
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A case report of ectopic salivary gland tissue in the larynx
K Sleurs1*; S Van Der Heijden1; B De Vries2; J Smit1
1 Department of Otorhinolaryngology, Zuyderland Medisch Centrum, Henri Dunantstraat 5 6419 PC Heerlen and Sittard-Geleen, Netherlands.
2 Department of Pathology, Zuyderland Medisch Centrum, Henri Dunantstraat 5 6419 PC Heerlen and Sittard-Geleen, Netherlands.
*Corresponding Author: Kristien Sleurs
Department of Otorhinolaryngology, Zuyderland
Medisch Centrum, Henri Dunantstraat 5 6419 PC
Heerlen and Sittard-Geleen, Netherlands.
Email: kristien.sleurs@student.kuleuven.be
Received : July 05, 2021
Accepted : Aug 23, 2021
Published : Aug 26, 2021
Archived : www.jcimcr.org
Copyright : © Sleurs K (2021).
Abstract
Submucosal laryngeal masses are challenging for ENT specialists as the diagnosis usually remains uncertain until histopathological examination is carried out. We report a case of a 54-year old man complaining of dysphonia and globus sensation. Flexible laryngoscopic examination showed a submucosal swelling in the right anterior laryngeal ventricle. Microlaryngoscopic excision of the submucosal mass was performed. Histological examination revealed salivary gland tissue. We found only a few cases in the literature of ectopic salivary gland tissue situated in the larynx. In these cases, the salivary gland tissue was also located at the anterior portion of the true or false vocal fold.
Thus, it is necessary to consider this condition in the differential diagnosis of a submucosal mass in the anterior true or false vocal fold or laryngeal ventricle.
Keywords: ectopic salivary gland; heterotopic salivary gland; choriostoma; larynx; laryngeal ventricle; submucosal mass.
Citation: Sleurs K, Heijden SVD, Vries BD, Smit J. A case report of ectopic salivary gland tissue in the larynx. J Clin Images Med Case Rep. 2021; 2(4): 1283.
Introduction
A submucosal mass in the larynx may result from a range of pathologies such as laryngoceles, cysts, systemic diseases, benign and malignant non-epithelial neoplasms. Benign nonepithelial tumors in the larynx include granular cell tumors, lipomas, neurofibromas and rhabdomyomas [1]. Malign tumors comprise of chondrosarcomas, synovial cell sarcomas, lymphomas, neuro-endocrine carcinomas, rhabdomyosarcomas and adenoid cystic sarcomas [1]. A submucosal mass may also be caused by a systemic disease such as amyloidosis, sarcoidosis or lupus [2]. Clinical symptoms may include dysphonia, dysphagia, sore throat, throat clearing, hemoptysis and a neck mass. CT imaging may give information about the size and extension of the lesion (e.g. extension in the paraglottic space) but may not differentiate between the aforementioned pathologies [1]. The final diagnosis is achieved after histological examination.
In our case, histological examination revealed ectopic salivary gland tissue. Ectopic salivary gland tissue is normal salivary gland tissue without malignant features outside the major and minor salivary glands. It is mostly seen in intraparotid lymph nodes [3] and less commonly in cervical lymph nodes in the mid and low neck [4]. Rarely ectopic salivary glands are seen in other regions of the head and neck for example in the middle ear [5] or thyroid gland [6]. We present a rare case of ectopic salivary gland located in the larynx.
