
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Polycystic ovarian syndrome and pituitary macroadenoma a deadly combination with good outcome
Ansari Sumayya Shamim; Reena Jatin Wani; Hema Prakash Relwani*; Kruti Doshi
H.B.T. Medical College & Dr. R. N. Cooper Hospital, Juhu, Mumbai, India.
*Corresponding Author: Hema Prakash Relwani
H.B.T. Medical College & Dr. R. N. Cooper Hospital,
Juhu, Mumbai, India.
Email: bharwanihema22@gmail.com
Received : May 28, 2021
Accepted : Aug 11, 2021
Published : Aug 16, 2021
Archived : www.jcimcr.org
Copyright : © Relwani HP (2021).
Abstract
We are presenting here a case of polycystic ovarian syndrome, an endocrine disorder, afflicting 5-13% females of reproductive age, causing 70-80% infertility associated with pituitary macroadenoma i.e. size >10 mm & prolactin level >250 ng/mI.
PCOS has a higher relationship with metabolic disturbance and hypothalamic-pituitary-ovarian axis function disorder.
Prolactinoma is present in about 50% women with hyperprolactinemia and 33% present with galactorrhea.
Our patient was a 22 yrs nulligravida married since 3 yrs first presenting 5 yrs back with complaints of secondary amenorrhea with galactorrhea and infertility. On evaluation she was diagnosed as PCOS and pituitary macroadenoma on MRI. We medically treated her with tab. cabergoline in consultation with endocrinologist and neurosurgeons opinion. Being a compliant patient with regular follow up she conceived twice with good outcome and breastfed her babies on medical management only. Now she has 2 children (male child of 3 yrs and 1 month). Dilemma in management options will be discussed.
Summary: Inspite of having both Polycystic Ovarian Syndrome (PCOS) & PITUITARY MACROADENOMA, which warrant surgical management (major causes of Infertility) selected cases like ours can be managed medically successfully.
Citation: Shamim AS, Wani RJ, Relwani HP, Doshi K. Polycystic ovarian syndrome and pituitary macroadenoma a deadly combination with good outcome. J Clin Images Med Case Rep. 2021; 2(4): 1268.
Introduction
PCOS and hyperprolactinemia are the two most common etiologies of anovulation in women [1]. PCOS is recognised as the most common endocrine disorder of reproductive aged women around the world. Prolactinoma is present in about 50%women with hyperprolactinemia and 33% patient present with galactorrhea.
Case report
Our patient was 22 yrs nulligravida first presenting 5yrs back married since 3 yrs with oligomenorrhea followed by secondary amenorrhoea with galactorrhea & infertility came to hospital & got evaluated. On evaluation she was diagnosed on Ultrasonography (USG) as polycystic ovarian disease.
Her Sr. prolactin was >329 ng/ml. All other hormones Sr. TSH, FSH, LH are within normal limits. Then patient was advised to do MRI brain, on MRI 2.8 ×2.5 ×2.7 cm pituitary macroadenoma found with apoplexy, other anterior pituitary hormones are evaluated & found Within Normal Limits (WNL).
Though prolactinoma warrant surgery, after doing multidisciplinary approach to Endocrinologist, Gynaecologists and neurosurgeons, as patient keen to conceive decission of medical management taken. Patient started on Tab. cabergoline 0.5 mg twice weekly & Sr prolactin levels are monitored 3 monthly, Perimetry done. 3 monthly & MRI done yearly.
