
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Management of neuroendocrine tumors of the extrahepatic bile duct: Case report and review of the literature
Luca Portigliotti1*; Fabio Maroso1; Andrea Amabile1; Filadelfio Massimiliano Nicolosi1; Fabio Colli1; Fabio Frosio1; Oscar Soresini1; Nicola de’Angelis2; Renzo Luciano Boldorini3; Raffaele Romito1
1 General Surgery Department, A.O.U. “Maggiore della Carità” Hospital, Novara, Italy.
2 Minimally Invasive and Robotic Digestive Surgery Unit, Regional General Hospital F. Miulli, Acquaviva delle Fonti (Bari), Italy and University Paris Est - UPEC, France.
3 Department of Health Science, School of Medicine, University of Eastern Piedmont “Amedeo Avogadro”. Pathology Unit, “Maggiore della Carità” Hospital.
*Corresponding Author: Luca Portigliotti
General Surgery Department, A.O.U. “Maggiore
della Carità” Hospital, Corso Mazzini 18, 28100,
Novara, Italy.
Email: luca.portigliotti@maggioreosp.novara.it
Received : July 01, 2021
Accepted : Aug 09, 2021
Published : Aug 12, 2021
Archived : www.jcimcr.org
Copyright : © Portigliotti L (2021).
Abstract
Neuroendocrine tumors of the extrahepatic bile duct (EBNETs) are exceedingly rare neoplasms, whose diagnostic and therapeutic process can be challenging. We present the case of a 58-year-old EBNET patient successfully treated at our Institution, followed by a systematic review of the literature on the surgical management of these rare tumors.
Keywords: neuroendocrine tumor; biliary neoplasm; carcinoid; biliary tract obstruction
Citation: Portigliotti L, Maroso F, Amabile A, Nicolosi FM, Colli F, et al. Management of neuroendocrine tumors of the extrahepatic bile duct: Case report and review of the literature. J Clin Images Med Case Rep. 2021; 2(4): 1263.
Case presentation
Neuroendocrine tumors (NETs) represent a rare, heterogeneous group of neoplasms with a distinct functional and biological behavior depending on their anatomic location, tumor size and clinical symptoms [1]. More than 50% of NETs arises in the gastrointestinal tract, being the appendix, the small bowel and the rectum the most common locations [2]. NETs located within the extrahepatic bile duct (EBNETs) are amongst the rarest primary sites, accounting for 0.2%-2% of all such malignancies [3,4] .
Obtaining a preoperative diagnosis of these tumors is difficult. Indeed, the majority of cases reported in the literature are diagnosed only after surgery, on the final pathological examination of the surgical specimen. Plasmatic Chromogranin A (CgA) and urinary 5-hidroxyindole acetic acid (5-HIAA) are slightly specific markers that can be used in combination to hypothesize the presence of NETs. Nevertheless, since, the majority of EB NETs are non-functioning neoplasms, these markers may not be produced, secreted and therefore detected. Computed Tomography (CT) scan and Magnetic Resonance Cholangiopancreatography (MRCP) are the recommended imaging exams to stage EBNETs and to plan the operative strategy. However, no specific CT or MRCP findings allowing distinguishing between EBNETs and other biliary neoplasms have been described so far. More sensitive and specific radiological techniques are available. Above all, positron emission tomography (PET) with radioactively labeled somatostatin analogues (like Ga68 DOTA-TATE, DOTATOC and DOTANOC) can be useful in case of clinical suspicion of EBNETs, in both localized and metastatic settings, with a reported sensitivity and specificity of 81% and 90%, respectively [5]. The accuracy of endobiliary brush cytology for the preoperative diagnosis of biliary disease has been widely discussed [6], but its sensitivity for biliary tree tumors is limited. This particularly applies to EBNETs, considering the submucosal localization of the lesion [7,8]. Finally, fine needle aspiration cytology (FNAC) and biopsy (FNAB) could be an helpful diagnostic tools [8], however in most cases a surgical exploration is still mandatory, in the suspicion of cholangiocarcinoma.
From a surgical standpoint, the resection of the extrahepatic bile ducts with portal lymphadenectomy and Roux-en-Y hepaticojejunostomy provides radical tumor clearance in most cases. In very selected patients a more extensive resection may be required, with various degrees of hepatic or pancreatic resection according to the tumor site.
In this paper, we present the case of a 58-year-old patient with an EBNET treated at our Institution. Moreover, we performed a systematic review of the literature on the surgical management of these rare neoplasms.
Case report
A 58-year-old man with history of type 2 diabetes and polycythaemia vera presented to our Hospital complaining of epigastric pain. Symptoms had started one month earlier. An Esophago-Gastro-Duodenoscopy (EGDS) showed mild gastritis (negative for Helicobacter pylori). Abdominal US demonstrated the presence of a mass (28 x 28 mm) located within the extrahepatic bile duct, causing diffuse dilatation of the intrahepatic biliary system. Despite the degree of ductal dilation, liver function tests and serum markers of cholestasis were within the normal ranges. The levels of alpha-fetoprotein, CA 19-9 and CEA were unremarkable. Endoscopic Ultrasound (EUS) showed a 28 mm hyperechoic lesion, with arterial and venous contrast enhancement after injection of SonoVue® contrast-agent; EUS confirmed the dilation of both right and left hepatic ducts, encompassing the cystic and the common bile duct, and also detected the presence of two reactive nodes within the hepatoduodenal ligament. A Fine Needle Biopsy (FNB) was performed and pathological analysis reported signet-ring cells adenocarcinoma. Since the patient did not present with jaundice, Endoscopic Retrograde Cholangiopancreatography (ERCP) was not performed. Abdominal CT-scan and MRCP revealed a mass of 28 x 24 mm in the common bile duct, without any suspicious nodes nor distant metastases.
The case was submitted to our Institutional Board and the patient was considerate candidate for exploratory surgery, followed by a bile duct resection, eventually associated with extended pancreatic or liver resection (established through intraoperative frozen section assessment of surgical margins).
At the laparotomic abdominal exploration, there was no evidence of carcinomatosis or distant metastases. The extrahepatic bile duct and the gallbladder were resected, and a radical lymphadenectomy of the liver pedicle was performed. The proximal and distal common bile duct margins were negative for malignancy on frozen section analysis, so a Roux-en-Y hepaticojejunostomy was finally performed. The postoperative course was unremarkable, and the patient was discharged on the post-operative day 6.
