
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Primary oral tuberculosis in an immunocompetent patient
Jihene Chelli1; Asma Ben Mabrouk1*; Houcem Elomma Mrabet1; Mohamed Masmoudi2; Mehdi Hasnaoui2; Fatma Larbi Ammari1
1 Department of Endocrinology and Internal Medicine, Tahar Sfar Hospital, Mahdia 5100, Tunisia.
2 Department of Otolaryngology-Head and Neck Surgery, Tahar Sfar Hospital, Mahdia 5100, Tunisia.
*Corresponding Author: Asma Ben Mabrouk
Internal medicine and Endocrinology Department,
University Hospital Taher Sfar, 5100 Mahdia, Tunisia.
Email: asma.ben.mabrouk@gmail.com
Received : Jun 16, 2021
Accepted : Jul 27, 2021
Published : Jul 30, 2021
Archived : www.jcimcr.org
Copyright : © Mabrouk AB (2021).
Abstract
Primary tuberculosis of the tongue is very rare. The chronic ulceration is commonly misdiagnosed as a cancerous lesion. We report the case of a 44 years old immunocompetent woman who presented with a lingual chronic painful ulceration. The biopsy of the lesion showed a granulomatous inflammation, with caseous necrosis in the center. The ulceration healed after a 6 month tuberculosis treatment.
Keywords: Tuberculosis; oral; immunocompetence; ulcer.
Citation: Chelli J, Mabrouk AB, Mrabet HE, Masmoudi M, Hasnaoui M. Primary oral tuberculosis in an immunocompetent patient. 2021; 2(4): 1247.
Introduction
Tuberculosis is a very common communicable disease that mainly affects the lungs. Extra pulmonary forms are less frequent and oral lesions are rare. They, for the most, occur among immune deficient patients [1]. The non-specific presentation as a chronic ulceration could be misleading and delay the diagnosis especially in primary cases.
Case report
We report the case of a 44 years old woman, coming from a rural area of the Tunisian center, with unpasteurized dairy products consumption. Elsewhere, she did not report any history of recurrent infections, auto-immune diseases, dental care or a prior tongue traumatic lesion.
The patient consulted for a painless ulcerative lesion of the tongue with a cervical tender lymphadenopathy. These symptoms dated back to five months with no improvement after antibiotic treatment with amoxicillin and clavulanic acid. The patient did not complain about fever, cough, asthenia, anorexia nor weight loss. On physical examination, the patient did not have fever. We found an ulceration measuring 1.5 cm of the dorsal surface on the tongue without signs of inflammation. No signs evoking another tuberculosis site were found. In fact, pulmonary, abdominal and neurological examination revealed no abnormalities. No lymphadenopthies were found. The ocular fundus examination was normal.
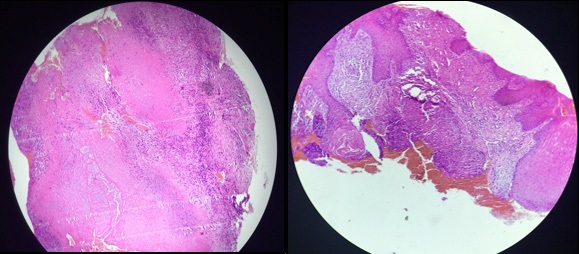
The biopsy of the tongue’s ulceration showed a granulomatous inflammation, with epithelioid macrophages and Langhans giant cells along with lymphocytes, and characteristic caseous necrosis in the center (Figure 1).
Tuberculin skin test was positive (3 cm). The complete blood count did not show any abnormality. The chest x-ray was normal. Cervical echography showed multiple bilateral lymphadenopathies with cortical widening and preservation of oval shape; the largest measuring 1.1 cm. Thoracic and abdominal tomography showed no other lesions in favor of tuberculosis. The examination of sputum and urine for acid-fast bacilli was negative. Syphilis and HIV serologies were negative, too.
The lesion healed after a six months tuberculosis treatment with rifampicin, isoniazid, ethambutol and pyrazinamide given for two months relayed by rifampicin and isoniazid for 4 months. No side effects were noted during the follow up.
