
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A voluminous portal cavernoma of the hepatic pedicle with severe portal hypertension
Ibrahima Niang*; Cheikh Tidiane Diop; Khadidiatou Ndiaye Diouf; Mbaye Thiam; Sokhna Ba
Radiology Department, Fann University Hospital Center, Dakar, Senegal.
*Corresponding Author: Ibrahima Niang
Radiology department, Fann University Hospital
Center, 5035 Avenue Cheikh Anta DIOP, Dakar,
Senegal.
Email: niangibrahimaniang@gmail.com
Received : Jun 02, 2021
Accepted : Aug 13, 2021
Published : Aug 18, 2021
Archived : www.jcimcr.org
Copyright : © Niang I (2021).
Abstract
Portal cavernoma is the cavernous transformation of the portal vein. It is the consequence of chronic portal vein thrombosis and occurs when collateral branches develop to bypass the portal occlusion. The clinical presentation includes hematemesis due to variceal bleeding, ascites or anemia, and splenomegaly. Herein we present images of a 37-year-old male patient received in our department for abdominal ultrasound, following 2 episodes of hematemesis. This case illustrates the ultrasound aspect of a voluminous portal cavernoma with portal hypertension signs.
Keywords: portal cavernoma; portal thrombosis; portal hypertension; ultrasound.
Citation: Niang I, Diop CT, Diouf KN, Thiam M, Ba S. A voluminous portal cavernoma of the hepatic pedicle with severe portal hypertension. J Clin Images Med Case Rep. 2021; 2(4): 1271.
Clinical image description
We report the case of a 37-year-old male patient received in our department for abdominal ultrasound, following 2 episodes of hematemesis. On clinical examination, the patient had a poor general condition with significant abdominal distension.
This ultrasound showed a non-dysmorphic liver of normal size with regular contour and homogeneous parenchyma. Presence of a lace of multiple varicose, dilated and tortuous veins at the level of the hepatic hilum with a hepatopetal flow on color Doppler (Figure 1A & B). The portal vein was occluded without visualized portal flow. No abnormality of the gallbladder and bile ducts.
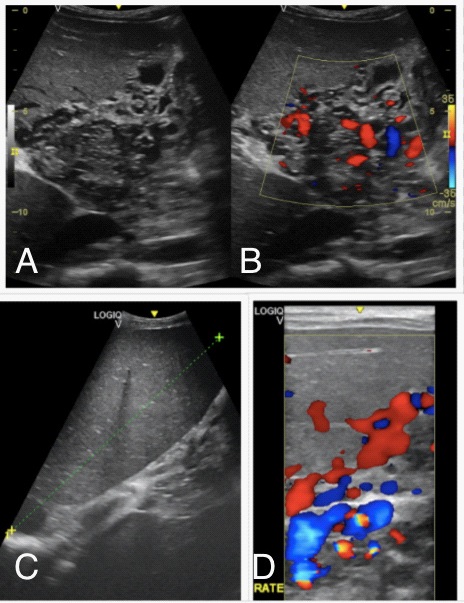
The spleen is enlarged, homogeneous with the presence of splenic varices (Figure 1C & D).
All this led to the diagnosis of portal cavernoma secondary to chronic portal thrombosis and complicated by portal hypertension.
Portal cavernoma is the cavernous transformation of the portal vein. It is the consequence of chronic portal vein thrombosis and occurs when collateral branches develop to bypass the portal occlusion [1]. The clinical presentation includes hematemesis due to variceal bleeding, ascites or anemia, and splenomegaly [2].
Its diagnosis is made by imaging with ultrasound as the first tool and it should also look for possible biliary consequences due to compression of the main biliary tract by the varicose veins. This compression of the bile duct is responsible for portal cholangiopathy [3].
Author’s contribution: IN and CTD wrote the manuscript with input of MT. KND preparation of the figures and proof reading. SB drafting and final approval of the version to be published.
References
- Berzigotti A, Piscaglia F. Ultrasound in portal hypertension--part 1. Ultraschall Med. 2011; 32: 548-68.
- Vibert E, Azoulay D, Castaing D, Bismuth H. [Portal cavenorma: Diagnosis, aetiologies and consequences]. Ann Chir. 2002; 127: 745-50.
- Kalra N, Shankar S, Khandelwal N. Imaging of portal cavernoma cholangiopathy. Journal of clinical and experimental hepatology. 2014; 4: S44-52.