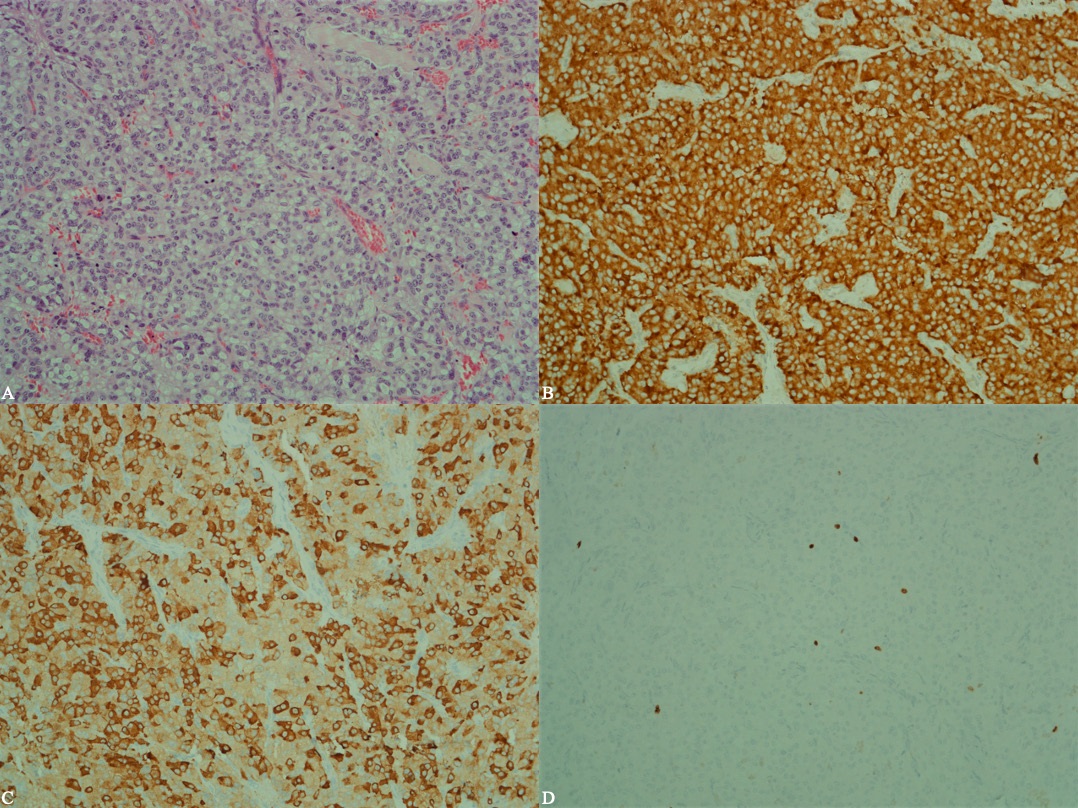
The final pathological analysis (Figure 1) demonstrated a G2 EBNET of 35 x 30 x 25 mm, Synaptophysin++, CgA+, infiltrating both the hepatic and the cystic duct, with ulceration of the mucosal layer. The lesion had solid-trabecular and pseudo-glandular growth pattern. The mitotic index was 2 for 10 high power fields, and Ki-67 labeling index was 5%. A neural invasion, but no vascular invasion, was detected. Lymph nodes examination did not detect any metastases.
Thus no adjuvant therapy was proposed by our Board. 6- and 12-month CT scans showed no evidence of local recurrence or distant metastases. At the 16-month follow-up, the patient is in good health, completely asymptomatic and with normal blood chemistry tests.
Review of the literature
We aimed at conducting a comprehensive systematic review and collecting data of all ENNETs cases which have been reported in the literature.
Materials and methods
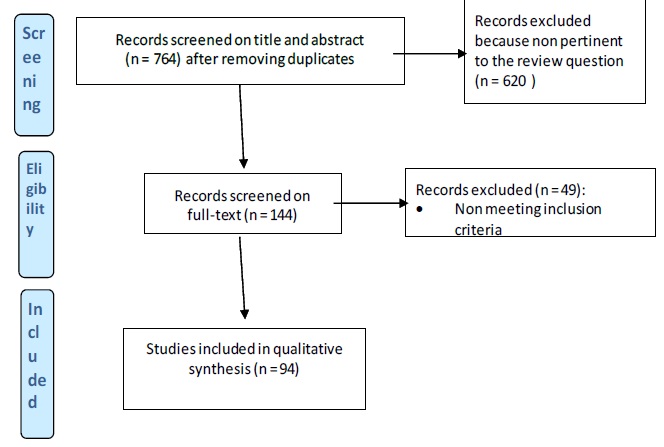
The review of the literature was conducted through a systematic approach, following the PRISMA statements checklist (Figure 2). The following online databases were consulted: MEDLINE (through PubMed), EMBASE, Google Scholar, Cochrane and ProQuest Dissertations, and Thesis Database.
In order to increase the accuracy in identifying relevant articles, a research equation was formulated for each database, using specific keywords and/or MeSH terms (i.e., “neuroendocrine tumor”, “Carcinoid”, “Bile Duct”). In addition, bibliography from both eligible studies and relevant review articles (not included in the systematic review) was crosschecked in order to identify additional reports. A grey literature search was also performed using the OpenGrey database.
No time restrictions were applied. Relevant articles were defined as those written in English and reporting at least the following clinical, radiological and pathological patients’ characteristics: age, gender, tumor location and size, symptoms, presence of metastases, time of diagnosis, treatment, immunohistochemistry, pathology, and follow-up data.
The studies eligible for inclusion, e.g., case report, case series have been all those answering to specific research question “How to manage successfully EBNETs patients?”
Reports of tumors involving intra-hepatic biliary ducts, liver parenchyma, gallbladder, and Vater region were excluded. Reports of Neuroendocrine Carcinomas (NEC) and mixed tumors, including both NET and adenocarcinoma features, were also excluded. Two reviewers (LP and FM) independently retrieved, screened and analyzed the selected studies. Conflicts between the two independent reviewers were solved with discussion with a third one (RR). A quality assessment and risk of bias of every study selected has been performed using tool described by Murad et al.
Results
Studied population
After removal of duplicates, the literature search identified a total of 763 articles. Of these, 619 were excluded upon title and abstract evaluation because they were not pertinent to topic. Out of the remaining 143 articles that underwent full-text evaluation, 49 were ruled out because they did not meet the inclusion criteria. Therefore, 94 articles, ranging from 1959 to 2020, were finally included in our systematic review (Table 1). Overall, 95 patients diagnosed with EBNETs were considered, 37 men (38.95%) and 58 women (61.05%). The mean age at the diagnosis was 47.48 ± 17.3 years. The main characteristics of the pooled population are summarized in Table 2.
