
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Hydatid bone disease of the humerus: A case report from East Africa
Antonio Loro*; Francesca Loro; Niall Brown
CoRSU Rehabilitation Hospital, Kisubi, Entebbe, Uganda
*Corresponding Author: Antonio Loro
CoRSU Rehabilitation Hospital, Kisubi, Entebbe,
Uganda.
Email: antonio.loro@corsuhospital.org
Received : Jun 21, 2021
Accepted : Aug 03, 2021
Published : Aug 06, 2021
Archived : www.jcimcr.org
Copyright : © Loro A (2021).
Abstract
Skeletal hydatidosis is extremely rare and involvement of the long bones of the appendicular skeleton is exceptional. We report on a case of a 68-year-old Ugandan woman who presented with a long standing history of a non-healing fracture of the mid-diaphysis of the right humerus. She had undergone multiple surgeries in peripheral health centres during the previous years. A shoulder disarticulation was carried out in our facility in agreement with the patient, who refused any other attempt of bone reconstruction. A diagnosis of hydatid bone disease was confirmed intra-operatively. There is no recurrence of the disease for a two-year follow-up period. To our knowledge this is the first case report of skeletal hydatosis in Uganda. It emphasises the diagnostic difficulties and delays, and how this led to inadequate management for the patient in this case.
Keywords: Hydatid bone disease; echinococcus; hydatidosis; echinococcus granulosus; bone infection(s).
Citation: Loro A, Loro F, Brown N. Hydatid bone disease of the humerus: A case report from East Africa. J Clin Images Med Case Rep. 2021; 2(4): 1256.
Introduction
Hydatid disease is a parasitic infection caused by the larval forms of tapeworm Echinococcus. In sheep-breeding countries, humans may become the intermediate host in the life cycle of the parasite Echinococcus granulosus. Its eggs are found in the stool or in the hair of dogs that are fed with viscera of sheep. When humans handle these pets or consume contaminated food, the larvae can cross the intestinal barrier, usually infecting the liver and lungs. The skeletal localization is rare per se, accounting for 0.5-2.5% of all localizations [1]. Of these, spine infection accounts for 50%, followed by long bones (28%), hippelvis (12%), and ribs and scapula (8%) [2-4].
Patients commonly present with pain, swelling, pathological fractures or neurological symptoms secondary to nerve compression. Hydatidosis in bone may remain clinically silent for a long time [3,5] and as such, a delay in diagnosis is common. The mainstay of treatment is radical surgical excision, which can be combined with medical therapy. Prognosis, dependent on disease localization, remains poor, especially for pelvic and spinal localizations [1].
We report a case of hydatidosis of the humerus in Uganda, which summarizes the clinical pattern of this slow growing infection from its silent course to the long delay in reaching a diagnosis. To our knowledge, this is the first case of skeletal hydatosis reported in Uganda; cases in our setting are likely to be under-reported. More widespread reporting is needed to increase awareness of the disease amongst the medical staff to aid early diagnosis, as well as for a more holistic understanding and monitoring of the disease at an epidemiological level.
Case presentation
A 68-year-old Ugandan woman presented to Mengo Hospital, Uganda, with a longstanding history of a non-healing fracture of the mid-diaphysis of the right humerus. Her symptoms started with a fracture of the right humerus five years earlier, following a trivial trauma, which was managed with an open reduction and internal fixation with plate and screws. Three weeks later, the osteosynthesis was revised due to loosening of the implant; the plate was replaced with an intramedullary Rush rod, inserted from the proximal end and augmented with a ring-type of external fixator. Two months later, leaving the osteosynthesis in situ, autologous cortico-cancellous bone grafts were applied. The external frame was ultimately removed, most probably due to the pins loosening, leaving the rod in place.
At the time of presentation to our facility, the patient was in good general condition with no comorbidities. The main complaint was right arm pain associated with important loss of function. On examination, a clean, long surgical scar was visible on the posterior aspect of the arm and there were no signs of local infection. There was pathological movement in the midthird of the arm, impairment of the shoulder joint function and reduced range of motion of the elbow joint.
The radiographs (Figure 1) showed an area of bone loss in the mid-third of the humerus, a pathological fracture, non-union and an enlargement of the medullary cavity in the distal diaphyseal-metaphyseal area with thinning of the cortices. There was avascular necrosis of the humeral head. The intramedullary rod showed signs of loosening; an isolated loose screw from the first osteosynthesis was still present. The preoperative blood workup was unremarkable.
