
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Fracture of the humerus in arm wrestling: An uncommon mechanism for a common fracture
Adnene Benammou*; Walid Balti; Firas Belatra; Mehdi Bellil; Kooli Mondher; Mohamed Ben Salah
Department of Orthopedic Surgery, Charles Nicolle’s hospital, Tunisia.
*Corresponding Author: Adnene Benammou
Department of Orthopedic Surgery, Charles
Nicolle’s hospital, Tunisia.
Email: Adnene.benammou@gmail.com
Received : July 05, 2021
Accepted : Aug 19, 2021
Published : Aug 23, 2021
Archived : www.jcimcr.org
Copyright : © Benammou A (2021).
Abstract
A case of a healthy young patient which had a spiral fracture of humerus shaft during an arm-wrestling game. Various differential diagnosis should be assessed. Treatment is the same as a fracture of humerus shaft from any other mechanism.
Keywords: muscular contraction; fracture; humerus; humeral fractures; arm wrestling.
Citation: Benammou A, Balti W, Belatra F, Bellil M, Mondher K, et al. Fracture of the humerus in arm wrestling: An uncommon mechanism for a common fracture. J Clin Images Med Case Rep. 2021; 2(4): 1280.
Introduction
Arm wrestling is a widespread sport which can cause an unusual injury: fracture of the humerus. Bending moment, axial compression and torsional forces applied to the humerus are known to be the cause of such fracture [1,2]. It was first described in 1975 by Brismar and Spangen [3]. Particular attention should be payed to eliminate differential diagnosis. We report the case of a 20-year-old male who sustained a humerus fracture during arm wrestling to discuss the differential diagnosis and the management of this type of lesion.
Case report
A healthy 20-year-old male, student, with no medical history presented to the emergency department complaining of left arm pain. He had been arm-wrestling when he felt a sudden crack and pain in the left arm. He had to abandon due to pain.
Interrogatory did not reveal any weight loss, impaired general condition, asthenia, fever, night-sweats or any drug intake.
Physical examination found a patient with attitude of traumatized upper left limb, a deformation of the arm with no skin damages. Neurovascular examination was normal.
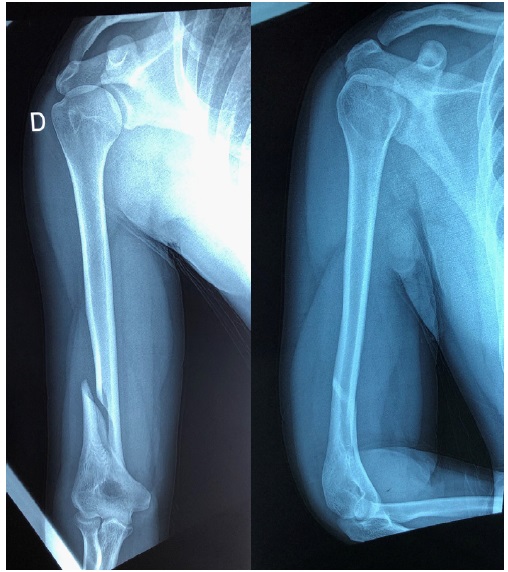
Radiography of the humerus showed a spiral fracture at the junction of the middle third and distal third of the humeral diaphysis (Figure 1). Radiological assessment did not show any preexisting lesion or an anomaly of bone structure evoking a pathological fracture. No further radiological examination (CTscan, MRI, Scintigraphy) were requested.
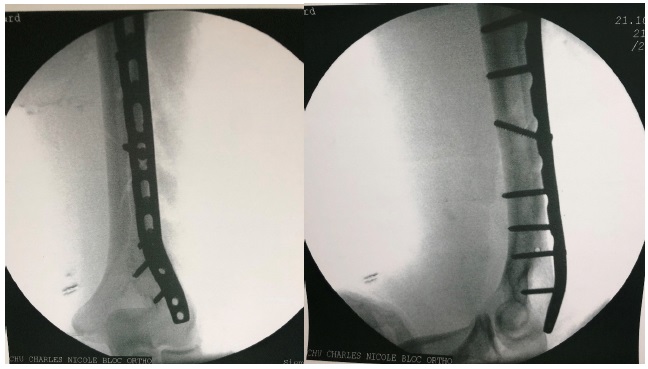
For the treatment, we chose a surgical treatment through an external approach with an Open Reduction Internal Fixation (ORIF) with a Locking Compression Plate (LCP) (Figure 2). Postoperative radial nerve examination was normal. Physical therapy has been started at day one post operatory.
