
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Woman with dyspnea and history of systemic lupus erythematosus
Nicolas Kahl1*; Sukhdeep Singh1; Jessica Oswald1,2
1 Department of Emergency Medicine, University of California San Diego, USA.
2 Center for Pain Medicine, University of California San Diego, USA.
*Corresponding Author: Nicolas Kahl
Department of Emergency Medicine, University of
California San Diego, USA.
Email: nmkahl@health.ucsd.edu
Received : July 09, 2021
Accepted : Aug 10, 2021
Published : Aug 14, 2021
Archived : www.jcimcr.org
Copyright : © Kahl N (2021).
Citation: Kahl N, Singh S, Oswald J. Woman with dyspnea and history of systemic lupus erythematosus. J Clin Images Med Case Rep. 2021; 2(4): 1265.
Introduction
32-year-old woman with history of pleurisy and systemic lupus erythematosus presented to the emergency department with shortness of breath and pleuritic chest pain, acutely worse over one day after a six hour flight three days prior. She became dyspneic walking from her hotel bed to the bathroom. She endorsed 3 weeks of right lower leg cramping. She denied history of blood clots. She appeared tachypneic and speaking in short phrases upon arrival. A bedside ultrasound was performed, see Figures. Vitals: T: 98.3 F, HR: 130, BP: 142/88, RR: 24, oxygen saturation 97% on room air.
Diagnosis
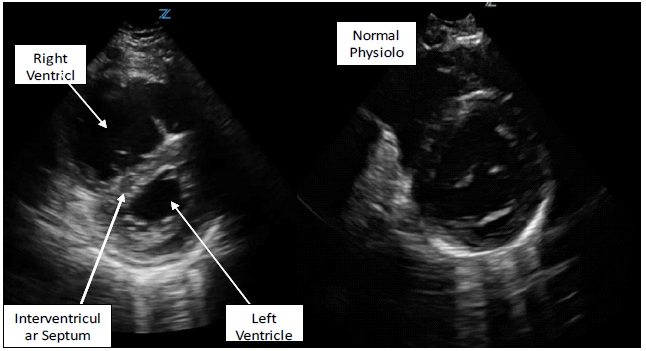
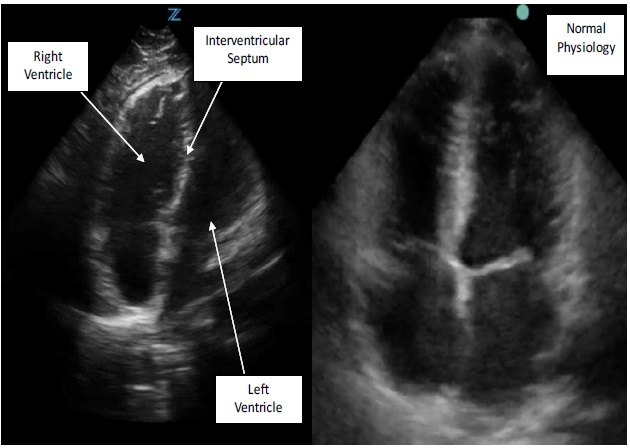
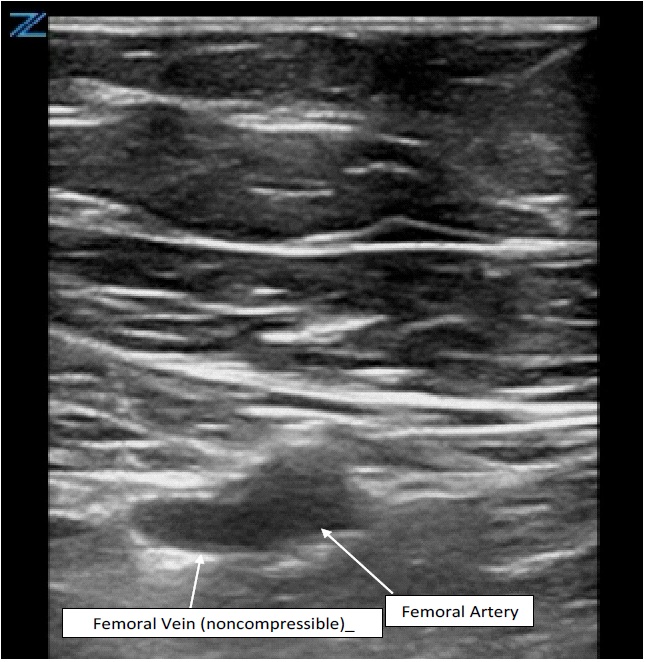
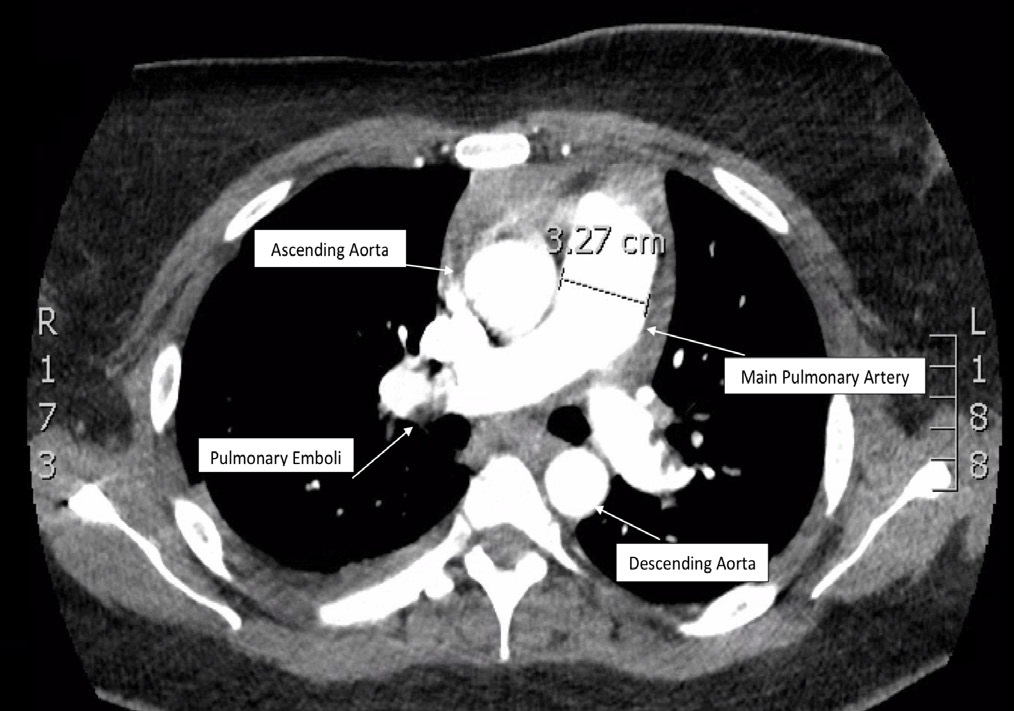
Submassive Pulmonary Embolism. Apical 4 chamber view of the heart on ultrasound demonstrates right ventricular dilation with bowing of the interventricular septum into the left ventricle. Parasternal short view of the heart illustrates “D sign” with right ventricular dilation and flattening of the septum indicating decreased left ventricular systolic function. Both views suggest right heart strain in the setting