
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A masked ST-elevation myocardial infarction
Michele Besana; Valentina Regazzoni; Passamonti Enrico; Valeria De Giuli; Gian Battista Danzi; Marco Loffi*
Cremona Hospital, Cremona, Italy.
*Corresponding Author: Marco Loffi
Division of Cardiology, Cremona Hospital, Viale
Concordia 1, 26100, Cremona, Italy.
Email: loffi.marco@gmail.com
Received : Jun 15, 2021
Accepted : Jul 27, 2021
Published : Jul 30, 2021
Archived : www.jcimcr.org
Copyright : © Loffi M (2021).
Abstract
Acute cardio-cerebral infarction is a rare circumstance characterized by high morbidity and mortality. It represents a management challenge due to the difficulty to choose which condition needs to be treated first. We describe the therapeutic challenge of a patient presenting with ischemic stroke and ST-elevation myocardial infarction.
Keywords: Ischemic stroke; STEMI; cardio-cerebral infarction; myocardial infarction; haemodynamic stroke.
Citation: Loffi M, Besana M, Regazzoni V, Enrico P, Giuli VD, et al. A masked ST-elevation myocardial infarction. J Clin Images Med Case Rep. 2021; 2(4): 1249.
History of presentation
A 69-year-old woman was brought to the Emergency Department for sudden onset of aphasia, right-sided homonymous hemianopsia, facial weakness and hemiparesis, (National Institutes of Health Stroke Scale [1] [NIHSS], 21). On hospital arrival oxygen saturation was 95% with Venturi mask 60% FiO2 , Arterial Blood Pressure (ABP) was 170/90 mmHg, heart rate 90 bpm, with no significant blood pressure difference between the two arms. Previously, ambulance personnel reported she had a transient hypotension with ABP of 70/40 mmHg.
GCS (Glasgow Coma Scale) was 11 and a NIHSS (National Institutes of Health Stroke Scale) [1]of 21 was identified with unremarkable general examination.
Past medical history
The patient was known for previous ST-elevation myocardial infarction in 2017 treated with percutaneous coronary intervention (PCI) and four drug-eluting stents implantation in the left anterior descending artery.
Investigations and differential diagnosis
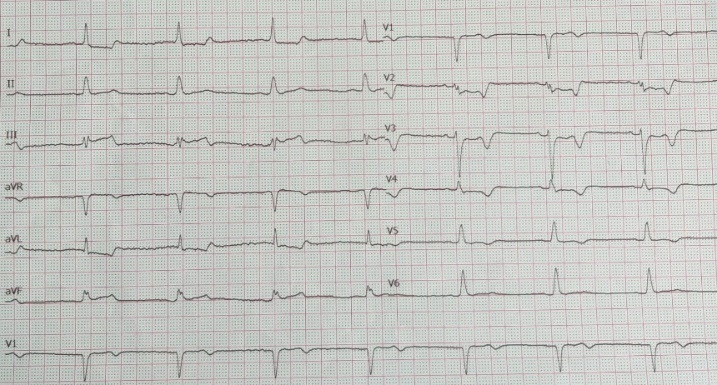
Electrocardiogram (ECG; Figure 1) at the presentation revealed a ST-elevation in inferior leads and ST depression in V2- V3 leads suggestive for ST-elevation inferior-posterior myocardial infarction (STEMI) confirmed by echocardiography, which showed moderate reduction of left ventricular ejection fraction (LVEF 40%) due to inferior and posterior walls hypokinesis.
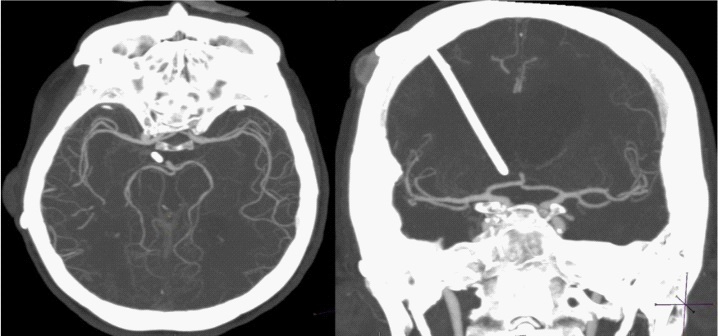
According to the clinical presentation, the most relevant condition seemed to be the neurological event. Cerebral computed tomography (CT) scan was negative for acute bleeding and, surprisingly, CT angiography revealed no cerebral main vessels obstruction and no significant stenosis on the extracranial carotid arteries (Figure 2).
