
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Mycobacterium bovis meningitis together with systemic brucellosis
Tuğçe Başarı*; Elif Tükenmez Tigen
Department of Infection Disease and Clinical Microbiology, Faculty of Medicine, Marmara University, İstanbul, Turkey.
*Corresponding Author: Tuğçe Başar
Department of Infection Disease and Clinical
Microbiology, Faculty of Medicine, Marmara
University, İstanbul, Turkey.
Email: tbasari54@gmail.com
Received : Jun 20, 2021
Accepted : Jul 26, 2021
Published : Jul 30, 2021
Archived : www.jcimcr.org
Copyright : © Başarı T (2021).
Abstract
M. bovis and Brucella spp. are zoonotic bacteria that can infect humans. These pathogens are usually seen in people who are primarily engaged in animal husbandry and consume infected animal products separately. Although our country is endemic for tuberculosis and brucellosis, it is rare to detect these two pathogens concomitantly. Thus, the case is instructive and unusual in terms of the coexistence of two concomitant zoonotic pathogens.
Keywords: M. bovis; meningitis; brucellosis; concomitant.
Abbreviations: PRZ: Pyrazinamide; DM: diabetes mellitus; RA: rheumatoid arthritis; MRI: magnetic resonance imaging; CSF: cerebrospinal fluid; EVD: Extraventricular drainage; INH: isoniazid; RIF: Rifampicin.
Citation: Başarı T, Tigen ET. Mycobacterium bovis meningitis together with systemic brucellosis. J Clin Images Med Case Rep. 2021; 2(4): 1245.
Introduction/background
M. bovis is a kind of zoonotic pathogen that transmits by inhalation and consuming infected food. Although M.tuberculosis is clinically similar to M. bovis, it is possible to distinguish it by laboratory typing and Pyrazinamide (PRZ) resistance. In our case report, a 66-year-old female was diagnosed with M. bovis meningitis and brucellosis. The case is instructive and remarkable because M. bovis is also brought to mind in tuberculosis patients mainly engaged in animal husbandry and its progress with brucellosis.
Case report
A sixty-six-year-old female patient applied to the outpatient clinic with a fever. She had a history of Diabetes Mellitus (DM) and Rheumatoid Arthritis (RA). Laboratory tests resulted as WBC: 3100/mm3 , PLT: 40000/mm3 , sedimentation: 79 mm/ hr. Echocardiography was normal, anti-HIV, VDRL, and brucella rose bengal tests were negative, and the PPD test was 15 mm positive. Thoracic and abdominal tomography revealed hilar lymphadenopathy, multiple micronodules in the lung parenchyma, and multiple hypodense lesions in the spleen. A bone marrow biopsy was performed to investigate the cause of bicytopenia compatible with the hypercellular bone marrow containing focal granulomatous inflammation, and the Ehrlich Zehl Neelsen staining was negative. Endobronchial ultrasonography was performed to exclude sarcoidosis. Pulmonary involvement of RA pathology revealed anthracosis pigment accumulation and necrotic material in the lung.
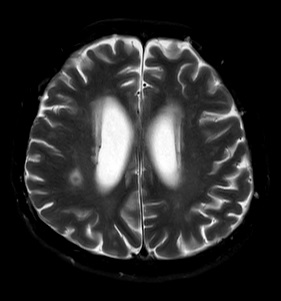
The patient developed severe headaches and confusion during the follow-up. Cranial Magnetic Resonance İmaging (MRI) showed hydrocephalus, peripheral contrast-enhancing, circumferential edema accompanying annular lesions in both cerebral hemispheres, leptomeningeal enhancement, and contrast increase in the lateral ventricle wall (Figure 1). At first, intracranial tuberculosis and neurosarcoidosis were considered. The angiotensin-converting-enzyme was normal. Mycobacterium PCR was found positive in the Cerebrospinal Fluid (CSF) examination. In the light of clinical, laboratory, and pathological data, it was thought that the possible diagnosis might be central nervous system tuberculosis. Extraventricular Drainage (EVD) was inserted because of the hydrocephaly, and then empirical tuberculosis, steroid therapy were initiated. Growth in mycobacteria culture was reported on the 19th day of the treatment. The M.bovis strain was isolated on the 38th day, resulting in Isoniazid (INH), Rifampicin (RIF), Ethambutol, streptomycin susceptible, and PZA resistance in the susceptibility test.
