
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Where is the stent? CTA assists angiography: A case of jailed LAD
Ilana Golub; Suraj Dahal; Suvasini Lakshmanan; Matthew J Budoff*
Harbor-UCLA Medical Center Lundquist Institute, Torrance, CA, USA.
*Corresponding Author: Matthew J Budoff
Lundquist Institute, 1124 W Carson St. Torrance, CA
90502, USA.
Email: mbudoff@lundquist.org
Received : July 17, 2021
Accepted : Aug 27, 2021
Published : Sep 02, 2021
Archived : www.jcimcr.org
Copyright : © Budoff MJ (2021).
Abstract
Stent malpositioning in the septal perforator is a serious procedural complication and especially prominent after main vessel stenting in coronary bifurcation lesions. This case report demonstrates Computed Tomography Angiography’s (CTA) role as a backup imaging tool, in cases where follow-up Coronary Angiogram (CAG) cannot be immediately completed. CTA also functions as a preferred imaging tool to follow up after stenting and assess for stent malpositioning. A 72-year-old female with history of hypertension and hyperlipidemia presented with dyspnea and was found to have STEMI. About a week after her three PCI’s to the Left Anterior Descending (LAD) artery, she returned to the hospital with recurrent dyspnea and V-Tach. Instead of completing a repeat catheterization, a noninvasive CTA was thought to be the next test. CTA imaging indicates that the failed stenting of the side-branch resulted in a jailed main vessel, which may induce ischemia and ventricular tachycardia (V-Tach). After the malpositioned stent finding on CTA, the patient was then referred to the Cath Lab for angiogram. CTA thus provided detailed anatomical information about the stent’s placement, which will greatly assist further management by the interventional cardiologist.
Keywords: computed tomography angiography; angiography; sidebranch compromise; percutaneous coronary intervention; Optical coherence tomography
Citation: Golub I, Dahal S, Lakshmanan S, Budoff MJ. Where is the stent? CTA assists angiography: A case of jailed LAD. J Clin Images Med Case Rep. 2021; 2(5): 1290.
Introduction
This report documents a rare case of stent malpositioning in the septal perforator, a serious procedural complication especially prominent after Main Vessel (MV) stenting in coronary bifurcation lesions [1]. Computed Tomography Angiography (CTA) allows for accurate anatomical assessment of stent malposition, especially critical in cases where follow-up Coronary Angiogram (CAG) cannot be immediately completed. CTA thus helps facilitate the precise subsequent interventional management via guidewire or balloon dilation [2]. If left untreated, this “Jailed Stent” may otherwise lead to periprocedural infarction, flow deterioration, abnormal local shear stresses, or heightened stent thrombosis and chronic restenosis [3]. Here, we present a rare but critical case. Failed stenting of the Side-Branch (SB) resulted in a jailed main vessel, which may induce ischemia and Ventricular Tachycardia (V-Tach).
Acute septal perforator occlusion manifests in approximately 12-41% of all Percutaneous Coronary Interventions (PCI) [2]. As 18-20% of stented lesions involve bifurcations and >50% of patients contain side branches within the angioplasty site, stents are often deployed across the SB ostium [3]. In fact, 2.9-19% of stents placed across a major side-branch demonstrate occlusion [3]. For successful clinical outcomes, it is therefore imperative that PCI’s at coronary bifurcations maintain long-term efficacy and are monitored for compromise or occlusion. Though the confirmation of jailing type in coronary bifurcation intervention is traditionally accomplished via Optical Coherence Tomography (OCT) [4], CTA offers increased spatial resolution with highquality multiplanar and 3-D reconstructed imaging. In addition to locating exact stent position, CTA also rules out acute aortic dissection, saddle pulmonary embolism, and ventricular thrombus after the MI. While dyspnea and EKG changes after PCI require coronary angiogram, CTA offers a rapid and non-invasive tool to assess urgent symptoms [5]. Here, we present a unique case report to demonstrate CTA’s role as a supplementary imaging tool, in cases where follow-up angiography cannot be immediately completed.