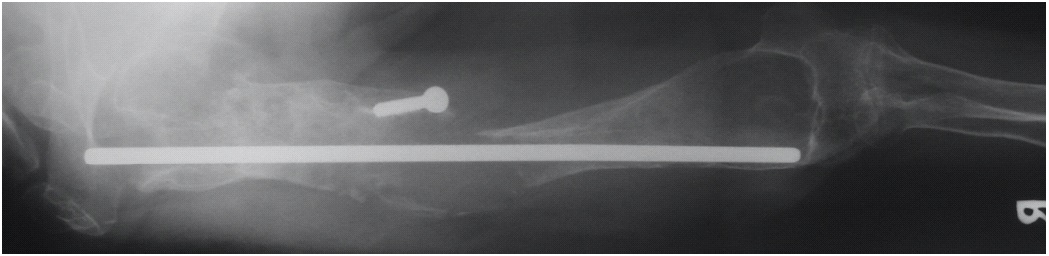
On the basis of preoperative radiographic features, a tumor or an underlying chronic infection, namely tuberculosis, were suspected.
A shoulder disarticulation was carried out in agreement with the patient, who refused any other attempt of bone reconstruction. The postoperative phase was uneventful and no medical therapy was initiated.
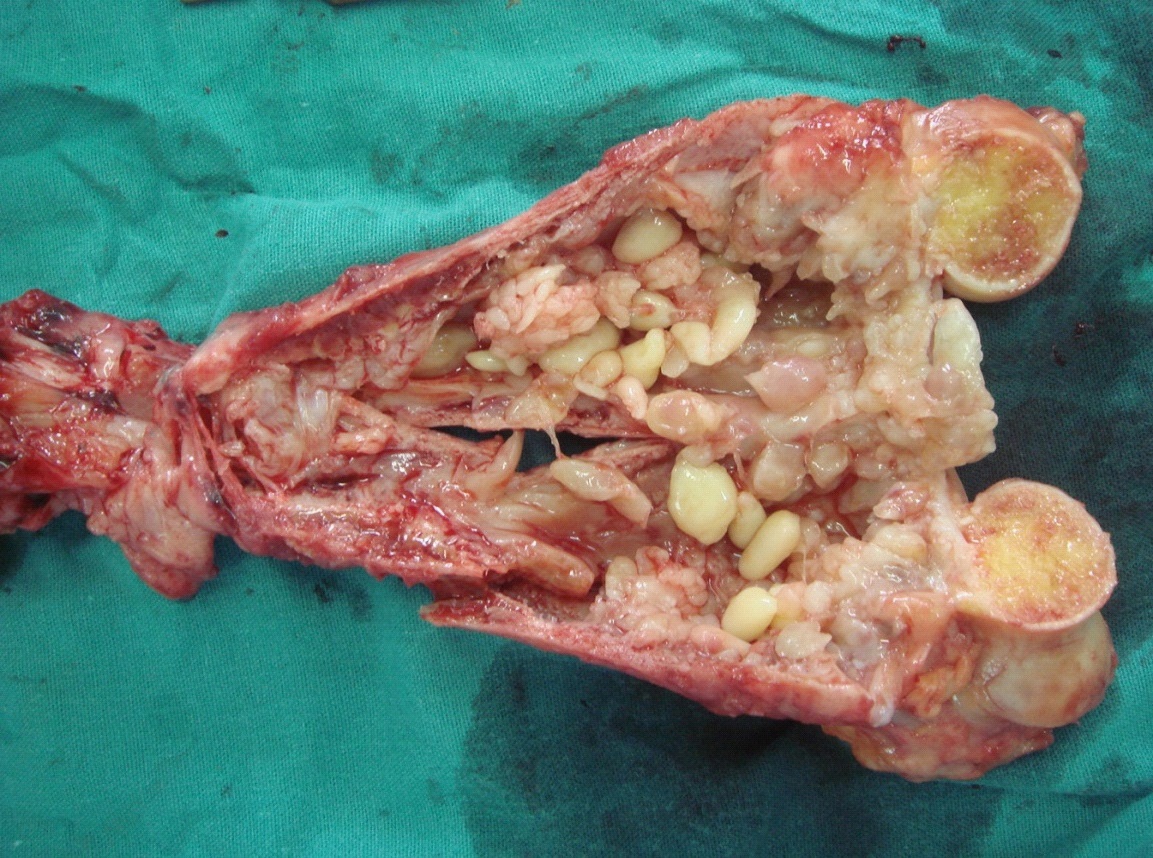
The post-operative macroscopic examination of the humerus revealed involvement of the entire bone by a chronic infection. The cortices were extremely thin and friable. The distal half showed a gross, fusiform enlargement. Numerous yellow cysts, both at the level of the non-union and in the distal medullary canal, were noted. Appearances were in keeping with the typical “Grapes” or “Bubbles of soap” caused by an Echinococcus granulosus infection (Figure 2). The entire bone was sent for histology, of which the report described features consistent with a diagnosis of chronic osteomyelitis and chronic nodular synovitis. Polypoid growth in the marrow cavity was described without any mention of cestode infection. No complication or recurrence were observed over the two-year follow-up period.