In the follow-up, the EVD of the patient whose hydrocephalus regressed was removed. M. bovis treatment was regulated and discharged. After 2 months, fever and confusion started again. Repeated cranial imaging showed regression in hydrocephalus, tuberculoma, and leptomeningeal involvement. It was learned that she consumed unpasteurized milk products. Brucella Wright agglutination test was positive at 1/320 titer. At first, neurobrucellosis was considered due to the fever and unconsciousness under the treatment of M.bovis meningitis. In the CSF sample; Total neutrophil count (TNC): 43, BFM: 41 (96.4%), glucose: 33 g/dL, concurrent blood glucose: 146 mg/ dL, protein: 196 mg/dL. Few leukocytes and no microorganisms were seen in direct examination. M.tuberculosis PCR, Wright agglutination test, brucella IgG, brucella IgM, 2-Mercaptoethanol (ME) tests were negative in the CSF. Serum 2-ME test was sent to the central laboratory, and it was negative. The systemic brucellosis but no neurobrucellosis was considered. Doxycycline and moxifloxacin were added to INH and RIF treatment, considering that resistance might have developed due to brucella infection under RIF treatment. Intracranial tuberculosis treatment was planned for at least 12 months and brucellosis treatment for at least six weeks. His general condition and orientation tended to improve under treatment and he was discharged with recommendations for continuing the outpatient treatment and outpatient clinic control.
Discussion
M. bovis is a zoonotic bacterium within the M.tuberculosis complex group, and its primary reservoir is bovine animals. The transmission occurs consumption of meat and dairy products of the infected animal and droplet inhalation. Although rare, transmission from human to human and from person to animal has been reported. In Taiwan, M.bovis infection due to consumption of fresh deer blood and milk has been reported [1]. Since the disease usually occurs with the consumption of infected products, more extrapulmonary involvement (lymph node and gastrointestinal system) is observed. In the United States, 1-2% of all tuberculosis cases is associated with M. bovis. In San Diego, between 2010-2015, it was observed that this rate was 10% and 54% for adults and children subsequently. It has been shown that these children are usually Hispanic or Mexican-born [2].
In an epidemiological study conducted in the United States, it was observed that Hispanic origin, living in Mexico for >2 months, HIV co-infection, and extrapulmonary involvement were associated with M. bovis rather than M. tuberculosis. In this study, the PZA monoresistance’s Positive Predictive Value (PPV) were detected as 92% and 82% in M. bovis [3].
In Turkey, M. tuberculosis sub-species analysis was performed on 220 samples between the years 2004-2014. M. bovis was detected in only three of these. The most striking issue in this study is that three isolates were seen in 2011-2014, attributed to bovine import [4]. In a study conducted in Egypt in 2002, M. bovis was isolated in 1/67 of the M. tuberculosis meningitis cases.
M. bovis infections cannot be distinguished clinically and radiologically from M. tuberculosis easily. Lung cavitation and sputum EZN positivity, contagiousness, and central nervous system involvement rates are similar with M. tuberculosis, but mortality is higher in M. bovis infections. Therefore, decontamination and culture procedures used for M.tuberculosis are used in the diagnosis of M. bovis too.
Brucellosis is a zoonotic disease transmitted mainly through consuming contaminated milk and dairy products. The most common type of subspecies in humans is B. melitensis. The initial symptoms are not specific. Patients present to the hospital with fever, weakness, night sweats, weight loss, and arthralgia at the first stage. Hepatosplenomegaly, lymphadenopathy and cytopenia occur as brucellosis involves the reticuloendothelial system. Biopsies from reticuloendothelial organs showed noncaseified granuloma. Although the gold standard in diagnosing the disease is the production of microorganisms in culture, the sensitivity of serological tests is very high. The most commonly used test is the Wright agglutination test, and titers of 1/160 and above in a single test or a four-fold increase between two tests are significant in terms of diagnosis. The agent to be chosen to treat the disease and the duration of treatment are determined according to the location of the involvement. Treatment is usually given for six weeks with a combination of doxycycline and RIF or an aminoglycoside.