Case series
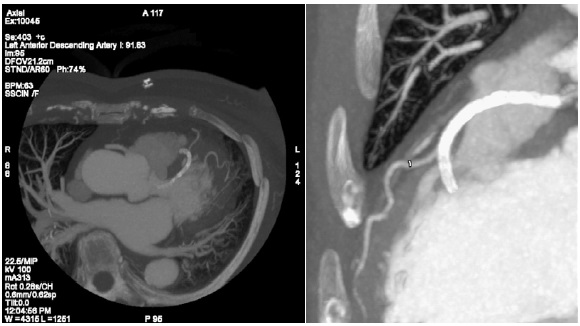
A 72-year-old female originally presented for cardiac evaluation with dyspnea, hypertension, and hyperlipidemia. After being diagnosed with a ST-Elevation Myocardial Infarction (STEMI), she had an angiogram with three PCI’s to the Left Anterior Descending (LAD) artery. About a week later, she returned to the hospital due to recurrent dyspnea and ventricular tachycardia. At that time, she was newly diagnosed with pericarditis and V-Tach. After completing an EP study, a loop recorder was placed. Approximately 2 months after stenting, she presented again with dyspnea that occurred both at rest and exertion. Instead of completing a repeat catheterization, a noninvasive CTA was thought to be the next test. Coronary CTA (CCTA) indicated no severe stenosis in any of the coronary arteries, but it identified the presence of a failed stent lodged in the septal perforator that subsequently jailed the distal LAD (Figure 1). Despite the jailed LAD, there is still antegrade flow in the distal vessel.
Discussion
The Figure 1 CTA illustrated that the patient’s three LAD stents were fully patent. However, the last stent appeared to veer medially off the parent LAD, in the direction of a septal branch. Seeing as septal perforators are not traditionally stented, our case presents an interesting question. Did this distal-most PCI transcend the LAD and perforate myocardium? Or, conversely, has the stent been mistakenly implanted into a septal branch?
CTA imaging indicated that the stent in the septal perforator was wedged deep in the interventricular septum. This unique finding explains the patient’s V-Tach. If CTA were done in advance, the loop recorder would have been avoided and a follow-up angiography may have been indicated earlier. After CTA’s malpositioned stent finding, the patient was then referred to the Cath Lab for angiogram. CTA thus provided detailed anatomical information about the stent’s placement, which will greatly assist further management by the interventional cardiologist.
Here, CTA provides a quick, noninvasive postprocedural screening tool and supplements CAG in cases when angiography cannot be completed immediately. This identification of stent placement failure clarifies the patient’s recent pericarditis and V-tach, and ameliorates outcomes that would otherwise retain heightened ischemic risk.
Conclusion
In conclusion, this case report demonstrates CTA’s well-suited modality to accurately and sensitively facilitate a misplaced stent diagnosis, particularly if a patient cannot undergo urgent coronary angiogram. CTA also provides diagnostic capabilities to rule out alternate causes of chest pain such as pulmonary embolism and aortic dissection. CTA offers high spatial resolution, enabling the comprehensive assessment of device positioning. Coronary CT angiography clinically adjudicates a jailed main vessel from the SB, in a noninvasive manner and with limited operator variability. This case demonstrates CTA’s role in providing coronary anatomy and detailed information about the stent’s placement. These details, in turn, greatly assist further management by the interventional cardiologist, in creating a personalized plan to care for the patient.
References
- Hahn JY, Chun WJ, Kim JH, et al. Predictors and outcomes of side branch occlusion after main vessel stenting in coronary bifurcation lesions: results from the COBIS II Registry (Coronary BIfurcation Stenting). J Am Coll Cardiol. 2013; 62: 1654-1659.
- Bhargava B, Waksman R, Lansky AJ, Kornowski R, Mehran R, et al. Clinical outcomes of compromised side branch (stent jail) after coronary stenting with the NIR stent. Catheter Cardiovasc Interv. 2001; 54: 295-300.
- Yamawaki M, Muramatsu T, Araki M, et al. Natural history of side branches jailed by drug-eluting stents. J Interv Cardiol. 2012; 25: 37-46.
- Holm NR, Tu S, Christiansen EH, Reiber JH, Lassen JF, Thuesen L, Maeng M. Use of three-dimensional optical coherence tomography to verify correct wire position in a jailed side branch after main vessel stent implantation. Euro Intervention. 2011; 7: 528- 9.
- Ostrom MP, Gopal A, Ahmadi N, Nasir K, Yang E, Kakadiaris I, Flores F, Mao SS, Budoff MJ. Mortality incidence and the severity of coronary atherosclerosis assessed by computed tomography angiography. J Am Coll Cardiol. 2008; 52: 1335-43.