Years |
|
Treatment |
March 2016 |
2818 |
Twice weekly |
March 2017 |
83.6 |
Twice weekly |
March 2018 |
148.0 |
Twice weekly |
Feb 2019 |
11.0 |
Once in a week |
Aug 2020 |
32.1 |
Once in a week |
Dec 2020 |
13.98 |
Once in a week |


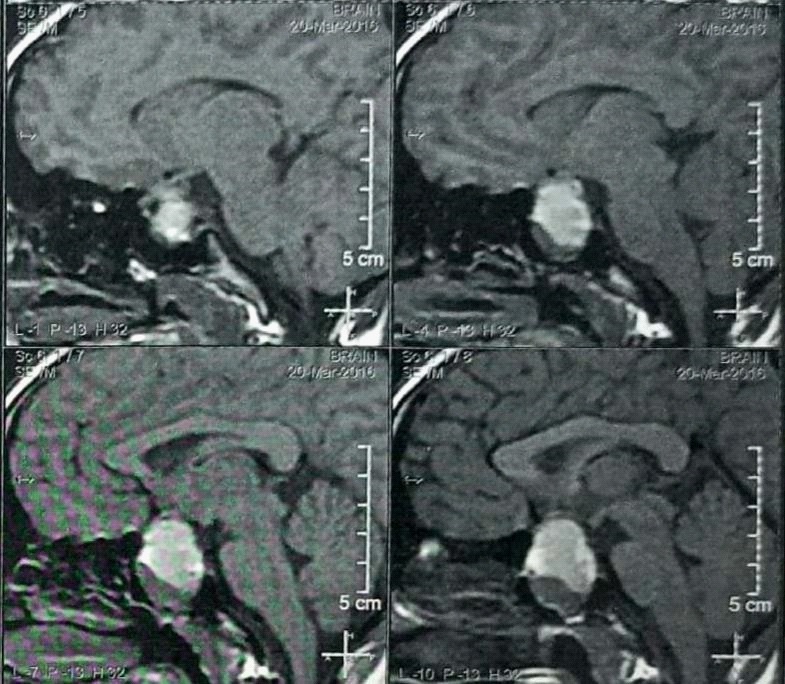
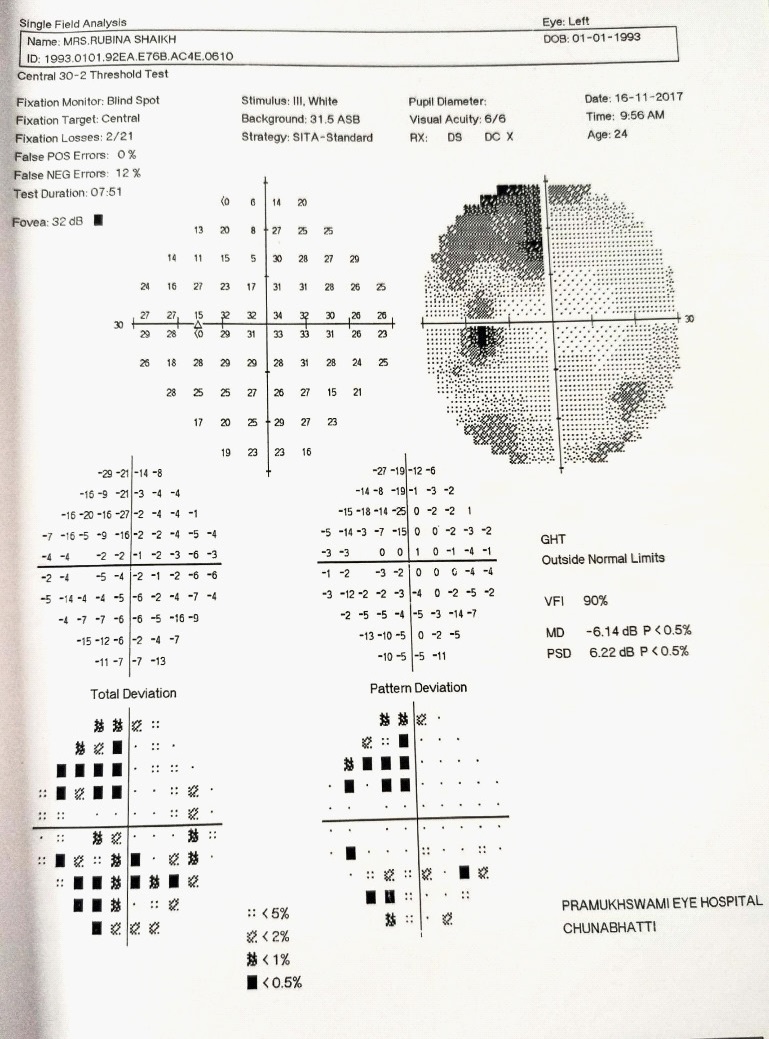
In 2017 on repeat MRI size was decreased slightly after that she was given Oral Contraceptive Pills (OCPs) for menstrual irregularities, patient conceived in NOV-2017 & cabergoline stopped for 2 month Sr Prolactin monitoring done which was increasing have re-started on T. cabergoline, Sr. Prolactin levels monitored 3 monthly & perimetry done in every trimester. She was given Tab. cabergoline throughout pregnancy & Lower Segment Caesarean Section (LSCS) was done at full term i/v/o poor Bishop's score. After delivery on endocrinologist advice T. cabergoline was continued & breastfeeding advised.