Table 1
1st Author |
Year |
Sex |
Age |
Location |
Max size |
Time of diagnosis |
Final diagnosis |
Treatment |
Metastasis |
F/up |
Pilz (35) |
1961 |
F |
55 |
CBD |
|
histology |
|
Lap-B |
0 |
|
Little (16) |
1968 |
F |
41 |
PCBD |
|
Preoperative (elevate urine 5-HIAA level) |
|
Lap-B |
1 |
3 weeks |
Schwesinger (36) |
1978 |
F |
72 |
DCBD |
2 |
histology |
|
|
0 |
|
Gerlock (37) |
1979 |
M |
32 |
PCBD |
4 |
histology |
|
BDR |
0 |
|
Vitaux (38) |
1981 |
M |
30 |
DCBD |
1,5 |
histology |
|
PD |
0 |
48 months |
Goodman (10) |
1984 |
F |
28 |
CD |
|
histology |
|
CH-C |
0 |
9 m |
Jutte (39) |
1986 |
M |
62 |
CHD |
5,5 |
histology |
|
BDR + right/left HJ |
0 |
24.5 m |
Gastinger (40) |
1987 |
F |
65 |
PCBD |
1 |
histology |
|
TR |
1 |
5 m |
Reinhardt (41) |
1988 |
F |
71 |
CBD |
2,5 |
histology |
|
PPPD |
0 |
12 m |
Fujita (42) |
1989 |
F |
55 |
CHD |
2 |
histology |
|
choledothomy, TR, T-tube |
0 |
6 m |
Chittal (43) |
1989 |
F |
46 |
CD |
0,8 |
histology |
|
Ch-C, partial BDR |
0 |
36 m |
Van der Wal (44) |
1989 |
M |
55 |
CHD-CD |
4 |
histology |
|
RYEJ |
0 |
12 m |
Bumin (45) |
1990 |
F |
38 |
CBD |
2 |
histology |
|
Ch-C, choledothomy, TR, T-tube |
0 |
|
Fellows (46) |
1990 |
M |
30 |
PCBD |
1,5 |
histology |
|
RYEJ |
0 |
|
Brown (47) |
1990 |
F |
35 |
CHD-B |
2 |
histology |
|
RYEJ |
0 |
|
Angeles-Angeles (48) |
1991 |
F |
39 |
CBD |
1,5 |
histology |
|
BDR + hepaticoduodenal anastomosis |
0 |
42 m |
Newman (49) |
1992 |
F |
15 |
DCBD |
|
histology |
|
PPPD |
0 |
48 m |
Rugge (50) |
1992 |
F |
64 |
CBD-CD |
2,5 |
histology |
|
RYEJ |
0 |
12 m |
Ueyama (51) |
1992 |
F |
60 |
CBD |
1,5 |
histology |
|
TR + segmentectomy |
0 |
|
Gembala (52) |
1993 |
M |
28 |
RHD-CHD |
3 |
histology |
|
Trisegmentectomy + HJ |
0 |
|
Sankary (53) |
1995 |
F |
47 |
PCBD |
2 |
histology |
|
Trisegmentectomy + HJ |
0 |
48 m |
Mandujano (11) |
1995 |
F |
53 |
DCBD |
2,2 |
gastrinoma |
|
CH-C + TR |
0 |
8 m |
Belli (54) |
1996 |
M |
78 |
PCBD |
1,5 |
histology |
|
RYEJ |
0 |
15 m |
Kopelman (33) |
1996 |
F |
44 |
CBD |
0,5 |
histology |
|
PPPD+ resection of left metastasis |
1 |
18 m |
Hao (12) |
1996 |
M |
42 |
CBD |
1,3 |
histology |
|
OLT |
0 |
5 m |
Meyer (55) |
1997 |
F |
56 |
CD |
|
histology |
|
CH-C, CDR |
0 |
96 m |
Shah (56) |
1998 |
F |
52 |
CD |
0,5 |
histology |
|
CH-C |
0 |
|
Oikawa (57) |
1998 |
M |
70 |
CBD-CD |
2,5 |
histology |
|
RYEJ+ liver resection |
1 |
6 m |
Bembenek (58) |
1998 |
F |
12 |
CHD |
1,5 |
histology |
|
RYEJ |
0 |
9 m |
Ross (59) |
1999 |
F |
65 |
DCBD |
2,5 |
histology |
|
PD |
0 |
17 m |
Perakath (60) |
1999 |
F |
36 |
CHD |
|
histology |
|
RYEJ |
0 |
6 m |
Hermina (61) |
1999 |
M |
69 |
CD |
0,5 |
histology |
|
RYEJ+Ch-C |
0 |
14 m |
Chamberlain (4) |
1999 |
F |
37 |
CHD-B |
2,7 |
histology |
|
RYEJ |
0 |
96 m |
Martignoni (62) |
1999 |
M |
60 |
CHD |
1,3 |
gastrinoma |
|
TR+T tube |
0 |
36 m |
Aronsky (63) |
1999 |
F |
64 |
CD |
0,4 |
histology |
|
RYEJ+Ch-C |
0 |
47 m |
Aronsky (63) |
1999 |
F |
51 |
CD |
|
histology |
|
RYEJ+Ch-C+ liver resection |
0 |
49 m |
Chan (64) |
2000 |
M |
14 |
CHD-B |
2,8 |
histology |
|
RYEJ+PTBD |
0 |
36 m |
Juturi (65) |
2000 |
M |
43 |
DCBD |
4 |
histology |
|
PD |
0 |
42 m |
Maitra (66) |
2000 |
F |
42 |
CBD |
1,1 |
histology |
|
RYEJ |
0 |
132 m |
Maitra (66) |
2000 |
F |
61 |
CHD-B |
2 |
histology |
|
RYEJ+Ch-C |
0 |
48 m |
Maitra (66) |
2000 |
F |
|
CBD |
1,4 |
histology |
|
RYEJ |
0 |
120 m |
Maitra (66) |
2000 |
F |
37 |
CHD |
2,7 |
histology |
|
RYEJ+Ch-C |
0 |
24 m |
Maitra (66) |
2000 |
F |
67 |
CHD |
2,5 |
histology |
|
RYEJ+Ch-C |
0 |
24 m |
Turrion (67) |
2002 |
F |
51 |
CHD-B |
2,7 |
histology |
|
OLT |
0 |
18 m |
Pawlik (68) |
2003 |
M |
59 |
PCBD |
2 |
histology |
|
RYEJ |
0 |
6 m |
Podnos (69) |
2003 |
F |
65 |
DCBD |
2,2 |
biopsy during Ch-C |
|
RYEJ |
0 |
37 m |
Volpe (70) |
2003 |
M |
19 |
PCBD |
1 |
biopsy during Ch-C |
|
RYEJ |
0 |
12 m |
El Rassi (71) |
2004 |
F |
41 |
LHD-H |
4 |
histology |
|
left hepatectomy + right HJ |
0 |
240 m |
El Rassi (71) |
2004 |
M |
79 |
DCBD |
0,2 |
histology |
|
PPPD |
1 |
34 m |
Menezes (72) |
2004 |
M |
30 |
CHD-CD |
3 |
histology |
|
RYEJ |
0 |
18 m |
Ligato (73) |
2005 |
F |
33 |
CHD |