Discussion
Isolated hydatidosis of long bones is very rare [1,4,5]. A high index of suspicion is needed in the presence of a long-standing, slow growing bone disorder in sheep-rearing areas in the Mediterranean basin, the Middle East, East Africa, Central Asia and South America. Extensive skeletal lesions may lead to presumptive diagnoses of more common conditions such as bone tumors, fibrous dysplasia, specific infections, myeloma or bone cysts.
When the skeleton is affected, the spine is the most common localization (50% of cases), followed by hip and pelvis. Other sites include femur, tibia, rib, scapula, and humerus. Since the parasite grows very slowly in the bone, the disease can be asymptomatic for several years, with clinical silence of 10 to 20 years not being uncommon [6]. The growth of the larva is atypical in bone: the invasion of the spongiosa and the marrow spaces occurs slowly and leads to bone resorption. Thus, in longstanding cases there is extensive erosion of the medullary canal and thinning of the cortices.
It is extremely difficult to make a diagnosis of bone hydatidosis in the preoperative stage. The disease is often overlooked, the routine blood tests are unhelpful and the radiographic features are non-specific. The diagnosis is usually made intraoperatively and may be confirmed by histologic examination post-operatively.
When available, computed tomography and magnetic resonance imaging are useful tools for confirming the diagnosis of the disease, for evaluating the extent of the bone lesions and for ruling out involvement of the surrounding soft tissues [5,7,8]. Unfortunately, these are not easily available in our setting.
Radical resection is the goal of surgery for osseous hydatidosis. This can be difficult to achieve in certain localizations or in the presence of extensive involvement of the affected bone. Recurrence can follow incomplete removal of the lesion. Surgery in the pelvis might be disappointing [5] since wide resection of the lesion is often impossible. For the patient in our case report, eradication and reconstruction were thought impossible. Shoulder disarticulation was chosen as management due to the extension and the severity of the infection, with loss of upper limb function.
No chemotherapy was instituted in the present case. However, when medical therapy is necessary, the anthelmintic drug of choice is Albendazole, proven more efficacious than Mebendazole [9]. Its use is advocated both before and after surgical treatment [10-11].
Prognosis remains poor and, if mismanaged, long-term prognosis is comparable with that of cancer [11].
Conclusion
This case report summarizes the clinical pattern of this slow growing infection and highlights the difficulties in reaching an early diagnosis. The delay in diagnosis unfortunately lead to physical and financial harm to the patient in this case report, with multiple inadequate and unnecessary surgeries being performed. A high index of suspicion is needed for an early diagnosis, which can be helped by increased reporting and education of the health care staff in endemic areas.
References
- Zlitni M, Ezzaoula K, Lebib H, Karray M, Kooli M, et al. Hydatid cyst of bone: diagnosis and treatment. World J Surg. 2001; 25: 75-82.
- Sami A, Elazhari A, Ouboukhlik A, Elkamar A, Jiddane M, et al. Hydatid cyst of the spine and spinal cord. Study of 24 cases. Neurochirurgie. 1996; 42: 281-7.
- Yildiz Y, Bayrakci K, Altay M, and Saglik Y. The use of polymethylmethacrylate in the management of hydatid disease of bone. J Bone Joint Surg Br. 2001; 83-B: 1005-8.
- Duran H, Fernandez L, Gomez-Castresana F, Lopez-Duran L, Mata P, et al. Osseous hydatidosis. J Bone Joint Surg Am. 1978; 60: 685-90.
- Herrera A, Martinez A. Extraspinal bone hydatidosis. J Bone Joint Surg Am. 2003; 85-A: 1790-4.
- Hooper J, McLean I. Hydatid disease of the femur: report of a case. J Bone Joint Surg Am. 1977; 59-A: 974-976.
- El Quessar A, Jroundi L, Tizniti S, Cisse M, Chakir N, et al. CT and MRI features of spinal hydatidosis. A report of 8 cases. J Radiol. 2001; 89: 917-21.
- Ciftdemir M, Sezer A, Puyon FO, Copuroglu C, Ozcan M. Hydatid disease of the femur with an extraosseus extent due to a former biopsy complicated by a pathological fracture. Case reports in Orthopedics. 2012: 169545: 1-4.
- Bonifacino R, Dogliani E, and Craig PS. Albendazole treatment and serological follow-up in hydatid disease of bone. Int Orthop. 1997; 21:127-32.
- Szypryt EP, Morris DL, and Mulholland RC. Combined chemotherapy and surgery for hydatid bone disease. J Bone Joint Surg Br. 1987; 69: 141-4.
- Cattaneo L, Manciulli T, Cretu CM, Giordani MT, Angheben A, et al. Cystic Echinococcosis of the Bone: A European Multicenter Study. Am J Trop Med Hyg. 2019; 100: 617-621.