
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Clinical case of preiser disease, bilateral femoral head and humeral head osteonecrosis associated with chronic corticosteroid therapy
Cunha R*; Verraest X; Martins P; Madureira R; Pereira A
Electrophysiology and Pacing Unit, Cardiology Service, Hospital de Santa Marta, Centro Hospitalar Universitario de Lisboa Cental, Lisbon, Portugal.
*Corresponding Author: Cunha R
Electrophysiology and Pacing Unit, Cardiology Service, Hospital de Santa Marta, Centro Hospitalar
Universitario de Lisboa Cental, Lisbon, Portugal.
Email: rui.al.cunha@gmail.com
Received : May 26, 2021
Accepted : Aug 11, 2021
Published : Aug 16, 2021
Archived : www.jcimcr.org
Copyright : © Cunha R (2021).
Abstract
Osteonecrosis is a pathologic process that is associated with numerous conditions and therapeutic interventions. Most commonly the hip is involved but almost any bone can develop osteonecrosis. It can occur in the femoral head, but also affect the femoral condyles, humeral heads, proximal tibia, vertebrae, and small bones of the hand and foot. The most frequent etiological factors are trauma, alcoholism, and chronic corticosteroid therapy; the latter causing the most devastating form of osteonecrosis. Glucocorticoid-induced osteonecrosis is a known toxicity in pediatric and young adult patients treated for Acute Lymphoblastic Leukemia (ALL) and Non-Hodgkin Lymphoma (NHL). Osteonecrosis of the shoulders and weight-bearing joints of the lower extremities has emerged as a major adverse effect of modern ALL therapy. Pain in the absence of activity (ie, rest pain) occurs in approximately two-thirds of patients, and nocturnal pain occurs in one-third. MRI continues to be the gold standard for diagnosis in symptomatic and asymptomatic patients, especially in early-stage disease. Respectively to Preiser disease, this condition is a rare disease of unknown etiology characterized by Avascular Necrosis (AVN), also known as osteonecrosis, of the scaphoid bone and the clinical manifestations include insidious and progressive pain lasting from months to years, edema, loss of strength and reduced range of motion in the wrist. The treatment of non-traumatic osteonecrosis remains one of the most controversial subjects in the orthopedic literature. The purpose of this case report is to bring to attention osteonecrosis as a potential side effect of corticosteroid use in the pediatric population, as a delayed or missed diagnosis can lead to several joints destruction.
Citation: Cunha R, Verraest X, Martins P, Madureira R, Pereira A. Clinical case of preiser disease, bilateral femoral head and humeral head osteonecrosis associated with chronic corticosteroid therapy. J Clin Images Med Case Rep. 2021; 2(4): 1269.
Case report
An 18-year-old woman, came to an appointment at the orthopedic department, for having pain in both hips and shoulders that initially related to boxing practice.
She has personal history of LLA B, who underwent chronic corticosteroid therapy, ended the treatment in 2013 – during this time she was followed by oncology. She made x-ray that shown avascular necrosis of large joints, with collapse and fracture of the humeral and femur heads. Was propose for joint replacement with bilateral hemiarthroplasty of the shoulders in 2016 and total joint replacement of the hip in 2014 and 2015 - followed up in orthopedics.
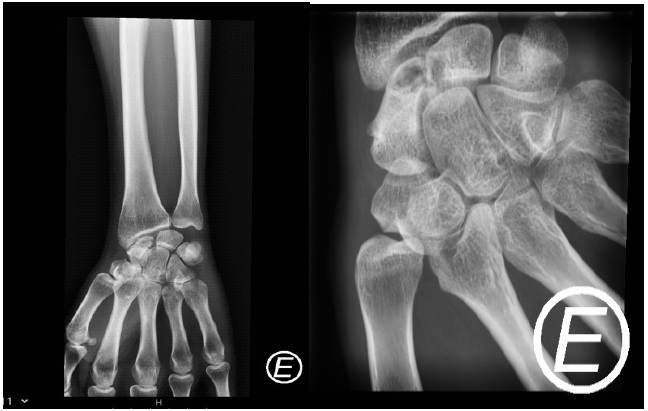
Later on, at the age of 26, the patient started with pain at the left wrist. On physical examination, she presented radial scaphoid pain in the loaded wrist, with range of motion of 70 degrees in both dorsiflexion and palmar flexion.
