltanian HT. Breast fibroadenomas in adolescents: current perspectives. Adolesc Health Med Ther. 2015; 6: 159-163.
- B. Erginel, B. Celet Ozden, S. Yesil Onder, S. Yuksel, F. Gun Soysal, et al. Management of a benign phyllodes tumor in a 13-year-old girl with trans-position of the nipple areola complex and breast reconstruction. Acta Chir Belg. 2015; 115: 256-259.
- MD Anderson Cancer Center. Clinical practice algorithms of phyllodes tumor. Available at: http://www.mdanderson.org/education-and-research/resources-for-professionals/clinical-toolsand-resources/practice-algorithms/ca-treatment-phyllodeswebalgorithm.pdf. Google Scholar.