3,9 |
histology |
|
RYEJ |
0 |
10 m |
Pithawala (74) |
2005 |
F |
38 |
CBD |
5 |
biopsy during Ch-C |
|
RYEJ |
0 |
2 m |
Hubert (75) |
2005 |
F |
46 |
CHD-CD |
2,5 |
histology |
|
RYEJ+Ch-C |
0 |
102 m |
Hubert (75) |
2005 |
M |
50 |
CD |
0,4 |
biopsy during ERCP |
|
RYEJ+Ch-C+ RFA for liver metastasis |
1 |
|
Nesi (14) |
2006 |
M |
30 |
DCBD |
1,8 |
Preoperative (elevate blood serotonin level) |
|
PPPD |
0 |
84 m |
Tzimas (76) |
2006 |
F |
29 |
LHD |
2,8 |
histology |
|
left hepatectomy + caudater lobe, right HJ |
0 |
24 m |
Kim (77) |
2006 |
F |
67 |
DCBD |
1,6 |
histology |
|
PPPD |
0 |
10 m |
Caglikulekci (78) |
2006 |
F |
40 |
CBD |
0,7 |
biopsy during Ch-C |
|
BDR |
0 |
14 m |
John (79) |
2006 |
F |
67 |
CBD |
|
histology |
|
PD |
0 |
|
Honda (80) |
2006 |
M |
76 |
DCBD |
1,4 |
histology |
|
PD |
1 |
8 m |
Ferrone (81) |
2007 |
M |
52 |
RHD-H |
2,2 |
histology |
|
Right Trisegmentectomy + BDR |
0 |
|
Sethi (82) |
2007 |
M |
51 |
PCBD |
2,8 |
histology |
|
RYEJ |
0 |
22 m |
Todoroci (83) |
2007 |
M |
73 |
DCBD |
1,2 |
histology |
|
PPPD |
0 |
12 m |
Colombo (84) |
2007 |
M |
52 |
CBD |
2 |
histology |
|
RYEJ |
0 |
41 m |
Stavridi (85) |
2008 |
F |
49 |
CD |
1,4 |
histology |
|
CH-C |
0 |
12 m |
Nafidi (86) |
2008 |
F |
31 |
CBD |
1,2 |
histology |
|
RYEJ |
0 |
|
Gusani (87) |
2008 |
F |
43 |
CHD |
2,5 |
histology |
|
RYEJ |
0 |
132 m |
Ferekouras (88) |
2009 |
F |
60 |
CD |
2,1 |
histology |
|
RYEJ+ STENT |
1 |
112 m |
Price (15) |
2009 |
F |
55 |
CHD-CD |
0,6 |
gastrinoma |
|
choledothomy, TR, T-tube + RFA liver metastasis |
1 |
24 m |
Price (15) |
2009 |
F |
33 |
DCBD |
|
gastrinoma |
|
PPPD |
0 |
24 m |
Tonnhofer (89) |
2009 |
F |
6 |
CHD |
|
histology |
|
RYEJ |
0 |
24 m |
Squillaci (90) |
2010 |
M |
70 |
CHD |
4,5 |
biopsy during Ch-C |
|
left hepatectomy + BDR, HJ |
0 |
59 m |
Zhan (91) |
2010 |
M |
10 |
DCBD |
2 |
histology |
|
PD |
0 |
12 m |
Cappell (92) |
2011 |
M |
42 |
DCBD |
1,8 |
histology |
|
PD |
0 |
|
Bhalla (93) |
2012 |
F |
28 |
CHD |
2 |
histology |
|
RYEJ |
0 |
4 m |
Linder (94) |
2013 |
M |
82 |
CBD |
1,9 |
histology |
|
PD |
0 |
6 m |
Yasuda (95) |
2013 |
F |
69 |
Hilar |
2,5 |
histology |
|
RYEJ |
0 |
2y |
De Luca (96) |
2013 |
M |
78 |
CBD |
3 |
histology |
|
PD |
0 |
|
Navas Cuellar (97) |
2014 |
F |
37 |
CBD |
4 |
histology |
|
RYEJ |
0 |
|
Yalav (98) |
2014 |
M |
16 |
CBD |
|
histology |
|
RYEJ |
0 |
40 m |
Sung Bae Park (99) |
2014 |
F |
75 |
CBD |
2,7 |
histology |
|
RYEJ |
0 |
12 m |
Safwan (9) |
2016 |
F |
41 |
CBD |
2,8 |
Ga68DOTA-TATE |
|
|
0 |
19 m |
Hosoda (100) |
2016 |
M |
35 |
CBD |
1,1 |
histology |
|
RYEJ |
0 |
|
Sanchez-Cabùs (101) |
2016 |
M |
38 |
CBD |
2 |
histology |
|
RYEJ |
0 |
|
Brig (102) |
2016 |
F |
45 |
CBD |
3,2 |
histology |
|
PD |
0 |
|
Khan (103) |
2016 |
M |
64 |
CBD |
1,3 |
histology |
|
RYEJ |
0 |
|
Murakami (104) |
2016 |
F |
51 |
CBD |
1,8 |
histology |
|
RYEJ |
0 |
|
Abe (26) |
2017 |
F |
57 |
CBD |
3 |
histology |
|
RYEJ |
0 |
34 m |
Costin (105) |
2017 |
F |
37 |
CBD |
|
histology |
|
RYEJ |
0 |
2y |
Hoepfner (106) |
2017 |
M |
45 |
CBD |
4 |
histology |
|
RYEJ |
0 |
6 m |
Zhang (107) |
2018 |
F |
56 |
CBD |
6 |
histology |
|
RYEJ |
0 |
8 m |
Choi (25) |
2019 |
F |
33 |
CBD |
2 |
citology brushing |
|
RYEJ |
0 |
10 m |
Chaouch (108) |
2019 |
M |
39 |
CBD |
2,4 |
histology |
|
RYEJ |
0 |
12 m |
Umezaki (109) |
2019 |
M |
59 |
CBD |
2,5 |
histology |
|
RYEJ |
0 |
11 m |
Park (110) |
2019 |
M |
58 |
CBD |
6,2 |
histology |
|
RYEJ |
0 |
12 m |
Table 2
|
NET VB |
Gender (male) |
37 (38.9%) |
Age (years) |
48 (± 17.3) |
Location |
69 (62,1%) 11 (11,6%)
36 (37,9%) 13 (13,7%) |
Maximum diameter (cm) |
2.2 (± 1.2) |
Symptoms (main) |
|
Time of diagnosis |
82 (86.3%) |
Metastasis |
|
Treatment |
|
Immunohistopathology |
74 (79.6%) |
90-day mortality rate |
1 (1.2%) |
Mean follow-up (months) |
33.3 (± 39.7) |
Symptoms
Most patients were symptomatic, (n= 89, 92.7%), being jaundice the most frequent symptom (n=61, 65.6%). Other aspecific symptoms reported were abdominal pain or discomfort, nausea, vomiting, and pruritus; they were related to the compression of the bile duct or to the presence of a growing mass in the right hypochondrium.