Clinical conditions started to improve spontaneously (NIHSS 21→15).The main diagnostic hypothesis was an embolic phenomenon with spontaneous resolution and possible distal embolism in the small vessels not visible on CT angiography.
Management
Intravenous thrombolysis with recombinant tissue-type plasminogen activator was administered (IV rt-PA 0.9 mg/kg) with subsequent further neurological improvement (NIHSS 15→12).
Nonetheless, after few minutes the patient’s blood pressure dropped abruptly (ABP 90/60 mmHg); dobutamine (8 mcg/kg/ min) and norepinephrine (0.1 mcg/kg/min) were started without benefit and acute pulmonary edema due to cardiogenic shock developed. ECG was superimposable on the previous one with ST elevation in inferior leads. Echocardiography showed severe reduction in LVEF (30%). Blood sample tests recorded a significant increase in troponin values from 349 to 500,000 ng/L.
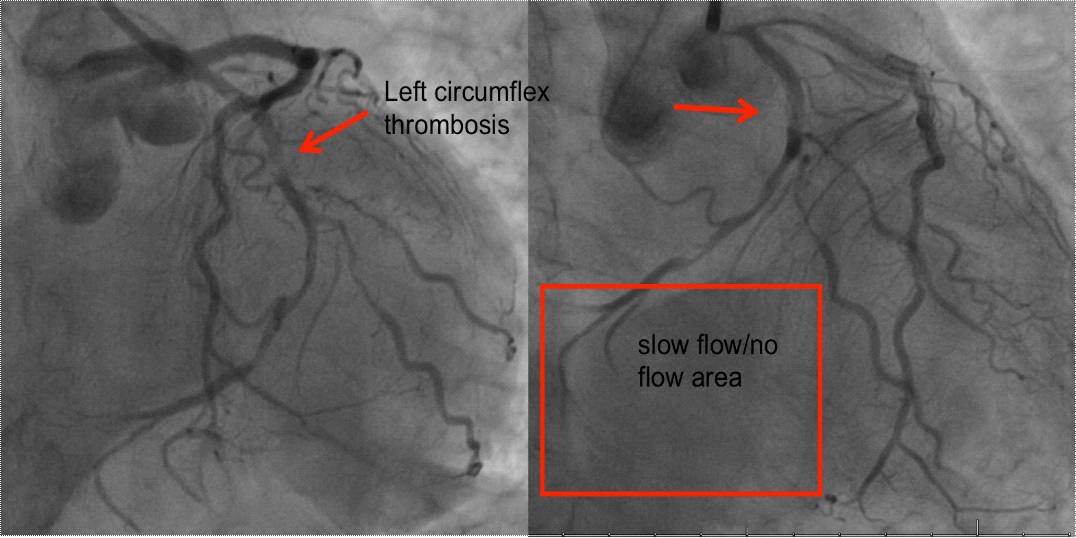
The patient was intubated and coronary angiography was performed, showing left circumflex artery thrombosis with distal embolism and slow-flow (Figure 3). 3000 IU of unfractionated heparin was administered and thrombus aspiration was performed with Export Catheter without flow improvement.
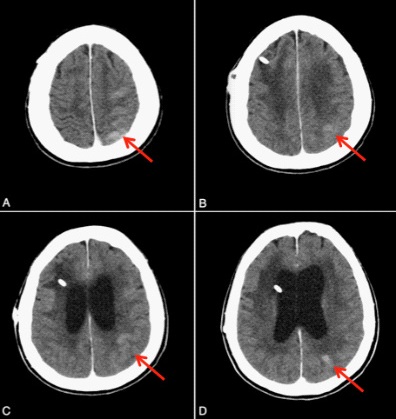
Cerebral CT scan performed 24 hours later revealed mild cortical bleeding in the left parietal lobe, probably due to hemorrhagic transformation of ischemic stroke (Figure 4).
The patient’s clinical status progressively worsened with multi-organ failure and exitus.
Unusual clinical presentation and evolution led us to reexamine the case, particularly the cerebral vascular circulation, and we realized that the left internal carotid artery was affected by severe stenosis (about 70-80%) at the supra-clinoid tract (Figure 5).
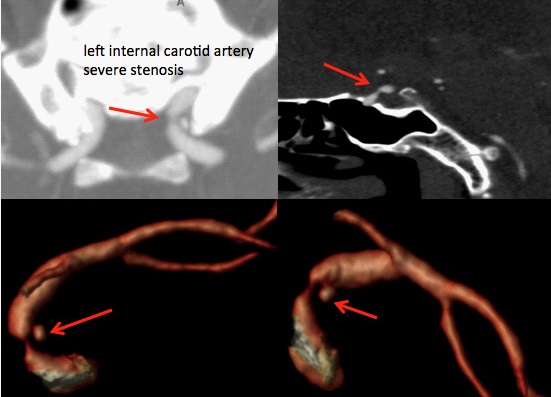
The STEMI probably caused phases of hypotension and subsequent hypoperfusion of the left-brain hemisphere owing to the left internal carotid artery stenosis. Such condition led to neurological clinical features of an ischemic stroke.