Case presentation
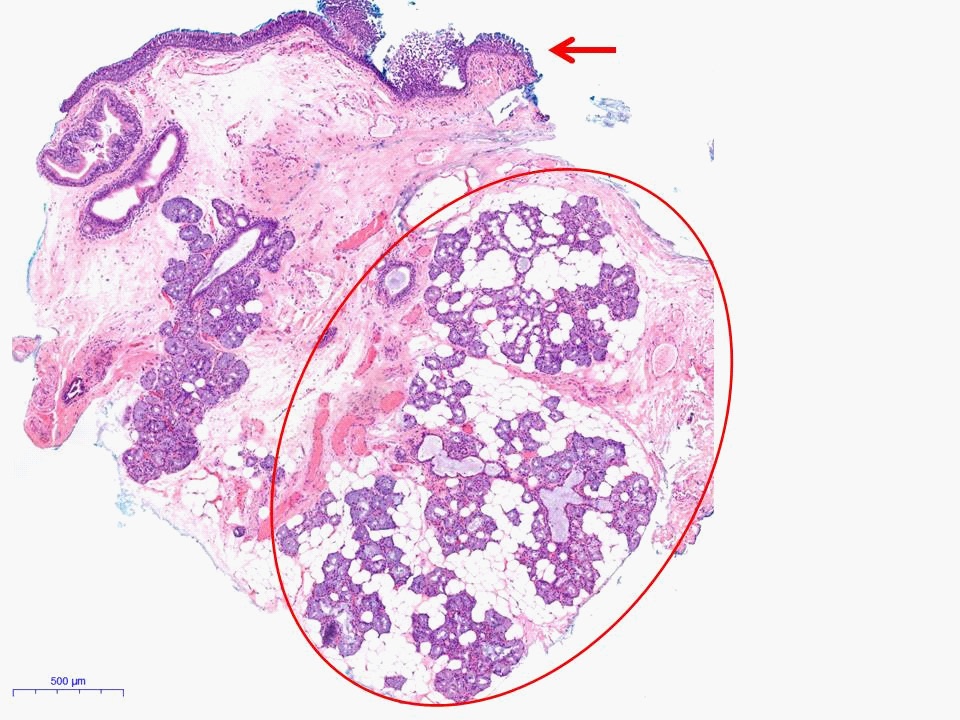
A 54-year old man was referred to an ENT specialist because of dysphonia and globus sensation. The man had no complaints of sore throat or swallowing difficulties. He never smoked and his alcohol consumption was moderate. There was no history of intubation or laryngeal trauma. Flexible laryngoscopic examination showed a small submucosal mass anterior in the right laryngeal ventricle extending just medially to the false vocal fold (Figure 1). Stroboscopy showed a reduced wave pattern in the right true vocal cord. No mass was detected with neck palpation. Laryngoscopy 4 months later revealed an unchanged image of the submucosal mass anterior in the laryngeal ventricle. Because of bothersome hoarseness and indistinct diagnosis, microlarygoscopic excision of the mass was performed under general anesthesia. Per-operatively the submucosal swelling was incised using a cold knife, whereafter a yellowish smooth mass appeared with a similar aspect as salivary gland tissue. The mass was pulled medially using forceps and removed as laterally as possible using scissors. Pathological examination confirmed the diagnosis of ectopic salivary gland tissue without malignant features (Figure 2).

Material and methods
A literature search was conducted in April 2021 using Pubmed and Embase databases. Articles were identified using terms ‘ectopic salivary gland’, ‘heterotopic salivary gland’ or ‘salivary gland choriostoma’ and ‘larynx’ or ‘laryngeal’. No languages restrictions were imposed. We found 5 case reports representing similar cases (Table 1).
Table 1: Review in literature of other cases of ectopic salivary gland tissue in the larynx.
Author |
Year |
Country |
Localization |
Side |
Age |
Sex |
Treatment |
Valentino et al.7 |
2020 |
USA |
False vocal cord |
L |
56 |
M |
Laser resection |
Tajima et al.8 |
2018 |
Japan |
Anterior false vocal cord |
L |
46 |
M |
Biopsy + follow-up |
Yilmaz et al.9 |
2017 |
Turkey |
Anterior vocal cord |
L |
43 |
M |
Surgical resection |
Kempf et al.10 |
2005 |
Germany |
Vocal cord |
L |
80 |
M |
Laser resection |
Kruk-Zagajewska et al. 11 |
1999 |
Poland |
Laryngeal ventricle |
Not mentioned |
56 |
M |
Not mentioned |
Discussion
In our case, the ectopic salivary gland tissue was located in the anterior laryngeal ventricle. In other cases found in literature, the ectopic salivary gland tissue was found in the anterior portion of the false vocal cord [7,8], true vocal cord [9,10] and - as in our case - in the laryngeal ventricle [11]. The age of the patients ranged from 43 [9] till 80 [10] years. Interestingly, all 6 patients, including our case, were males. The patients complained of hoarseness [7,9,10], productive coughing [9,10], sore throat [8] and throat clearing [7]. In the cases of Valentino et al [7]. and Tajima et al [8]. CT and MRI showed a solid tissue nodule without signs of inflammation or malignancy. In our case pre-operative imaging was not performed.
Surgical excision of the salivary gland tissue is sufficient and has a low risk of recurrence. In the case of Valentino et al [7]and Kemph et al [10] a CO2 laser was used. In our case cold instruments were used. In our patient laryngoscopy was repeated 1 week and 3 months after surgery. Neither in our case, nor in the other cases, recurrence was observed.
