
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A 7 cm trachea resection and carina reconstruction due to a rare tracheal carina tumor
Bohao Liu1,2; Kun Fan1; Jizhao Wang1; Hongyi Wang1; Heng Zhao1,2; Yixing Li1,2; Zhiyu Wang1,2; Yanpeng Zhang1,2; Junke Fu1; Jia Zhang1; Weiwei Wu3*; Guangjian Zhang1*
1 Department of Thoracic Surgery, First Affiliated Hospital, Xi’an Jiaotong University, Xi’an 710061, China.
2 Health Science Center, Xi’an Jiaotong University, Xi’an710061, China.
3 Interdisciplinary Research Center of Smart Sensors, Academy of Advanced Interdisciplinary Research, Xidian University, Xi’an, 710061, China.
*Corresponding Author: Zhang Guangjian11 & Weiwei Wu2
1 Department of Thoracic Surgery, First Affiliated
Hospital, Xi’an Jiaotong University, Xi’an 710061,
China. 2 Interdisciplinary Research Center of Smart
Sensors, Academy of Advanced Interdisciplinary
Research, Xidian University, Xi’an, 710061, China.
Email: michael8039@163.com; wwwu@xidian.edu.cn
Received : July 07, 2021
Accepted : Aug 10, 2021
Published : Aug 14, 2021
Archived : www.jcimcr.org
Copyright : © Guangjian Z & Wu W (2021).
Abstract
Background: Tracheal Squamous Cell Carcinoma (SCC) is a rare primary tumour. Currently, surgery is the main treatment, but it becomes the biggest obstacle to surgery when the tumour invades the trachea for more than 6 cm.
Case presentation: A 56-year-old Asian man presented with expectoration and asthma as his initial symptoms. Because of the particularity of tumour location and volume, we removed the 7 cm bronchus and performed carinau reconstruction.
Conclusion: How to treat the rare tumours at tracheal carina is a valuable and rare example that could be reference in many centres.
Keywords: carina reconstruction; tracheal resection; SCC.
Citation: Zhang G, Wu W. Liu B, Fan K, Wang J, et al. A 7 cm trachea resection and carina reconstruction due to a rare tracheal carina tumor. J Clin Images Med Case Rep. 2021; 2(4): 1267.
Introduction
Primary tracheal tumor is a rare tumour occurring below the cricoid cartilage to the level of the carina, which originates from epithelial, salivary gland, interstitial and other structures. The lack of specific manifestations in the early stage is prone to misdiagnosis, and the primary tracheal tumour is very rare in surgery, accounting for about 0.1 % of all tumours [1]. Primary tracheal squamous cell carcinoma treatment mainly includes surgical tracheal resection, various endoscopic resection, tracheal stent and chemoradiotherapy. However, only surgical resection can cure all benign and most malignant tumours. If a long bronchus needs to be removed, it will cause difficulties in tracheal anastomosis. If the tumour involves a protuberance, it needs to reconstruct the protuberance, but the reconstruction of the tracheal carina is still a significant challenge in thoracic surgery. Tracheal carina reconstruction surgery requires formulating a precise preoperative surgical plan, and the tacit cooperation between the anaesthesia team and the surgical team during the operation, which makes the operation very difficult. The risk and difficulty of surgery will also increase as the size of the tumour increases. The larger the tumour, the more trachea needs to be removed, and the more difficult it is to suture the remaining trachea. Here, we report the first case of resection and reconstruction of tumour in giant tracheal protuberance in our center.
Case report
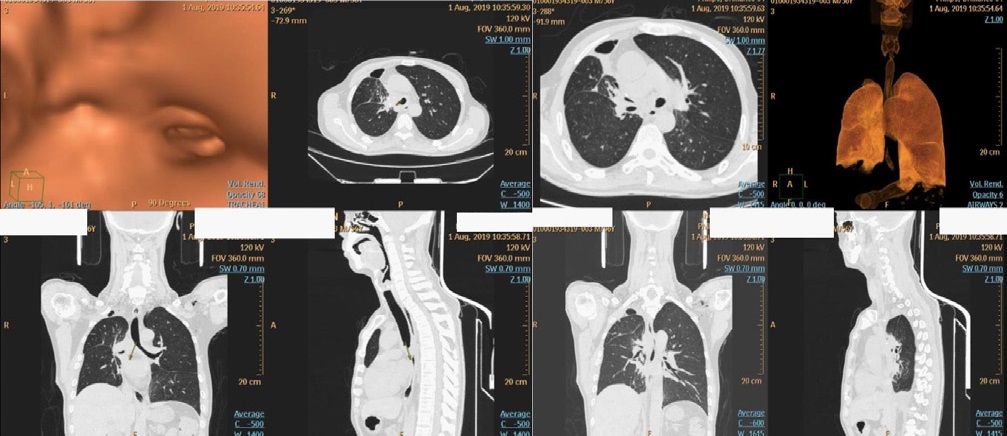
A 56-year-old male was admitted to hospital for “expectoration for 1 year, aggravated with asthma for 4 months”. Bronchoscopy showed that the carina was deformed, with a large number of caseous lesions attached, and the left and right central bronchial openings were significantly narrowed (Figure 1). Chest CT and three-dimensional reconstruction showed that the left and right main bronchial bifurcations of the lower trachea were unevenly thickened, and the corresponding segment of the local lumen was narrowed (Figure 2). Therefore, we decided to perform thoracoscopic assisted thoracotomy for tracheal tumor resection, sleeve resection of the upper lobe of the right lung, and carina resection and reconstruction.