The left-hand x-ray showed sclerosis of the body and cystic lesion of the proximal pole. It was requested left hand MRI that confirmed the suspicion of scaphoid necrosis/Preiser disease.
Once the patient had mild symptoms, it was decided at this stage, to try conservative treatment, with joint immobilization for two months. A new appointment was scheduled after 4 months to consider surgical treatment if the symptoms persist.



Discussion
Osteonecrosis, also known as aseptic necrosis, Avascular Necrosis (AVN), atraumatic necrosis, and ischemic necrosis, is a pathologic process that is associated with numerous conditions and therapeutic interventions.
The annual incidence of all types of osteonecrosis doubled from 1989 to 2003 (from 1.4 to 3/100,000), perhaps due to the more frequent use of MRI. Most commonly, the hip is involved but almost any bone can develop osteonecrosis [1]. It can occur in the anterolateral femoral head, but also affect the femoral condyles, humeral heads, proximal tibia, vertebrae, and small bones of the hand and foot.
The most frequent etiological factors are trauma, alcoholism, and chronic glucocorticoid therapy; the later causing the most devastating form of osteonecrosis [1]. Adolescence is the most consistently identified and most significant risk factor, with patients >10 years old at the highest risk [2]. Glucocorticoid-induced osteonecrosis is a known toxicity in pediatric and young adult patients treated for Acute Lymphoblastic Leukemia (ALL) and non-Hodgkin lymphoma (NHL) [2]. Osteonecrosis of the shoulders and weight-bearing joints of the lower extremities has emerged as a major adverse effect of modern ALL therapy [3]. In a study of 10,729 new-onset acute lymphoblastic leukemia patients (age range, 2.02 to 21.23 years), 242 (2.3 percent) developed osteonecrosis within five years of their acute lymphoblastic leukemia diagnosis [4]. Glucocorticoid therapy (prednisone and dexamethasone) is commonly used in the treatment of acute lymphoblastic leukemia, and it may increase the risk for osteonecrosis (particularly dexamethasone) [5].
The early events leading to osteonecrosis are poorly understood. All contributing mechanisms finally lead to an imbalance between the actual and the required bone perfusion, which may be related to intravascular clotting/embolism (intraluminal obliteration), increased marrow pressure (extraluminal obliteration), and direct blood vessel injury. In addition, the direct toxic effects of chemotherapy on bone marrow and bone cells may disturb bone integrity and contribute to osteonecrosis [2]. The adverse effects of glucocorticoids on the skeleton are primarily due to direct actions on osteoblasts and osteoclasts, decreasing the production of both osteoblasts and osteoclasts and increasing the apoptosis of osteoblasts while prolonging the lifespan of osteoclasts [1]. Numerous studies relate the use of systemic glucocorticoids to the development of osteonecrosis. In one study of 1199 joints in 302 patients, the incidence of developing osteonecrosis as a consequence of systemic glucocorticoids ranged from 21 to 37 percent; the frequency varies, depending, in part, upon the associated comorbidities, duration, and dose6. The patients can have bilateral involvement at the time of diagnosis, including disease of the hips, knees, and shoulders or another non-hip joint.
A complete history should be made including questions related to the various risk factors. The most common presenting symptoms of osteonecrosis is pain. In many cases there is weight bearing or motion-induced pain. Pain in the absence of activity occurs in approximately two- thirds of patients, and nocturnal pain occurs in one-third [7]. When an extremity is affected, the position of the limb (eg, elevated, dependent) does not alter the pain. Although rare, pain in multiple joints suggests a multifocal process. A small proportion of patients are initially asymptomatic, particularly in early-stage disease; in these cases, the diagnosis is usually incidental. Asymptomatic involvement contralateral to a symptomatic site is also frequently noted. Physical findings are largely nonspecific [8].