Patient continued on Tab. cabergoline once a week. She was then lost to follow up but in 2020 she conceived spontaneously and registered again with us. She was continued on Tab cabergoline weekly. Prolactin levels monitored 3 monthly and admitted near term. Emergency LSCS done i/v/o G2P1L1 with 38.2 weeks with previous LSCS in labour not willing for Trial Of Labour After Caesarean (TOLAC). Room in was done with exclusive breastfeeding and Tab Cabergoline continued she advised to repeat MRI brain after 6 weeks.
Discussion
PCOS has a higher relationship with metabolic disturbance and hypothalamic-pituitary-ovarian axis function disorder [2]. This syndrome results in hyperandrogenemia, hyperinsulinemia /insulin resistance, increase estrone, LH and FSH ratio imbalance, Infertility, cardiovascular disease, endometrial dysfunction, obesity [3]. PCOS women can have difficulty in conceiving. Prolactinoma is the most common type of hormone producing tumor. Prolactinoma (lactotroph adenoma) is one of the most common cause of prolactin excess [4]. Hyperprolactinemia is a typical condition producing reproductive dysfunction in both sexes, resulting in hypogonadism, Infertility and galactorrhea [4].
Prolactinoma is only tumour for which medical therapy has proven role. Surgery and radiotherapy are 2nd line of management [5].
Dopamine agonist Bromocriptine, Cabergoline, Pergolide mesylate, Lisuride, Quanagolide [5].
Cabergoline can be given once or twice a week with a starting dose of 0.25 mg twice a week. Titrate these based on prolactin level and tolerability [5].
Being a compliant patient with regular follow up she conceived twice with good outcome and breastfed her babies.
Now she has 2 children (male child of 3 yrs and 1 month).
Conclusion
Inspite of having both PCOS & Pituitary macroadenoma, which warrant surgical management (major causes of Infertility) selected cases like ours can be managed medically successfully.
References
- Patel S. Polycystic Ovary Syndrome (PCOS), an inflammatory, systemic, lifestyle endocrinopathy. J Steroid Biochem Mol Biol. 2018; 182: 27-36.
- Delcour C, Robin G, Young J, Dewailly D. PCOS and Hyperprolactinemia: What do we know in 2019?. Clin Med Insights Reprod Health. 2019; 13: 1179558119871921.
- Li Y, Chen C, Ma Y, Xiao J, Luo G, et al. Multi-system reproductive metabolic disorder: significance for the pathogenesis and therapy of polycystic ovary syndrome (PCOS). Life Sci. 2019; 228: 167-175.
- Capozzi A, Scambia G, Pontecorvi A, Lello S. Hyperprolactinemia: Pathophysiology and therapeutic approach. Gynecol Endocrinol. 2015; 31: 506-510.
- Speroff’s clinical gynaecologic endocrinology & Infertility, 9th edition.