Discussion
STEMI and acute ischemic stroke are both life-threatening conditions. The simultaneous occurrence of such events, named acute cardio-cerebral infarction, is a rare circumstance with a prevalence of 0.009%, but with a high morbidity and mortality. It represents a challenge in terms of immediate management due to the difficulty to choose which condition needs to be treated first [2].
Multiple theories have been proposed about the pathogenesis of acute cardio-cerebral infarction. It has been suggested that acute myocardial infarction, especially when involving the anterior and apical wall, and the associated left ventricular systolic dysfunction, provide the substrate for the thrombus formation and increase the risk of embolization [2]. Furthermore, brain watershed infarctions can occur as a consequence of cardiac output impairment and concomitant cerebral artery stenosis [3].
In our case we did not find any occlusion of the main intracranial vessel at the cerebral CT angiography; the patient just improved significantly and spontaneously before administration of IV rt-PA and quickly became hypotensive. With the benefit of hindsight, the hypothesis of an haemodynamic stroke acquires greater significance rather than embolic mechanism.
The finding of severe left intracranial internal carotid artery stenosis supported the theory of cerebral hypoperfusion. In particular, cardiac output impairment together with carotid narrowing and, probably, the lack of compensation from the contralateral carotid and posterior circulation, led to neurological symptoms.
Calcifications of the carotid siphon or intracranial internal carotid artery are frequent findings, but significant stenosis of this segment is less common. It has been estimated that stenosis of the carotid siphon is about one-sixth as common as disease of the carotid bifurcation [4].
Intracranial stenosis is considered a marker for extensive cerebrovascular and coronary artery disease as it indicates widespread atherosclerosis; besides, it implies that the hemisphere with stenosis is at mild increased risk for an ischemic event [5].
Intracranial stenosis alone are not responsible of important acute neurological symptoms in absence of an atheroembolic mechanism and medical therapy (antithrombotic therapy, aggressive risk factor control and lifestyle changes) is the standard of care in symptomatic patients [6].
In 2018 the American Heart Association and American Stroke Association (AHA/ASA) recommended that in the setting of hyperacute simultaneous cardio-cerebral infarction, treatment with intravenous alteplase at the dose used for cerebral ischemia followed by percutaneous coronary intervention is reasonable (Class IIa; level of evidence C) [2]. Depending on the clinical picture, physicians may focus on the management of either the stroke or the STEMI.
In our case, rt-PA was administered in keeping with the guidelines, although the prevailing neurological picture masked the underlying STEMI and therefore delayed the percutaneous coronary intervention; this was fatal to our patient.
Conclusions
With this case report we want to emphasize the importance of investigating cardiac function in case of cerebral ischemic stroke symptoms without evidence of main intracranial arteries occlusion on CT angiography. Moreover, in this scenario it is useful to search for potential causes predisposing cerebral hemisphere hypoperfusion, in particular extra as well as intracranial internal carotid artery stenosis.
Learning objectives
• To investigate cardiac function in case of cerebral ischemic stroke symptoms without evidence of main intracranial arteries occlusion on CT angiography.
• To search for potential causes predisposing cerebral hemisphere hypoperfusion, in particular extra as well as intracranial internal carotid artery stenosis.
References
- National Institute of Health, National Institute of Neurological Disorders and Stroke. Stroke Scale. https://www.ninds.nih.gov/ sites/default/files/NIH_Stroke_Scale_Booklet.pdf
- Obaid O, et al. Simultaneous Acute Anterior ST-Elevation Myocardial Infarction and Acute Ischemic Stroke of Left Middle Cerebral Artery: A Case Report. Am J Case Rep, 2019; 20: 776-779c.
- SidlerD, et al. Basilar artery occlusion after acute myocardial infarction. International Journal of Cardiology. 2012; 156: e57– e59.
- Lawrence R, et al. The Prognosis of Carotid Siphon Stenosis. Stroke. 1986; 17: 1986.
- Philip G, et al. The natural history of isolated carotid siphon stenosis. J VascSurg. 1984; 1: 744-749.
- Brent F, et al. Intracranial Atherosclerosis Treatment. Stroke. 2020; 51: 3.