The great majority of the neoplasms were non-functioning NET. Only 5 cases (5,4%) were associated with hormone hypersecretion [9-14] and the serum levels of 5-hydroxyindoleacetic acid (5-HIAA) were slightly elevated in two cases [13,15]; however, a true carcinoid syndrome has never been reported in patients with EBNETs.
Tumor location
The most frequent location was the common hepatic duct in 37,9% of cases (n=36), followed by the middle portion of common bile duct (34,8 %) while the distal part of CBD was involved in 15 cases (15,7%). Cystic duct was involved in 14 cases (14,7%) and proximal common bile duct (11,6 %). The tumor size has been reported 87 cases (91.5%), and its mean diameter was 2.2 cm (range, 0.2 – 6.2cm).
Type of intervention and outcomes
Several surgical options have been reported for patients with EBNETs, according to the location and extension of the neoplasm. The most frequently performed procedure was Biliary Duct Resection (BDR) and Roux-en-Y hepaticojejunostomy (RYHJ) (59.1%). Pancreatic and liver resections were performed in 27 patients (28.4%). Neoplasms were located within the cystic duct in 5 patients (5.3%), and cholecystectomy was considered an adequate treatment in all these cases. Finally, in 4 cases (4.2%) a radical resection was not possible and thus only biopsies were taken. The disease was metastatic at time of diagnosis in 26 cases (27.4%), with nodal involvement in 17 (17.7%) and liver metastases in 9 cases (9.4%). Immunohistochemistry staining was performed in all cases; the different markers expressed by the neoplasms are reported in Table 1.
The mortality rate in the postoperative period was low (n=1, 1.05%). Follow-up surveillance data were available for 71 patients (74.7%) and ranged from 1 to 240 months.
References
- Klöppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci. 2004; 1014: 13-27.
- Thompson GB, van Heerden JA, Martin JK, Schutt AJ, Ilstrup DM, Carney JA. Carcinoid tumors of the gastrointestinal tract: resentation, management, and prognosis. Surgery. 1985; 98: 1054-63.
- Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer. 1997; 79: 813-29.
- Chamberlain RS, Blumgart LH. Carcinoid tumors of the extrahepatic bile duct. A rare cause of malignant biliary obstruction. Cancer. 1999; 86: 1959-65.
- Haug AR, Cindea-Drimus R, Auernhammer CJ, Reincke M, Wängler B, Uebleis C, et al. The role of 68Ga-DOTATATE PET/CT in suspected neuroendocrine tumors. J Nucl Med. 2012; 53: 1686- 92.
- Selvaggi SM. Biliary brushing cytology. Cytopathology. 2004; 15: 74-9.
- Govil H, Reddy V, Kluskens L, Treaba D, Massarani-Wafai R, Selvaggi S, et al. Brush cytology of the biliary tract: retrospective study of 278 cases with histopathologic correlation. Diagn Cytopathol. 2002; 26: 273-7.
- Safwan M, Vij M, Govil S, Rela M. Well-Differentiated Neuroendocrine Tumour of the Extrahepatic Bile Duct: A Case Report with Review of Literature. J Gastrointest Cancer. 2016; 47: 93-9.
- Goodman ZD, Albores-Saavedra J, Lundblad DM. Somatostatinoma of the cystic duct. Cancer. 1984; 53: 498-502.
- Mandujano-Vera G, Angeles-Angeles A, de la Cruz-Hernández J, Sansores-Pérez M, Larriva-Sahd J. Gastrinoma of the common bile duct: immunohistochemical and ultrastructural study of a case. J Clin Gastroenterol. 1995; 20: 321-4.
- Hao L, Friedman AL, Navarro VJ, West B, Robert ME. Carcinoid tumor of the common bile duct producing gastrin and serotonin. J Clin Gastroenterol. 1996; 23: 63-5.
- Martignoni ME, Friess H, Lübke D, Uhl W, Maurer C, Müller M, et al. Study of a primary gastrinoma in the common hepatic duct - a case report. Digestion. 1999; 60: 187-90.
- Nesi G, Lombardi A, Batignani G, Ficari F, Rubio CA, Tonelli F. Well-differentiated endocrine tumor of the distal common bile duct: A case study and literature review. Virchows Arch. 2006; 449: 104-11.
- Price TN, Thompson GB, Lewis JT, Lloyd RV, Young WF. ZollingerEllison syndrome due to primary gastrinoma of the extrahepatic biliary tree: Three case reports and review of literature. Endocr Pract. 2009; 15: 737-49.
- Little JM, Gibson AA, Kay AW. Primary common bile-duct carcinoid. Br J Surg. 1968; 55: 147-9.
- Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020; 76: 182-8.
- Gusani NJ, Marsh JW, Nalesnik MA, Tublin ME, Gamblin TC. Carcinoid of the extra-hepatic bile duct: a case report with longterm follow-up and review of literature. Am Surg. 2008; 74: 87- 90.
- Takahashi K, Sasaki R, Oshiro Y, Fukunaga K, Oda T, Ohkohchi N. Well-differentiated endocrine carcinoma originating from the bile duct in association with a congenital choledochal cyst. Int Surg. 2012; 97: 315-20.
- Klimstra DS, Modlin IR, Adsay NV, Chetty R, Deshpande V, et al. Pathology reporting of neuroendocrine tumors: application of the Delphic consensus process to the development of a minimum pathology data set. Am J Surg Pathol. 2010; 34: 300-13.
- Rindi G, Klimstra DS, Abedi-Ardekani B, Asa SL, Bosman FT, et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod Pathol. 2018; 31: 1770-86.
- Vinik AI, Silva MP, Woltering EA, Woltering G, Go VL, et al. Biochemical testing for neuroendocrine tumors. Pancreas. 2009; 38: 876-89.
- Angela Prestifilippo GB, Maria Paola Vitale and Dario Giuffrida (2012). Chromogranin A and, Neuroendocrine Tumors NT, Dr. Anthony Lowell (Ed.), ISBN: 978-953-51-0653-1.