of likely Pulmonary Embolism (PE). The right lower extremity showed a noncompressible right femoral vein, indicating Deep Vein Thrombosis (DVT) as the likely source. CT chest angiogram confirmed diagnosis of PE extending into all 5 lobes and 3.2 cm dilation of the pulmonary artery. The patient was admitted to the ICU, and half dose TPA was given.
Point-of-care transthoracic cardiac ultrasound in the emergency department is an effective tool to promptly diagnose acute pulmonary embolism with right heart strain, and rapidly guide management [4,5]. Identification of right ventricular dilation on point-of-care echocardiography for the diagnosis of PE is highly specific [1]. When cardiac and lower extremity ultrasound are combined, the sensitivity and specificity are above 90% [3]. Patients who present normotensive but have signs of cardiac dysfunction secondary to a PE are classified as submassive, and thrombolytic therapy should be considered to reduce long term risk of pulmonary hypertension [2,6].
References
- Dresden S, et al. Right Ventricular dilatation on bedside echocardiography performed by emergency physicians aids in diagnosis of pulmonary embolism. Ann Emerg Med; 2014; 63: 16-24.
- Malik Sonika et al. Advanced Management Options for Massive and Submassive Pulmonary Embolism. USC US Cardiology Review. 2016.
- Nazerian P, et al. Diagnostic accuracy of focused cardiac and venous ultrasound examinations in patients with shock and suspected pulmonary embolism. Intern Emerg Med. 2018; 13: 567- 574.
- Fields JM, et al. Transthoracic Echocardiography for Diagnosing Pulmonary Embolism: A Systematic Review and Meta-Analysis. J Am Soc Echocardiogr. 2017.
- Kahl N, et al. Point-of-care Ultrasound Diagnosis of Pulmonary Embolism with Thrombus in Transit.Clin Pract Cases Emerg Med. 2019; 3: 11–12.
- Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am J Cardiol. 2013; 111: 273-277.