After general anaesthesia, the patient was lying on the left side, and the Trocar was inserted into the mid-axillary line of the seventh intercostal space, scapula line and the fourth intercostal opening of the left side, and then freed the lower lung ligament and mediastinal pleura. At last, an incision was sutured. The patient was changed to the right lateral position, and a 15 cm incision was made through the fifth intercostal space, and the chest was opened for exploration. The lower pulmonary ligament and the right upper lobe bronchus of mediastinal pleura were dissociated. The tumour was located at 2 cm above the carina, extending nearly 1 cm into the right central bronchial orifice and 0.5 cm into the left main bronchial orifice. Then the tumour and its invading bronchi were excised. From the junction of the membrane part and cartilage part, 2/3 of the lower trachea and left main branch bronchus were sutured continuously, and then the lower trachea was sutured continuously with the residual end of the right middle bronchus, and the mediastinal pleura was embedded and sutured on the surface of the anastomosis. During the operation, the tubular tissue of ‘Tracheal Tumour’, with a length of 7 cm, a diameter of 2–2.5 cm, and a lumen, was excised and opened to reveal a protuberant mass (Fig. 3A), with a volume of 4 cm × 2 cm × 1.5 cm, and invasion of the entire tracheal layer. Pathological showed: moderately differentiated squamous cells (Figure 3B). A lymph node biopsy was also sent for immunohistochemical markers indicating no cancer metastasis.
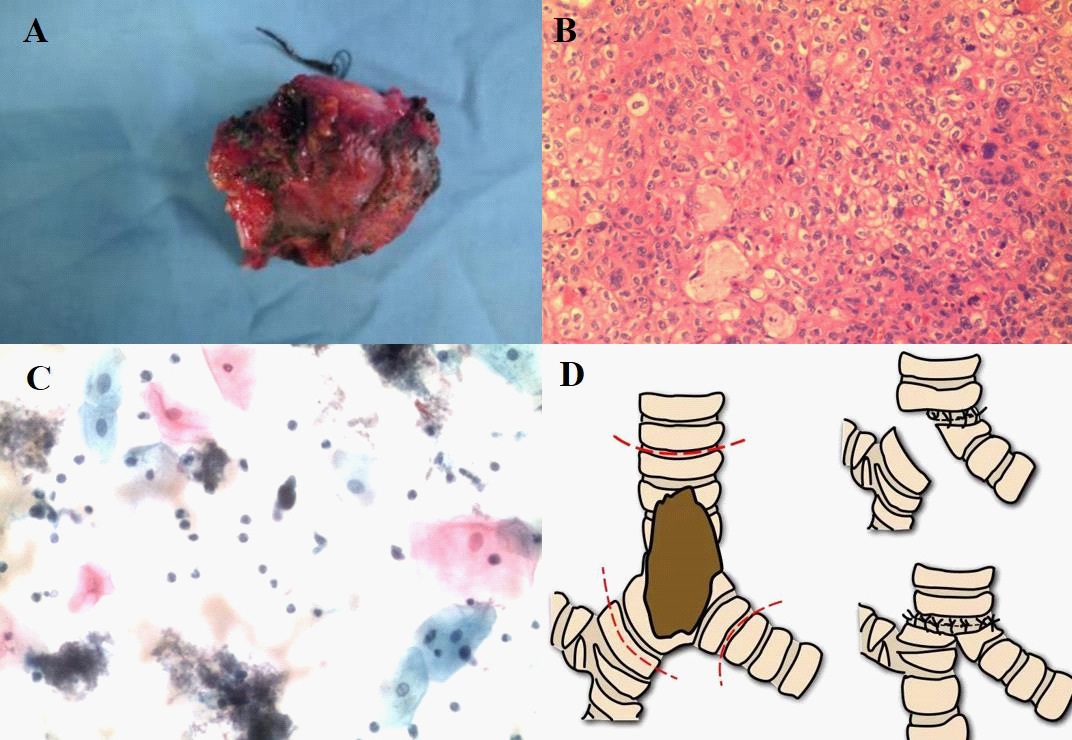
Patients were discharged from the hospital 15 days after operation without any complications. After 3 months of follow-up, no tumour recurrence or distant metastasis was found (Figure 3C).