Discussion
Tuberculosis (TB) is very common worldwide. The world health organization estimated that 10 million persons contracted TB in 2019, and 1.4 million actually died because of TB. Typically, this disease affects the lungs but extra-pulmonary involvement in TB accounts for about 16% of the cases [2]. Oral lesions only occurred among 0.5 to 1.5 % of the patients with tuberculosis. Lingual tuberculosis is rare, particularly in immunocompetent patients [3,4].
This type of lesions is mainly of secondary origin; lesions are due to hematogenous or lymphatic dissemination. Only few case reports of primary oral tuberculosis, like in our patient, were reported. Therefore, an exhaustive query is to be conducted in order to exclude another tuberculosis site before concluding to primary tubercular lesions. It mainly occur, like in our case, among younger patients [5].
The thickness of the squamous epithelium and the protective role of salivary enzymes and tissue antibodies makes it hard for Mycobacterium tuberculosis to invade the oral barrier [6]. Lesions mainly result from a direct inoculation of a preexistent lesion such as an extraction wound, an open pulp of carious tooth, or a perforation of erupting tooth [6,7]. Our patient did not report such lesion or a history of dental care. But a small eruption could be missed by patients.
The symptoms presented by our patient fit with the typical description of primary oral tuberculosis: A single painless ulcer with a regional lymph node enlargement [3,8]. A thorough investigation was carried out to make sure there were no other tuberculosis lesions and rule out the secondary origin of the oral ulcer.
Other oral lesions such as tuberculoma, tuberculous fissure, tubercular papilloma and tubercular cold abscess were also reported [4].
The non-specific symptoms may delay the diagnosis since the lesions could be confused with malignancy, traumatic ulcers, syphilitic ulcers, Wegener granuloma, aphthous ulcers, viral or bacterial infections and actinomycosis [1,6]. In our case the first diagnosis evoked was cancer.
Aspiration cytology could provide an early and reliable diagnosis in tongue lesions. Elsewhere deep biopsy is to be performed to confirm the diagnosis and rule out the other differential diagnosis. Histopathological findings show caseating epithelioid cell granulomas with Langhan’s and foreign body giant cells [4]. The polymerase chain reaction have a high sensitivity and specificity in the detection of Mycobacterium tuberculosis in saliva, which is by far superior to culture methods [9].
The treatment consists of the classic 6 to 10 months regimen of anti-tuberculosis drugs for oral tuberculosis. A longer course is with a favorable outcome in primary cases among immunocompetent patients and a prognosis that depends on the severity of the disease and an eventual underling immuno-depression elsewhere [1,5].
Conclusion
Although rare, primary oral tuberculosis is to be evoked when managing chronic tongue ulcerations, especially in endemic countries like ours.
References
- Ramírez Amador V, Anaya Saavedra G, González Ramírez I, Mosqueda Gómez JL, Esquivel Pedraza L, et al. Lingual ulcer as the only sign of recurrent mycobacterial infection in an HIV/ AIDS-infected patient. Med Oral Patol Oral Cir Bucal. 2005; 10: 109–114.
- OMS | Rapport sur la tuberculose dans le monde. 2021.
- Jain P, Jain I. Oral manifestations of tuberculosis: Step towards early diagnosis. J Clin Diagnostic Res. 2014; 8: ZE18-ZE21.
- Kumar S, Sen R, Rawal A, Dahiya RS, Dalal N, Kaushik S. Primary lingual tuberculosis in immunocompetent patient: A case report. Head Neck Pathol. 2010; 4: 178–180.
- Pasticci MB, Floridi P, Schiaroli E, Stagni GM, De Socio GV, et al. Lingual tuberculosis: A rare disease in Western countries. New Microbiol 2012; 35: 233–237.
- Arora KS, Garg S, Kaur P, Mohapatra S. Primary oral tuberculosis on the tongue mimicking squamous cell carcinoma. Indian J Tuberc. 2018; 65: 84–86.
- de Souza BC, de Lemos VMA, Munerato MC. Oral manifestation of tuberculosis: A case-report. Brazilian J Infect Dis 2016; 20: 210–213.
- Wu YH, Chang JYF, Sun A, Chiang CP. Oral tuberculosis. J Formos Med Assoc 2017; 116: 64–65.
- Smolka W, Burger H, Iizuka T, Smolka K. Primary tuberculosis of the oral cavity in an elderly nonimmunosuppressed patient: Case report and review of the literature. Arch Otolaryngol - Head Neck Surg. 2008; 134: 1107–1109.