Preiser disease
It is a rare disease of unknown etiology characterized by avascular necrosis (AVN), also known as osteonecrosis, of the scaphoid bone, described by Preiser in 1910 [10]. The clinical manifestations are characterized by insidious and progressive pain lasting from months to years and sometimes edema in the dorsal-radial region of the wrist, which may be associated with loss of strength and reduced range of motion in the wrist, with hypersensitivity in the region of the wrist [11].
The most commonly cited radiographic classification for Preiser disease is a 4-stage classification proposed by Herbert and Lanzetta in 1994 [12].
Cases were classified radiographically as: (1) normal x-rays with positive bone scan, (2) increased density of proximal pole, (3) fragmentation of proximal pole, and (4) carpal collapse pattern. For early-stage disease, the authors proposed either conservative treatment or vascularized bone grafting to potentially alter the course of disease [13]. In 2003, Kalainov et al [14]. Classified patients into 2 types, based on MRI characteristics, in a retrospective study of 19 patients. Type 1 had diffuse scaphoid involvement on MRI and had worse outcomes and increased radiographic deterioration, whereas type 2 had limited proximal pole involvement and more favorable outcomes. In addition, type 1 cases were more often associated with steroid use (not statistically significant), and type 2 cases had a statistically significant higher rate of previous wrist trauma. The clinical implications of this classification, however, are unclear. So far, therapy and prognosis are based on retrospective case series with a low number of patients. The treatment is controversial; non-surgical measures consist of physiotherapy and kinesiotherapy, immobilization, NSAID and, occasionally, steroid infiltration. Multiple surgical approaches may be used in these cases, among which carpectomy of the proximal row is included, proximal scaphoid excision with a silastic replacement, radial styloidectomy with bone debridement and implant, total wrist arthroplasty, large and semilunar bone fusion or scaphoid debridement with vascularized bone implant. Revascularization procedures are performed in those cases with necrosis but without degenerative changes, while more aggressive treatments (proximal row carpectomy of the wrist) are indicated in patients who already have osteoarthritic changes [13].
References
- Weinstein RS. Glucocorticoid-induced osteonecrosis; Endocrine. 2012; 412: 183–190.
- Kunstreich M, et al. Osteonecrosis in children with acute lymphoblastic leukemia; Haematologica. 2016; 10111: 1295–1305.
- Jones LC, et al. Team approach: Management of osteonecrosis in children with acute lymphoblastic leukemia – Pediatric Blood & Cancer. 2020; 67: 2020.
- Heneghan MB, et al. Treatment of Osteonecrosis in Children and Adolescents With Acute Lymphoblastic Leukemia; Clin Lymphoma Myeloma Leuk. 2016; 164: 223.
- Hiroto Inaba, MD, Prof. Ching-Hon Pui, MD; Glucocorticoid use in acute lymphoblastic leukaemia; Lancet Oncol. 2010; 1111: 1096–1106.
- Shigemura T, et al. Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: Prospective MRI study. Rheumatology Oxford. 2011; 5011: 2023-2028.
- Lespasio MJ, et al. Osteonecrosis of the Hip: A Primer. Perm J. 2019; 23: 18-100.
- Lynne C Jones, PhD, Michael A Mont, MD, Clinical manifestations and diagnosis of osteonecrosis avascular necrosis of bone. 2021.
- Jones LC, Mont MA, Treatment of nontraumatic hip osteonecrosis avascular necrosis of the femoral head. in adults; Up To Date. 2021.
- Preiser G. Eine typische posttraumatische und zur spontanfraktur führende ostitis des naviculare carpi]. Fortschr Geb Roentgenstr. 1910; 15: 189-197.
- Julio Got, Javier A. Cavallasca; Bilateral Avascular Necrosis of the Scaphoid Preiser’ Disease., a Rare Cause of Wrist Pain; Reumatol Clin. 2014; 106: 418–421.
- Herbert TJ, Lanzetta M. Idiopathic avascular necrosis of the scaphoid. J Hand Surg Br. 1994; 192: 174 –182.
- Lin JD, Strauch RJ. Preiser Disease. Journal of Hand Surgery. 2013; 38: 1833-1834.