Discussion
Primary Squamous Cell Carcinoma of the trachea (SCC) often occurs in the middle of the trachea, which is more common in men [2] and is closely related to smoking. Most of the tumours grow in the lobar and segmental bronchi close to the hilum of the lung, and tend to grow into the lumen.
Primary tracheal squamous cell carcinoma treatment mainly includes surgical tracheal resection, various endoscopic resection, tracheal stent and chemoradiotherapy. The choice of surgical resection depends on the location and size of the tumour. For the site located in the tracheal carina, if the tumour is large, it will block the bilateral airway, causing respiratory dysfunction and endanger life, requiring emergency surgical treatment.
Only 23-45% of primary tracheal tumours can be accurately diagnosed by chest CT. F [3], Besides, sputum smear can be used for diagnosing early carcinoma in situ. The development of new aerosol contrast agents and spectroscopic techniques can improve the sensitivity and specificity of virtual bronchoscopy [4]. Bronchoscopy can be selected for asthma, cough and expectoration. Bronchoscopy allows tissue samples to be taken from the tumour and adjacent trachea, and allows accurate determination of tumour size, tracheal length, and possible and necessary resection range [5]. Endotracheal ultrasonography provides further information for the deep infiltration of tumours [6]. For the significant stenosis of left and right central bronchial openings caused by large tumours reported in this paper, the relationship between tumor and surrounding tissues can be clarified combining the bronchoscopy and CT three-dimensional reconstruction technology, which provides an important reference for the formulation of surgical plan.
Tracheal tumour resection in the carina section is usually performed by the carina resection and reconstruction operation carried out by Belsey [7] in 1957. Grillo [8] reported personal experience of carina reconstruction in 1982 and pointed out that no matter what method was adopted, it was necessary to free the trachea sufficiently to increase the tracheal mobility to reduce the tracheal tension after anastomosis.
Later, more doctors reported the cases of tracheal reconstruction, but the reconstruction of tracheal carina is still a major challenge in thoracic surgery. The surgical technique and anastomosis reconstruction method are very complex, and the requirements for anesthesia technology and postoperative management are very high. Liu [9] Reported that 4 cases of tracheal tumor resection and carinoplasty had been successfully completed, and the 5-year survival rate was only 55.0 %. The incidence of postoperative complications is high, with a reported mortality rate of 13 – 31% [10]. Christina [11] counted all the patients undergoing carinal reconstruction in their center from 1997 to 2017, with a total of 45 cases. Among them, 28 patients have experienced varying degrees of complications. The 30 - days mortality rate was 6.8 %, and the 3 - month mortality rate was 7 %. By comparison, it was pointed out that mechanical and circulatory support, including CPB and ECMO could reduce the surgical risk and postoperative mortality. Jiangxin He team [12] has made some achievements in reconstructing carina, and successfully resected a tracheal adenoid cystic carcinoma with a size of about 2.1 cm × 1.2 cm in VAST and reconstructed carina. It is the first reported VATS tracheal carinal reconstruction using cross-vision ventilation in the world. Although there have been successful cases of tracheal carina reconstruction, no successful case of tracheal reconstruction with such a huge tumor at the carina has been reported by scholars.