From the 6th week of gestation the salivary glands develop out of oral epithelium of ectoderm origin that invades the surrounding mesenchyme [12]. The secretory acini and excretory ducti arise from these epithelial invaginations and the gland capsule and septa with blood vessels will develop from the mesenchymal tissue. It is unclear how salivary gland tissue that originates form oral epithelium migrates to the larynx [12].
Malignant transformation of ectopic salivary gland tissue is extremely rare but has been reported in intraparotid and cervical lymph nodes [3]. In these cases metastasis from an unknown primary lesion was ruled out by the clinician and pathologist [3].
Differential diagnosis for the submucosal mass in our patient is including saccular cyst, laryngocele, amyloidosis, sarcoidosis, granular cell tumor, lipoma and neurofibroma [1,2]. Based on the anterior localization of the lesion a saccular cyst is more probable than a laryngocele. A saccular cyst is a mucous-filled dilatation of the saccule in the anterior or lateral larynx, while a laryngocele is an air-filled enlargement of the ventricle that extends towards the posterosuperior false vocal or aryepiglottic fold2 . Laryngeal amyloidosis was a possible diagnosis in our case. In amyloidosis submucosal masses consist of immunoglobulin light chain fragments and are located in the ventricle, false vocal fold, true vocal fold, aryepiglottic fold or subglottis [2]. Laryngeal involvement in sarcoidosis is characterized by edematous, pale swellings most often located in the supraglottis [2], but sarcoidosis is mostly accompanied with lung and skin involvement. Lipomas are most often located in the false vocal fold or aryepiglottic fold [1,2] and have a characteristic appearance on CT or MRI imaging. The predilection site of a granular cell tumor, that consists of Schwann cells, is the true vocal fold [1]. Neurofibroma, that arise from perineural fibrocytes, are found around the nerve endings of the internal branch of the superior laryngeal nerve in the aryepiglottic fold or arytenoid [1,2]. The submucosal mass in our case did not have the typical red brownish appearance of rhabdomyoma [1,2] or red bluish color of hemangioma or lymphangioma. A malignant cause was unlikely because neither obvious tumor growth nor symptoms of malignancy (e.g. fatigue, weight loss) were present.
Conclusion
In conclusion, it is necessary to include ectopic salivary gland tissue in the differential diagnosis of a laryngeal submucosal mass, especially when it is located in the anterior true or false vocal cord or laryngeal ventricle.
References
- Friedman AD, Burns JA, Lutch MJ, Zeitels SM. Submucosal neoplasms of the laryngeal introitus. The Journal of laryngology and otology. 2012; 126; 706–713.
- Marvin PF, Melin T. Clinical Laryngology The essentials. New York, USA: Thieme. 2015; 62-73.
- Faras F, Abo-Alhassan F, Bastaki J, Al-Sihan MK. Primary Mucoepidermoid Carcinoma Arising from Ectopic Salivary Tissue within an Intraparotid Lymph Node. Case reports in otolaryngology. 2015; 879137.
- Tsakiropoulou E, Konstantinidis I, Vital I, Triaridis S, Vital V. Ectopic Warthin’s tumour presenting as a neck mass. B-ENT. 2008; 4; 111–115.
- Enoz M, Suoglu Y. Salivary gland choristoma of the middle ear. The Laryngoscope 2006; 116; 1033–1034.
- Levy GH, Marti JL, Cai G et al. Pleomorphic adenoma arising in an incidental midline isthmic thyroid nodule: A case report and review of the literature. Human pathology. 2012; 43; 134–137.
- Valentino W, Paknezhad H, Sataloff RT. Heterotopic Salivary Gland Tissue in the Larynx. Ear, nose, & throat journal. 2020; 99; NP84–NP85.
- Tajima S, Yamauchi K, Higo R, Ikeda K. A case of ectopic salivary gland of the larynx. Auris nasus larynx. 2018; 45; 633–636.
- Yılmaz R, Bedir R, Şehitoğlu İ, Dursun E. Salivary Gland Choristoma of the Larynx. Balkan medical journal 2017; 34; 288–289.
- Kempf HG, Störkel S. Choristom des Taschenbandes [Choristoma in the vocal fold]. HNO 2005; 53; 361–363.
- Kruk-Zagajewska A, Manasterski J, Gładysz, J. Heterotropowa tkanka gruczołu ślinowego imitujaca torbiel przedsionka krtani [Heterotopic salivary gland imitating laryngeal cyst]. Otolaryngologia polska = The Polish otolaryngology. 1999; 53; 623–625.
- Sangeetha Priya P, Anitha N, Rajesh E, Masthan KMK. Embryology and development of salivary gland. European Journal of Molecular & Clinical Medicine. 2020; 7; 764-770.