- El Rassi ZS, Mohsine RM, Berger F, Thierry P, Partensky CC. Endocrine tumors of the extrahepatic bile ducts. Pathological and clinical aspects, surgical management and outcome. Hepatogastroenterology. 2004; 51: 1295-300.
- Hong N, Kim HJ, Byun JH, Kim SY, Kim KW, Kim JH, et al. Neuroendocrine neoplasms of the extrahepatic bile duct: radiologic and clinical characteristics. Abdom Imaging. 2015; 40: 181-91.
- Choi J, Lee KJ, Kim SH, Cho MY. Preoperative diagnosis of welldifferentiated neuroendocrine tumor in common hepatic duct by brush cytology: A case report. Diagn Cytopathol. 2019; 47: 720-4.
- Abe T, Nirei A, Suzuki N, Todate Y, Azami A, et al. Neuroendocrine tumor of the extrahepatic bile duct: A case report. Int J Surg Case Rep. 2017; 40: 6-9.
- Michalopoulos N, Papavramidis TS, Karayannopoulou G, Pliakos I, Papavramidis ST, Kanellos I. Neuroendocrine tumors of extrahepatic biliary tract. Pathol Oncol Res. 2014; 20: 765-75.
- Elias E, Hamlyn AN, Jain S, Long RG, Summerfield JA, Dick R, et al. A randomized trial of percutaneous transhepatic cholangiography with the Chiba needle versus endoscopic retrograde cholangiography for bile duct visualization in jaundice. Gastroenterology. 1976; 71: 439-43.
- Okuda K, Kubo Y, Okazaki N, Arishima T, Hashimoto M. Clinical aspects of intrahepatic bile duct carcinoma including hilar carcinoma: A study of 57 autopsy-proven cases. Cancer. 1977; 39: 232-46.
- Alexander F, Rossi RL, O’Bryan M, Khettry U, Braasch JW, Watkins E. Biliary carcinoma. A review of 109 cases. Am J Surg. 1984; 147: 503-9.
- Shah MH, Goldner WS, Halfdanarson TR, Bergsland E, Berlin JD, Halperin D, et al. NCCN Guidelines Insights: Neuroendocrine and Adrenal Tumors, Version 2.2018. J Natl Compr Canc Netw. 2018; 16: 693-702.
- Alexandraki KI, Kaltsas G. Gastroenteropancreatic neuroendocrine tumors: new insights in the diagnosis and therapy. Endocrine. 2012; 41: 40-52.
- Kopelman D, Schein M, Kerner H, Bahuss H, Hashmonai M. Carcinoid tumor of the common bile duct. HPB Surg. 1996; 10: 41-3.
- Shah MH, Goldner WS, Halfdanarson TR, Bergsland E, Berlin JD, Halperin D, et al. NCCN Guidelines Insights: Neuroendocrine and Adrenal Tumors, Version 2.2018. J Natl Compr Canc Netw. 2018; 16: 693-702.
- PILZ E. [On carcinoid of the bile duct]. Zentralbl Chir. 1961; 86: 1588-90.
- Schwesinger G. Das Karzinoid der Gallenwege [Carcinoid tumor of the bile ducts]. Z Arztl Fortbild (Jena). 1978; 72: 796-8.
- Gerlock AJ Jr, Muhletaler CA. Primary common bile duct carcinoid. Gastrointest Radiol. 1979; 4: 263-4.
- Vitaux J, Salmon RJ, Languille O, Buffet C, Martin E, Chaput JC. Carcinoid tumor of the common bile duct. Am J Gastroenterol. 1981; 76: 360-2.
- Jutte DL, Bell RH Jr, Penn I, Powers J, Kolinjivadi J. Carcinoid tumor of the biliary system. Case report and literature review. Dig Dis Sci. 1987; 32: 763-9.
- Gastinger I, Schütze U, Beetz G, Lippert H. Verschlussikterus durch ein Karzinoid des Ductus hepatocholedochus [Obstructive jaundice caused by a carcinoid tumor of the hepatocholedochal duct]. Zentralbl Chir. 1987; 112: 1170-5.
- Reinhardt D, Thiele H, Weber JC, Hofmann WJ. Carcinoid des Ductus choledochus. Seltene Ursache eines Verschlussikterus [Carcinoid of the ductus choledochus. A rare cause of obstructive jaundice]. Chirurg. 1988; 59: 683-7.
- Fujita N, Mochizuki F, Lee S, Satoh K, Kobayashi G, Yano A, Shimoda T. Carcinoid tumor of the bile duct: Case report. Gastrointest Radiol. 1989; 14: 151-4.
- Chittal SM, Ra PM. Carcinoid of the cystic duct. Histopathology. 1989; 15: 643-6.
- van der Wal AC, Van Leeuwen DJ, Walford N. Small cell neuroendocrine (oat cell) tumour of the common bile duct. Histopathology. 1990; 16: 398-400.
- Bumin C, Ormeci N, Dolapçi M, Güngör S. Carcinoid tumor of the biliary duct. Int Surg. 1990; 75: 262-4.
- Fellows IW, Leach IH, Smith PG, Toghill PJ, Doran J. Carcinoid tumour of the common bile duct--a novel complication of von Hippel-Lindau syndrome. Gut. 1990; 31: 728-9.
- Brown WM 3rd, Henderson JM, Kennedy JC. Carcinoid tumor of the bile duct. A case report and literature review. Am Surg. 1990; 56: 343-6.
- Angeles-Angeles A, Quintanilla-Martínez L, Larriva-Sahd J. Primary carcinoid of the common bile duct. Immunohistochemical characterization of a case and review of the literature. Am J Clin Pathol. 1991; 96: 341-4.
- Newman K, Vates T, Duffy L, Anderson K. Pancreatoduodenectomy with preservation of the stomach and pylorus: A safe and effective alternative in children. J Pediatr Surg. 1992; 27: 1334-5.
- Rugge M, Sonego F, Militello C, Guido M, Ninfo V. Primary carcinoid tumor of the cystic and common bile ducts. Am J Surg Pathol. 1992; 16: 802-7.
- Ueyama T, Ding J, Hashimoto H, Tsuneyoshi M, Enjoji M. Carcinoid tumor arising in the wall of a congenital bile duct cyst. Arch Pathol Lab Med. 1992; 116: 291-3.
- Gembala RB, Arsuaga JE, Friedman AC, Radecki PD, Ball DS, Hartman GG, Rabin L, Caroline DF. Carcinoid of the intrahepatic ducts. Abdom Imaging. 1993; 18: 242-4.
- Sankary HN, Foster P, Frye E, Williams JW. Carcinoid tumors of the extrahepatic bile duct: an unusual cause of bile duct obstruction. Liver Transpl Surg. 1995; 1: 122-3.