We believe that for tumours with tracheal carina, whether thoracotomy or VAST, no matter what method is used to increase the degree of freedom of the trachea, the first thing to consider should be whether the tumor can be resected as completely as possible. Therefore, it is extremely important to predict the size of the tumour before operation. In this case, the upper edge of the tumor was located 2 cm above the carina, and the lower edge of the tumour completely invaded the left and right bronchus. Therefore, thoracoscopic-assisted thoracotomy was performed, and satisfactory results were achieved. Studies have shown that [11] if the resection length exceeds 6 cm, it is often difficult to anastomose during the operation or the anastomosis healing is poor after an operation. The length of the resected trachea of this patient is about 7 cm; the success in this patient’s reconstruction might shed light on how to deal with a large trachea tumour. In order to avoid the difficulty of anastomosis, we sufficient anastomosis was ensured by fully freeing the hilar, pulmonary vascular, lower pulmonary ligament and wrapping the anastomotic stoma through cervical flexion and pedicled pleural suture. Further release was achieved through pericardial dissection, and the pericardium was cut in a U shape around the lower side of the inferior pulmonary vein. The pulmonary hilum was further dissociated through the right pulmonary artery trunk and the upper segment of the pulmonary vein. And the anastomotic leakage was effectively prevented. Our center has found that bending the neck to about 20° could effectively reduce the anastomotic tension and minimize the discomfort caused by neck bending of patients. Mulliken and Grillo [8,13] showed in the cadaveric study that bending 15 – 35° could complement the tracheal length of 4.5 cm (equivalent to 7.2 tracheal rings) [13]. However, not the larger the bending angle is, the better the surgical effect will be. If the bending angle is too large, it will not reduce the incidence of anastomotic leakage, but will increase the pain of patients [14]. There are various ways of tracheal carina anastomosis. The most common one is to anastomose trachea end-to-end with left main bronchus, and then implant the right main trachea into one side of the trachea. Or lateral anastomosis of the inner wall of the left and right main bronchi is performed first, and then the trachea is anastomosed end to end to form a new bulge. The former method saves time and is less difficult. It is suitable for small tumors that only invade one side of the bronchus. The latter method is suitable for large tumors that invade both sides, and has certain requirements on suture. Because the patient ' s left and right bronchus were invaded, we adopted the second way (Figure 3D). During the suture, we first successively sutured two thirds of the left bronchus and the main bronchus, and then sutured from the side of the posterior tracheal wall. Finally, sutured the remaining one-third of the perimeter and right bronchus while maintaining ventilation. Squamous cell carcinoma is prone to metastasize, so lymph node dissection and resection of adjacent lung tissue are crucial. The tumor of this patient invaded 1 cm into the right main bronchus, and sleeve resection of the upper lobe of the right lung was performed. As a result, R0 resection was achieved, and the postoperative lung function was retained to the maximum extent. For complex tracheal carina tumor, a careful surgical plan should be formulated before operation. In the process of operation, tracheal intubation and surgical operation must be closely combined. Tracheal anastomosis and extubation should be carried out alternately. Oxygenation condition of patients should be closely monitored to ensure the safety of operation. CPB and ECMO can be used to assist operation when conditions perimit.
Conclusions
Tracheal tumours are rare and challenging for surgery. The traditional operation idea is that if the tumour is huge and the bronchus needs to be removed for more than 6 cm, the surgery can not be operated, because it will lead to inevitable anastomotic leakage. Here, we adopted a series of release methods to successfully reconstruct the carina of 7 cm trachea without complications, which reminds us that the surgical treatment of huge tracheal tumours is feasible, and provided a reference for areas that have never tried such operations.
Funding: The Key Research and Development Program of Shannxi (2020GXLH-Y-012). The Key Research and Development Program of Shannxi (2021SF-034).
References
- Paolo M. Primary tracheal tumours. Lancet Oncol. 2006; 1.
- Hoerbelt R, Padberg W. Primäre Trachealtumoren in Hals und Mediastinum. Der Chirurg. 2011; 82: 125-33.
- McCarthy MJ, Rosado-de-Christenson ML. Tumors of the trachea. J Thorac Imaging. 1995; 10: 180-98.
- Finkelstein SE, Summers RM, Nguyen DM, Schrump DS. Virtual bronchoscopy for evaluation of airway disease. Thorac Surg Clin. 2004; 14: 79-86.
- Wood DE. Bronchoscopic preparation for airway resection. Chest Surg Clin N Am. 2001; 11: 735-48.
- Kurimoto N, Murayama M, Yoshioka S, Nishisaka T, Inai K, Dohi K. Assessment of usefulness of endobronchial ultrasonography in determination of depth of tracheobronchial tumor invasion. Chest. 1999; 115: 1500-6.
- BELSEY R. Resection and reconstruction of the intrathoracic trachea. Br J Surg. 1950; 38: 200-5.
- Grillo HC. Carinal reconstruction. Ann Thorac Surg. 1982; 34: 356-73.
- Liu XY, Liu FY, Wang Z, Chen G. Management and surgical resection for tumors of the trachea and carina: experience with 32 patients. World J Surg. 2009; 33: 2593-8.
- Mathisen DJ. Carinal reconstruction: Techniques and problems. Semin Thorac Cardiovasc Surg. 1996; 8: 403-13.
- Costantino CL, Geller AD, Wright CD, Ott HC, Muniappan A, Mathisen DJ, et al. Carinal surgery: A single-institution experience spanning 2 decades. The Journal of Thoracic and Cardiovascular Surgery. 2019; 157: 2073-83.
- He J, Wang W, Li J, Yin W, Xu X, et al. Video-assisted thoracoscopic surgery tracheal resection and carinal reconstruction for tracheal adenoid cystic carcinoma. J Thorac Dis. 2016; 8: 198- 203.
- Mulliken JB, Grillo HC. The limits of tracheal resection with primary anastomosis: further anatomical studies in man. J Thorac Cardiovasc Surg. 1968; 55: 418-21.
- Heitmiller RF. Tracheal release maneuvers. Chest Surg Clin N Am. 1996; 6: 675-82.