
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Effects of magnetic stimulation compared to electrical stimulation on muscle contraction in quadriceps femoris muscle of healthy subjects: A pilot study
Ryosuke Nakanishi1,2; Minoru Tanaka1,3; Noriaki Maeshige1; Hidemi Fujino1*
1 Department of Rehabilitation Science, Kobe University Graduate School of Health Sciences, Kobe, Japan.
2 Department of Physical Therapy, Kobe International University, Kobe, Japan
3 Department of Rehabilitation Science, Osaka Health Science University, Osaka, Japan.
*Corresponding Author: Hidemi Fujino
Professor, Department of Rehabilitation Science,
Kobe University Graduate School of Health Sciences,
7-10-2 Tomogaoka, Kobe 654-0142, Japan.
Email: fujino@phoenix.kobe-u.ac.jp
Received : July 21, 2021
Accepted : Sep 02, 2021
Published : Sep 07, 2021
Archived : www.jcimcr.org
Copyright : © Fujino H (2021).
Abstract
Background/Aims: This study investigated whether pulsed magnetic stimulation contracts superficial and/or deep muscles compared with those induced by electrical stimulations, i.e., low- and kilohertzfrequency currents.
Methods: Eight healthy subjects were recruited and measured the quadriceps femoris muscle thickness using ultrasound imaging, and Visual Analog Scale (VAS) for stimulation-induced pain during the same stimulation intensity.
Results: Pulsed magnetic stimulation increased the thickness of rectus femoris muscle similar to other electrical stimulations, but not the vastus intermedius muscle. Meanwhile, the pain score of VAS caused by pulsed magnetic stimulation was lower than that by those electrical stimulations.
Conclusions: These results suggest that pulsed magnetic stimulation is effective for the contraction of superficial layer muscles without stimulation-induced pain but not for contraction of deep layer muscles.
Keywords: pulsed magnetic stimulation; electrical stimulation; stimulation-induced pain; muscle contraction.
Citation: Nakanishi R, Tanaka M, Maeshige N, Fujino H. Effects of magnetic stimulation compared to electrical stimulation on muscle contraction in quadriceps femoris muscle of healthy subjects: A pilot study. J Clin Images Med Case Rep. 2021; 2(5): 1297.
Introduction
Electrical stimulation is classified into electrical stimulation using a low-frequency current and electrical stimulation using a burst-modulated kilohertz-frequency current, according to frequency characteristics [1-3]. Electrical stimulation using a lowfrequency current is used in clinical sites and has characteristics that are effective for the contraction of superficial layer muscle but it has no effect on deep layer muscle [4,5]. On the other hand, electrical stimulation using a burst-modulated kilohertzfrequency current which is delivered at a frequency of 2,500 Hz and burst modulated at a low levels frequency (such as 50, or 100 Hz) is expected to reach and contract deep layer muscle [3,5]. However, both electrical stimulations may have disadvantageous characteristics resulting in withdrawal from treatment because of strength-dependent stimulation-induced pain as a result of the unavoidable stimulation of skin nociceptors [6,7].
Pulsed magnetic stimulation, which is effective as a muscle contraction method, can avoid stimulation-induced pain [8-10]. Magnetic stimulation uses a magnetic field, which results in the generation of eddy currents to contract muscle fibers via depolarization of the neural membrane [11]. A magnetic field can penetrate high resistance tissues, resulting in minimal activation of the skin nociceptors [11,12]. Several studies have indicated the magnetic stimulation generates joint torque via stimulation of the lower limb muscles such as hip flexion, and knee extension [9,10,13]. However, it is not yet clear what depth the magnetic stimulation reaches and causes muscle contraction. Therefore, the purpose of this study is to investigate whether pulsed magnetic stimulation contracts superficial and/or deep muscles compared with those induced by electrical stimulation using a low-frequency current and electrical stimulation using a burst-modulated kilohertz-frequency current. If this study is validated, new non-invasive therapeutic interventions for skeletal muscle contraction can be established.
Methods
A pilot randomized and three-way crossover study was conducted in one laboratory. At first, the peak torque during maximum voluntary isometric contraction was measured using an isokinetic dynamometer (Cybex NORM; Computer Sports Medicine Inc., New York, USA). After the peak torque was measured, we set the current intensity to induce a 20% maximum voluntary isometric contraction using each stimulator. The next day, the muscle thickness of Rectus Femoris Muscle (RF) and Vastus Intermedius Muscle (VI), and the levels of stimulation-induced pain during pulsed magnetic stimulation, and electrical stimulations at 20% of the torque level of Maximum Voluntary Isometric Contraction (MVIC) were measured. All experiments were conducted in an environmentally controlled room at 25±2°C.
