
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An unusual case of breast abscess in a male patient
Adiel Cohen1*ϯ; Bar Avital1* ϯ; Elchanan Parnasa1; Yafa Shani Parnasa2; Yonatan Oster3
1 Hadassah Hebrew University Medical Center, Jerusalem, Israel.
2 Department of Surgery, Hadassah Hebrew University Medical Center, Jerusalem, Israel.
3 Faculty of Medicine, Hebrew University of Jerusalem, Department of Clinical Microbiology and Infectious Diseases, Hadassah Hebrew University Medical Center, Jerusalem, Israel.
ϯ Equal contribution
*Corresponding Author: Yonatan Oster
Department of Clinical Microbiology and Infectious
Diseases, Hadassah-Hebrew University Medical
Center, Ein Kerem POB 12000, Jerusalem 91120,
Israel.
Email: yonatano@hadassah.org.il
Received : July 22, 2021
Accepted : Aug 19, 2021
Published : Aug 23, 2021
Archived : www.jcimcr.org
Copyright : © Oster Y (2021).
Abstract
A 49-year-old male patient presented to the emergency department with acute onset of painful swelling in the left breast. An unusual diagnosis of breast abscess was made using ultrasound scan, incision and drainage were performed followed by antibiotics, with full recovery.
Keywords: breast abscess; male.
Citation: Cohen A, Avital B, Parnasa E, Parnasa YS, Oster Y. An unusual case of breast abscess in a male patient. J Clin Images Med Case Rep. 2021; 2(4): 1277.
Introduction
Breast abscess is a type of a breast infection, found mainly in females. It is an uncommon complication of mastitis with a reported incidence of 0.1-3% % in breastfeeding women [1-2].
The differential diagnosis includes benign and malignant pathologies which included epidermal inclusion cyst, sebaceous cyst, post traumatic hematoma and ductal carcinoma. The most common etiology of the male breast lumps is gynecomastia and the majority of them are benign. Radiological modalities play an important role in evaluating male breast lesions, it is the key to narrow down the differential diagnosis or to diagnose accurately [3].
Case presentation
The patient is a 49-year-old, Israeli Arab male patient with past medical history of Ischemic Heart Disease, Hypertension, Hypertriglyceridemia and Diabetes Mellitus. He presented at the emergency department with acute onset painful left breast swelling.
He noted progressive pain over the past days, particularly with palpation, accompanied with swelling and redness of the breast.
The patient denied any fever, chills, nipple discharge, night sweats, weight loss, or skin laceration, no history or findings consistent with local trauma. He had no personal history of similar complains, and no known family history of breast or ovarian cancer.
On physical examination there was a 20mm palpable fluctuated lump in the left breast around the areola, with no nipple retraction. The palpable mass was red, warm and tender. Physical examination of the axilla and right breast was unremarkable.
Lab tests showed increased leukocytosis of 14.3 109 /L (normal range: 4.05-11.84 109 /L), with 62% neutrophils (normal range: 42%-77%). C-reactive protein was slightly elevated up to 2.33mg/dl (0-0.5). The rest of the laboratory results were normal.
He underwent an ultrasound scan of the left breast which showed a well-defined small echogenic lesion at a 5 o’clock position, measured up to 13 X 12 mm and surrounded by echogenic fat. The hypoechoic center of this lesion was up to 4 X 6 mm (Figure 1).
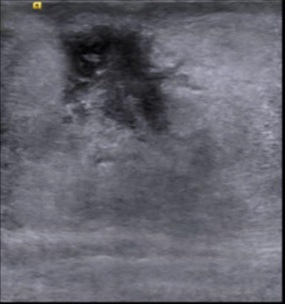
Those findings led to the final diagnosis of breast abscess. Incision and drainage were performed with a 10 mm cut, at the center of the abscess. Small amount of pus was drained with an immediate relief of the pain.
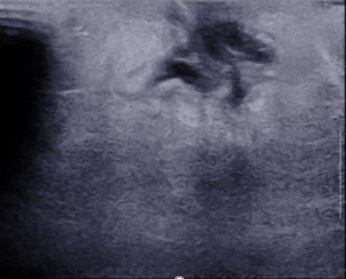
An empiric antibiotic treatment of First-generation Cephalosporin IV was administered. Due to lack of improvement, after two days, cefazolin was replaced by Vancomycin. During his hospitalization, a follow up ultrasound scan was performed, showing edematous breast tissue posteriorly to the nipple without any suspicious lesion or defined collection. These findings can reassemble inflammation and fully drained abscess. Axillary lymphadenopathy was not seen (Figure 2).
Culture from the pus obtained was positive to Staphylococcus Epidermidis, and while the patient improved clinically, he was discharged home, for additional oral antibiotic treatment with Clindamycin for additional 5 days.
Discussion
It is important to be aware that breast pathologies, which usually occur in females, can occur in males. The majority of the breast lumps in males are benign, and the most common reason is gynecomastia [3]. The main predisposing factor for breast infections in women is breastfeeding [1]. Breast infections and abscesses in male patients are very rare with unknown incidence or predisposing features.
A subareolar abscess is a localized infection secondary to ductal ectasia, chronic obstruction, and inflammation. Staphylococcus Aureus and Staphylococcus Epidermidis are the most common causative organisms [3-5]. There are more benign non-neoplastic breast lesions in males such as epidermal inclusion cyst, sebaceous cyst, post traumatic hematoma and fat necrosis, seroma, diabetic mastopathy, periductal chronic inflammation and ductal ectasia, granulomatosis mastitis and intramammary lymph node [3]. Malignant pathologies should always be part of the differential diagnosis. Furthermore, breast cancer presenting initially as an abscess has been described a handful of times in the literature [6]. Therefore, a follow up US after resolution of the abscess is important as was recommended to our patient.
Conclusion
Although a subareolar abscess is a rare infection in males, clinicians should acknowledge this entity since it night be a sign for a life threating disease such as breast cancer. Moreover, even in a simple infection this pathology is usually ignored, making more suffering for the patient. This article emphasizes the importance of considering this entity, in the hope it will contribute to better outcomes for those patients
References
- Dener C, Inan A. Breast Abscesses in Lactating Women. World Journal of Surgery. 2003; 27: 130-133.
- Amir LH, Forster D, Mclachlan H, Lumley J. Incidence of breast abscess in lactating women: Report from an Australian cohort. BJOG: An International Journal of Obstetrics and Gynaecology. 2004; 111: 1378-1381.
- Önder Ö, Azizova A, Durhan G, Elibol FD, Akpınar MG, et al. Imaging findings and classification of the common and uncommon male breast diseases. Insights into Imaging. 2020; 11.
- Nguyen C, Kettler MD, Swirsky ME, et al. Male Breast Disease: Pictorial Review with Radiologic-Pathologic Correlation. RadioGraphics. 2013; 33: 763-779.
- Versluijs-Ossewaarde FNL, Roumen RMH, Goris RJA. Subareolar Breast Abscesses: Characteristics and Results of Surgical Treatment. The Breast Journal. 2005; 11: 179-182.
- Ventham NT, Hussien MI. Male breast cancer is rare: an initial presentation may be as an abscess. BMJ Case Reports. 2010; 2010.