- Belli G, Rotondano G, D'Agostino A, Marano I. Primary extrahepatic bile duct carcinoids. HPB Surg. 1996; 9: 101-5.
- Meyer CN, Geerdsen J, Christensen N. Limited surgical excision of a localized carcinoid tumour of the cystic duct. Dig Surg. 1997; 14: 423–425.
- Shah IA, Schlageter MO, Wong SX, Gani OS. Carcinoid tumor of the cystic duct. Dig Surg. 1998; 15: 372-3.
- Oikawa I, Hirata K, Katsuramaki T, Mukaiya M, Sasaki K, Satoh M. Neuroendocrine carcinoma of the extrahepatic biliary tract with positive immunostaining for gastrin-releasing peptide: Report of a case. Surg Today. 1998; 28: 1192-5.
- Bembenek A, Lotterer E, Machens A, Cario H, Krause U, Holzhausen HJ, Fleig WE, Dralle H. Neuroendocrine tumor of the common hepatic duct: a rare cause of extrahepatic jaundice in adolescence. Surgery. 1998; 123: 712-5.
- Ross AC, Hurley JB, Hay WB, Rusnak CH, Petrunia DM. Carcinoids of the common bile duct: a case report and literature review. Can J Surg. 1999; 42: 59-63.
- Perakath B, Chandran BS, Srivastava VM, Nair A, Sitaram V. Carcinoid tumor of common hepatic duct. Indian J Gastroenterol. 1999; 18: 127.
- Hermina M, Starling J, Warner TF. Carcinoid tumor of the cystic duct. Pathol Res Pract. 1999; 195: 707-9.
- Martignoni ME, Friess H, Lübke D, Uhl W, Maurer C, Müller M, Richard H, Reubi JC, Büchler MW. Study of a primary gastrinoma in the common hepatic duct - a case report. Digestion. 1999; 60: 187-90.
- Aronsky D, Z'graggen K, Stauffer E, Lange J, Klaiber C. Primary neuroendocrine tumors of the cystic duct. Digestion. 1999; 60: 493-6.
- Perakath B, Chandran BS, Srivastava VM, Nair A, Sitaram V. Carcinoid tumor of common hepatic duct. Indian J Gastroenterol. 1999; 18: 127.
- Juturi JV, Maghfoor I, Doll DC, Evans ML. A case of biliary carcinoid presenting with pancreatitis and obstructive jaundice. Am J Gastroenterol. 2000; 95: 2973-4.
- Maitra A, Krueger JE, Tascilar M, Offerhaus GJ, Angeles-Angeles A, Klimstra DS, Hruban RH, Albores-Saavedra J. Carcinoid tumors of the extrahepatic bile ducts: a study of seven cases. Am J Surg Pathol. 2000; 24: 1501-10.
- Turrión VS, Salas C, Alvira LG, Jimenez M, Lucena JL, Ardaiz J. Carcinoid tumour of the common bile duct: an exceptional indication for liver transplantation. Transplant Proc. 2002; 34: 264- 5.
- Pawlik TM, Shah S, Eckhauser FE. Carcinoid tumor of the biliary tract: treating a rare cause of bile duct obstruction. Am Surg. 2003; 69: 98-101.
- Podnos YD, Jimenez JC, Zainabadi K, Ji P, Cooke J, Busuttil RW, Imagawa DK. Carcinoid tumors of the common bile duct: Report of two cases. Surg Today. 2003; 33: 553-5.
- Volpe CM, Pryor JP, Caty M, Doerr RJ. An adolescent with bile duct carcinoid tumor. Med Pediatr Oncol. 2003; 40: 137-8.
- El Rassi ZS, Mohsine RM, Berger F, Thierry P, Partensky CC. Endocrine tumors of the extrahepatic bile ducts. Pathological and clinical aspects, surgical management and outcome. Hepatogastroenterology. 2004; 51: 1295-300.
- Menezes AA, Diver AJ, McCance D, Diamond T. Carcinoid tumour of the extrahepatic bile duct--report of a case and literature review. Ulster Med J. 2004; 73: 59-62.
- Ligato S, Furmaga W, Cartun RW, Hull D, Tsongalis GJ. Primary carcinoid tumor of the common hepatic duct: A rare case with immunohistochemical and molecular findings. Oncol Rep. 2005; 13: 543-6.
- Pithawala M, Mittal G, Prabhu RY, Kantharia CV, Joshi A, Supe A. Carcinoid tumor of bile duct. Indian J Gastroenterol. 2005; 24: 262-3.
- Hubert C, Sempoux C, Berquin A, Deprez P, Jamar F, Gigot JF. Bile duct carcinoid tumors: an uncommon disease but with a good prognosis? Hepatogastroenterology. 2005; 52: 1042-7.
- Tzimas GN, Vali K, Deschênes M, Marcus VA, Barkun JS, Tchervenkov JI, Metrakos PP. Liver transplantation for metastases from a bile duct carcinoid. HPB. 2006; 8: 67-8.
- Kim DH, Song MH, Kim DH. Malignant carcinoid tumor of the common bile duct: report of a case. Surg Today. 2006; 36: 485-9.
- Caglikulekci M, Dirlik M, Aydin O, Ozer C, Colak T, Dag A, Canbaz H, Aydin S. Carcinoid tmour of the common bile duct: report of a case and a review of the literature. Acta Chir Belg. 2006; 106: 112-5.
- John BM, Song MH, Park YS, Jo YJ, Kim SH, Lee HH, Kim SK, Jung SH, Kim DH, Kim DH. [A case of carcinoid tumor of the common bile duct]. Korean J Gastroenterol. 2006; 47: 320-3.
- Honda H, Hayashi S, Sekiguchi Y, Tsukadaira T, Nakamura K. Nihon Shokakibyo Gakkai Zasshi. 2006; 103: 1169-75.
- Ferrone CR, Tang LH, D'Angelica M, DeMatteo RP, Blumgart LH, Klimstra DS, Jarnagin WR. Extrahepatic bile duct carcinoid tumors: malignant biliary obstruction with a good prognosis. J Am Coll Surg. 2007; 205: 357-61.
- Sethi H, Madanur M, Srinivasan P, Portmann B, Heaton N, Rela M. Non-functioning well-differentiated neuroendocrine tumor of the extrahepatic bile duct: an unusual suspect? Hepatobiliary Pancreat Dis Int. 2007; 6: 549-52.
- Todoroki T, Sano T, Yamada S, Hirahara N, Toda N, Tsukada K, Motojima R, Motojima T. Clear cell carcinoid tumor of the distal common bile duct. World J Surg Oncol. 2007; 5: 6.