Tuberculosis and brucellosis are endemic diseases in our country. Distinguishing these two infections is essential because their treatments are different, but their laboratory and histological parameters are similar. Misdiagnosis and mistreatment lead to the progression of the disease and the development of antimicrobial resistance. However, brucellosis and tuberculosis co-infection can be seen rarely in patients with animal exposure, but an actual co-infection rate has not been specified. According to the literature review, two cases of spondylodiscitis co-infected with brucellosis and tuberculosis [5,6], one osteomyelitis [7], two meningitis [8,9], one lymphadenitis and neck abscess [10], and one pericarditis have been reported. Therefore, Dasari et al. suggested that tuberculosis should be investigated in patients with suspected or proven brucellosis [11].
Conclusion
Since M. bovis infections cannot be easily distinguished from M. tuberculosis as clinically and radiologically, M. bovis should be considered in the case with livestock history, extrapulmonary involvement, non-response to M. tuberculosis treatment, in pediatric case, or PZA resistance in a patient diagnosed with tuberculosis. Typing for M. bovis should be performed in all M. tuberculosis strains showing early growth or single PZA resistance in liquid media. Cases with fluctuations in the clinic despite appropriate anti-tuberculosis treatment should be investigated for a second zoonotic pathogen if there is contact with livestock animals. Our case is instructive and extraordinary in terms of the rare co-infection of M.bovis and brucellosis..
Ethical approval: Our institution does not require ethical approval for case reports.
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
References
- Wei CY, Hsu YH, Chou WJ, Lee CP, Tsao WL. Molecular and histopathologic evidence for systemic infection by Mycobacterium bovis in a patient with tuberculous enteritis, peritonitis, and meningitis: A case report. The Kaohsiung Journal of Medical Sciences. 2004; 20: 302-307.
- Rodwell TC, Moore M, Moser KS, Brodine SK, Strathdee SA. Tuberculosis from Mycobacterium bovis in binational communities, United States. Emerging Infection Diseases. 2008;14: 909- 916.
- Gallivan M, Shah N, Flood J. Epidemiology of human Mycobacterium bovis disease, California, USA, 2003-2011. Emerging Infection Diseases. 2015; 21: 435-443.
- Öztürk CE, Şahin İ, Öksüz Ş, et al. [Investigation of Mycobacterium bovis subsp. bovis among the strains of Mycobacterium tuberculosis complex isolated in Düzce Province, Turkey]. Mikrobiyoloji Bulteni. 2016; 50: 392-400.
- Turunc T, Demiroglu YZ, Uncu H, Colakoglu S, Arslan H. A comparative analysis of tuberculous, brucellar and pyogenic spontaneous spondylodiscitis patients. The Journal of infection. 55; 158–163.
- Papachristodoulou E, Kakoullis L, Louppides S, Panos G. Granulomatous infective spondylitis in a patient presenting with progressive difficulty in walking: the differential between tuberculosis and brucellosis. BMJ case reports. 2019 24; 12: e232540.
- Quirino A, Torti C, Strazzulla A, Nisticò S, Galati L, et al. Professional Acquisition of M. bovis in Calabria Region (Southern Italy): A Challenging Case of Osteomyelitis in a Migrant Patient from Bulgaria. Case reports in infectious diseases vol. 2015: 794715.
- Ozkok A, Elcioglu OC, Akpinar TS, Kara E, Tufan F, Cagatay A. Tuberculous meningitis together with systemic brucellosis. Journal of infection and chemotherapy : official journal of the Japan Society of Chemotherapy. 18: 403–405.
- Karsen H, Karahocagil MK, Irmak H, Demiröz AP. Menenjitli bir olguda Brucella ve tüberküloz koenfeksiyonu. A meningitis case of Brucella and tuberculosis co-infection]. Mikrobiyoloji bulteni. 42; 689–694.
- Gude D, Bansal DP, Kotari HR. An unusual case of double jeopardy. Annual of Tropical Medicine and Public Health. 2013; 6: 125-127.
- Dasari S, Naha K, Prabhu M. Brucellosis and tuberculosis: clinical overlap and pitfall. Asian Pacific journal of tropical medicine. 6; 823–825.