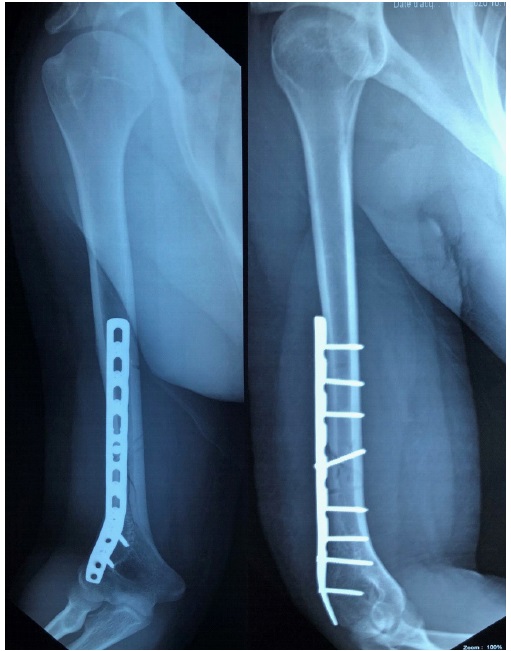
Postoperative course was uneventful (Figure 3).
Discussion
Diaphyseal fracture of the humerus usually occurs after direct trauma [4]. Spiral fractures of humeral shaft had been described as unusual complications of sports which include torsional forces such as arm wrestling [3] or overhead throwing of different types of object [5]. Position of the arm is known to be the key element to the fracture pattern [6].
While arm-wrestling, the humeral shaft is trapped between two opposite torsional moment, one created by the shoulder with a moment of internal rotation (pectoralis major, teres major, latissimus dorsi and subscapularis) and the other created by the opponent applied the elbow joint with a moment of external rotation [1].
The fracture usually occurs in middle third distal third junction. This might be explained by the lack of balance between the internal and external diameter and the low mineral density of the distal third of the humeral shaft compared to other bones [7].
The frequency of this type of fracture may be underrated [1] and is more important in Japan where Ogawa [8] reported 30 cases. The fractures usually occur in middle or distal third of the of the shaft.
Diagnosis is made with interrogatory for the mechanism and radiographs of the humerus. Cutaneous and neurovascular complications are rare [9,10].
Special attention should be payed in eliminating differential diagnosis which can be stress fracture [11] even if they are rare in the upper limb, steroids intake in recreational or professional athlete [12] or pathological fracture due to bone metastases [13].
Treatment is not different from a humerus shaft fracture. It can be orthopedic or surgical ( intramedullary nailing, intramedullary wiring, plate fixation) [14]. In our case, we chose ORIF with Locking Compression Plate to start early rehabilitation.
Conclusion
Arm wrestler should be well aware of injuries that can happen. Even if diagnosis of a humerus fracture which happen on arm wrestling game is simple, physician should linger on differential diagnosis. Treatment is like any other shaft fractur of the humerus.
Acknowledgements: The authors declare no conflict of interest.
References
- Benhima MA, Younsi A, Abkari I, Najeb Y, Fikry T. Fracture de l’humérus au cours d’une partie de « bras de fer ». Analyse d’un mécanisme « peu commun » pour une fracture « commune ». Sci Sports. 2014; 29: 138‑42.
- Ahˇcan U, Aleˇs A, Zavrˇsnik J. Spiral Fracture of the Humerus Caused by Arm Wrestling. Eur J Trauma. 2000; 4.
- Brismar B, Spangen L. Fracture of the humerus from arm wrestling. Acta Orthop Scand. 1975; 46: 707‑8.
- Saab M. Arm wrestler’s fracture. Eur J Emerg Med Off J Eur Soc Emerg Med. déc 1999; 6: 407‑8.
- Linn RM, Kriegshauser LA. Ball thrower’s fracture of the humerus: A case report. Am J Sports Med. 1 mars. 1991; 19: 194‑7.
- Whitaker JH. Arm wrestling fractures-A humerus twist. Am J Sports Med. avr 1977; 5: 67‑77.
- Pedrazzini A, Pedrazzoni M, De Filippo M, Nicoletto G, Govoni R, Ceccarelli F. Humeral fractures by arm wrestling in adult: A biomechanical study. Acta Bio-Medica Atenei Parm. août 2012; 83: 122-6.
- Ogawa K, Ui M. Humeral shaft fracture sustained during arm wrestling: report on 30 cases and review of the literature. J Trauma. févr. 1997; 42: 243‑6.
- Chao SL, Miller M, Teng SW. A mechanism of spiral fracture of the humerus: a report of 129 cases following the throwing of hand grenades. J Trauma. 1971; 11: 602‑5.
- de Barros JW, Oliveira DJ. Fractures of the humerus in arm wrestling. Int Orthop. 1995; 19: 390‑1.
- Stress fracture of the humerus: A case study - Murray E. Allen. 1984.
- Napp M, Frank M, Amtsberg G, Hinz P, Ekkernkamp A. [Humeral fracture due to arm wrestling - an indirect fracture in a doped athlete]. Sportverletz Sportschaden Organ Ges OrthopadischTraumatol Sportmed. 2011; 25: 118‑20.
- Dijkstra S, Stapert J, Boxma H, Wiggers T. Treatment of pathological fractures of the humeral shaft due to bone metastases: A comparison of intramedullary locking nail and plate osteosynthesis with adjunctive bone cement. Eur J Surg Oncol EJSO. 1996; 22: 621‑6.