- Colombo F, Carrara B, Rosato S, Rück F, Simonetti A, Soccio M, Taverniti G, Zeppieri MC. Carcinoide delle vie biliari. Chir Ital. 2007; 59: 405-10.
- Stavridi F, Chong H, Chan S, Goldsmith C, Reddy M, Glees J, Benepal T. Neuroendocrine tumour of the cystic duct: a case report and literature review. J Gastrointest Cancer. 2007; 38: 32-3.
- Nafidi O, Nguyen BN, Roy A. Carcinoid tumor of the common bile duct: A rare complication of von Hippel-Lindau syndrome. World J Gastroenterol. 2008; 14: 1299-301.
- Gusani NJ, Marsh JW, Nalesnik MA, Tublin ME, Gamblin TC. Carcinoid of the extra-hepatic bile duct: a case report with longterm follow-up and review of literature. Am Surg. 2008; 74: 87- 90.
- Felekouras E, Petrou A, Bramis K, Prassas E, Papaconstantinou I, Dimitriou N, Pazaiti A, Tsigris C, Giannopoulos A. Malignant carcinoid tumor of the cystic duct: a rare cause of bile duct obstruction. Hepatobiliary Pancreat Dis Int. 2009; 8: 640-6.
- Tonnhofer U, Balassy C, Reck CA, Koller A, Horcher E. Neuroendocrine tumor of the common hepatic duct, mimicking a choledochal cyst in a 6-year-old child. J Pediatr Surg. 2009; 44: E23-5.
- Squillaci S, Marchione R, Piccolomini M, Colombo F, Bucci F, Bruno M, Bisceglia M. Well-differentiated neuroendocrine carcinoma (malignant carcinoid) of the extrahepatic biliary tract: report of two cases and literature review. APMIS. 2010; 118: 543-56.
- Zhan J, Bao G, Hu X, Gao W, Ruo X, Gong J, Zhu Q, Liu Y. Carcinoid tumor of the common bile duct in children: a case report. J Pediatr Surg. 2010; 45: 2061-3.
- Cappell MS, Killeen TC, Jury R. Common bile duct carcinoid mimicking the clinical, EUS, and ERCP findings of cholangiocarcinoma: a rare but potentially curable cause of obstructive jaundice. Clin Gastroenterol Hepatol. 2011; 9: e112-3.
- Bhalla P, Powle V, Shah RC, Jagannath P. Neuroendocrine tumor of common hepatic duct. Indian J Gastroenterol. 2012; 31: 144- 6.
- Linder R, Dorfman T, Ben-Ishay O, Kakiashvili E, Velodavsky E, Kluger Y. Mixed neuroendocrine tumor of the common bile duct. JOP. 2013; 14: 71-3.
- Yasuda T, Imai G, Takemoto M, Yamasaki M, Ishikawa H, Kitano M, Nakai T, Takeyama Y. Carcinoid tumor of the extrahepatic bile duct: Report of a case. Clin J Gastroenterol. 2013; 6: 177-87.
- De Luca L, Tommasoni S, de Leone A, Bianchi ML, de Nictolis M, Baroncini D. Neuroendocrine tumor of the extrahepatic bile duct: A tumor in an unusual site visualized by cholangioscopy. Endoscopy. 2013; E338-9.
- Navas-Cuéllar JA, Álamo-Martínez JM, Bernal-Bellido C, MartínPérez B, Marín-Gómez LM, Suárez-Artacho G, Serrano-DíezCanedo J, Gómez-Bravo MÁ, Padillo-Ruiz J. Neuroendocrine carcinoma of the common bile duct. Rev Esp Enferm Dig. 2014; 106: 558-60.
- Yalav O, Ülkü A, Demiryürek H, Doran F. A rare cause of bile duct obstruction in adolescence: Neuroendocrine tumor. Turk J Gastroenterol. 2014; 25: 311-2.
- Park SB, Moon SB, Ryu YJ, Hong J, Kim YH, Chae GB, Hong SK. Primary large cell neuroendocrine carcinoma in the common bile duct: First Asian case report. World J Gastroenterol. 2014; 20: 18048-52.
- Hosoda K, Kobayashi A, Shimizu A, Kitagawa N, Ito T, Yamada A, Miyagawa S. Neuroendocrine tumor of the common bile duct. Surgery. 2016; 160: 525-6.
- Fernández-Cruz L, Pelegrina A. Cirugía del gastrinoma: Resultados inmediatos y a largo plazo. Cir Esp. 2015; 93: 390-5.
- Banerjee JK, Saranga Bharathi R, Shrivastava S, Ranjan P. Neuroendocrine tumor of distal bile duct. Med J Armed Forces India. 2016; 72: S101-S104.
- Khan FA, Stevens-Chase A, Chaudhry R, Hashmi A, Edelman D, Weaver D. Extrahepatic biliary obstrution secondary to neuroendocrine tumor of the common hepatic duct. Int J Surg Case Rep. 2017; 30: 46-49.
- Murakami M, Katayama K, Kato S, Fujimoto D, Morikawa M, Koneri K, Hirono Y, Goi T. Large-cell neuroendocrine carcinoma of the common bile duct: A case report and a review of literature. Surg Case Rep. 2016; 2: 141.
- Costin AI, Păun I, Păun M, Constantin VD, Vârcuş F. Primary neuroendocrine tumors - an extremely rare cause of obstruction of extrahepatic bile ducts: a case report. Rom J Morphol Embryol. 2017; 58: 641-644.
- Hoepfner L, White JA. Primary extrahepatic bile duct neuroendocrine tumor with obstructive jaundice masquerading as a Klatskin tumor. J Surg Case Rep. 2017; 2017:104.
- Zhang L, Yang Z, Chen Q, Li M, Zhu X, Wan D, Xie H, Zheng S. Mixed adenoendocrine carcinoma in the extrahepatic biliary tract: A case report and literature review. Oncol Lett. 2019; 18: 1585-1596.
- Choi J, Lee KJ, Kim SH, Cho MY. Preoperative diagnosis of welldifferentiated neuroendocrine tumor in common hepatic duct by brush cytology: A case report. Diagn Cytopathol. 2019; 47: 720-724.
- Umezaki N, Hashimoto D, Yamashita YI, Nakagawa S, Nakao Y, Itoyama R, Yusa T, Yamao T, Okabe H, Imai K, Hayashi H, Chikamoto A, Baba H. Neuroendocrine Tumor of the Hilar Bile Duct. Anticancer Res. 2019; 39: 903-907.
- Park JY, Jeon TJ. Large Cell Neuroendocrine Carcinoma of the Extrahepatic Bile Duct. Korean J Gastroenterol. 2018; 72: 318-321.