
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Intestinal gangrene as the presenting manifestation of acute promyelocytic leukemia
Sneha Tandon1*; Sanjeev Yadav2; Ruchi Gupta2 ; Soniya Nityanand2
1 Division of Paediatric Oncology, Department of Paediatrics, University Hospital Southampton, Southampton, UK.
2 Department of Clinical Haematology, Sanjay Gandhi Postgraduate Institute, Lucknow, India.
*Corresponding Author: Sneha Tandon
Consultant Paediatric Haematologist, University
Hospital Southampton, UK.
Email: sneha25tandon@gmail.com
Received : Jun 16, 2021
Accepted : Jul 26, 2021
Published : Jul 30, 2021
Archived : www.jcimcr.org
Copyright : © Tandon S (2021).
Abstract
Bleeding, often catastrophic, is common, however, thrombosis is rare in Acute Promyelocytic Leukemia (APL). Intestinal gangrene is an unusual presentation of thrombosis of mesenteric vasculature. We hereby, for the first time report this unusual presentation of intestinal gangrene secondary to leukaemic infiltration in APL and highlight the importance of prompt therapeutic intervention given its catastrophic nature.
Keywords: Bowel; intestine; gangrene; acute promyelocytic leukaemia.
Citation: Tandon S, Yadav S, Gupta R, Nityanand S. Intestinal gangrene as the presenting manifestation of acute promyelocytic leukemia. 2021; 2(4): 1246.
Introduction
Acute Promyelocytic Leukemia (APL), a rare subtype of AML is characterized by clonal proliferation of promyelocytes, fibrinolysis, and Disseminated Intravascular Coagulation (DIC) [1]. Bleeding, often catastrophic, is common, however, thrombosis is rare. Intestinal gangrene is an unusual presentation of thrombosis of mesenteric vasculature. Moreover, bowel gangrene due to leukemic infiltration by promyelocytes has not been previously reported in literature. We hereby, report this extremely rare presentation of intestinal gangrene in a 5-year-old boy with APL secondary to leukemic infiltration.
Case summary
A five-year-old boy presented with clinical and radiological evidence of intestinal obstruction, peritonitis, and DIC.
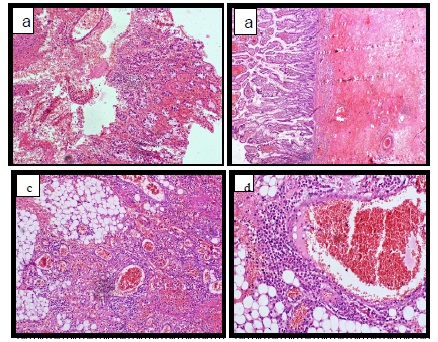
Bloodwork showed Haemoglobin (Hb) 7 g/L, WBC 4 x 109 /L and platelets of 28 x 109 /L. Bone marrow aspirate showed 95% myeloperoxidase (MPO) positive blasts with numerous Auer rods and faggot cells (Figure 1a,1b). Immunophenotyping was consistent with a diagnosis of APL. Ultrasound abdomen showed circumferential thickening of the caecum and ascending colon with ileo-caecal junction intussusception. He underwent an emergency laparotomy with resection of the gangrenous terminal ileum, caecum and ascending colon. On histopathology, the resected segments revealed leukaemic infiltration (Figure 2a,2b,2c,2d). He was extremely unwell and was commenced on emergency chemotherapy with low dose subcutaneous cytarabine (100 mg/m2 /day) chemotherapy, however, he succumbed to torrential pulmonary hemorrhage.


Acute promyelocytic leukemia is characterized by clonal proliferation of promyelocytes, fibrinolysis, proteolysis and Disseminated Intravascular Coagulation (DIC). Bleeding is a common presenting manifestation; however, thrombosis is rare. APL cells express two tumor-associated procoagulants: Tissue Factor (TF) and Cancer Procoagulant (CP) [1]. Thrombosis in APL is considered to be due to expression of TF and CP by APL cells which activates the coagulation cascade. TF is an activator of coagulation and its expression is elevated in patients with APL and APL-like cells in vitro [1]. Falanga et al. have demonstrated that compared to other leukemic cells, levels of CP are highest in patients with APL [2]. Leukemic promyelocytes secrete cytokines like IL-1b and TNF-α that mediate APL-associated coagulopathy by upregulating TF expression on endothelial cells and loss of thrombomodulin [2,3]. Thus, the effect of these cytokines is to change the normal anticoagulant endothelium to a procoagulant surface. Bowel gangrene secondary to thrombosis has been previously reported. Our case is unique as it presented with bowel gangrene secondary to intestinal leukaemic cell infiltration which has not been previously reported in literature.
Conclusions
In summary, we for the first time report this unusual presentation of intestinal gangrene secondary to leukaemic infiltration in APL as well as highlight the importance of prompt therapeutic intervention given its catastrophic nature.
References
- Bleeding and thrombosis in acute promyelocytic leukemia. Aditi Choudhry and Thomas G. DeLoughery. Am. J. Hematol. 2012; 87: 596–603.
- Falanga A, Consonni R, Marchetti M, et al. Cancer procoagulant in the human promyelocytic cell line NB4 and its modulation by all-trans-retinoic acid. Leukemia 1994; 8: 156–159.
- Moore KL, Esmon CT, Esmon NL. Tumor necrosis factor leads to the internalization and degradation of thrombomodulin from the surface of bovine aortic endothelial cells in culture. Blood 1989; 73: 159–165.