Ethical approval
The subjects were informed of all the procedures, purposes, benefits, and risks of the study and signed an informed consent form, which was approved by the Medical Ethical Committee of Kobe International University in accordance with the declaration of Helsinki (G2018-087).
Recruitment
This study recruited eight healthy subjects (29.3 ± 5.5 years old, 174.4 ± 6.8 cm, 63.6± 10.3 kg). The subjects with a history of injury to the lower limbs or could not tolerate electrical stimulation equivalent to 20% MVIC were excluded. The subjects were asked to avoid stimulants (e.g. alcohol, caffeine, chocolate) on the test day, and did not perform any intense exercise for 2 days prior to the tests.
Intervention
Pulsed magnetic stimulation, electrical stimulation using a low-frequency current, and electrical stimulation using a kilohertz-frequency alternating current were performed on a pulsed magnetic stimulator (Pathleader; IFG Co., Ltd., Miyagi, Japan), low- frequency current electric stimulator (ES-520; Ito Co., Ltd., Tokyo, Japan), and burst-modulated kilohertz-frequency current electric stimulator (ES-520; Ito Co., Ltd.,), respectively. These stimulator currents used a frequency of 50 Hz. A pulsed magnetic stimulation probe was placed 50 mm upper from the motor point along to RF, because the circular coil using this magnetic stimulation causes the peak of electric fields a little distant point from the center of the coil [14]. The electrical stimulation electrodes (50 × 90 mm) were placed on the front of the thigh: one electrode was placed 50 mm upper from the motor point along to RF, and the other was placed 50 mm lower from the motor point along to RF, resulting in placing so as to sandwich the motor point.
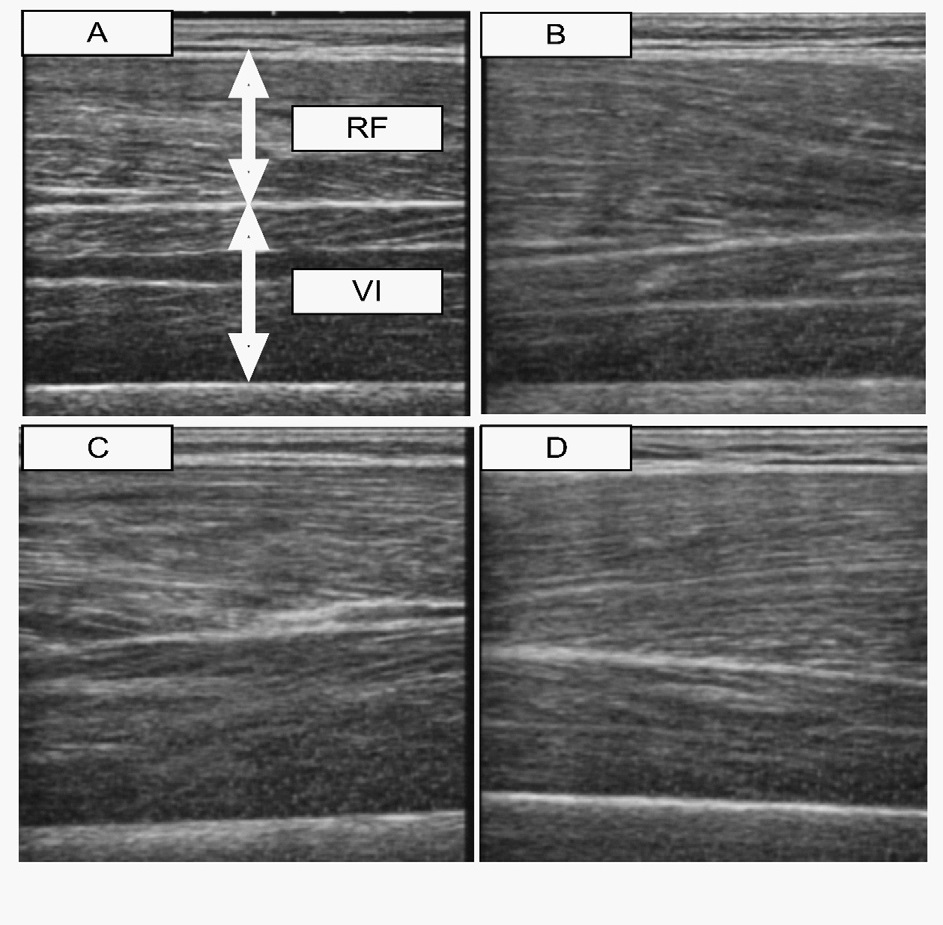
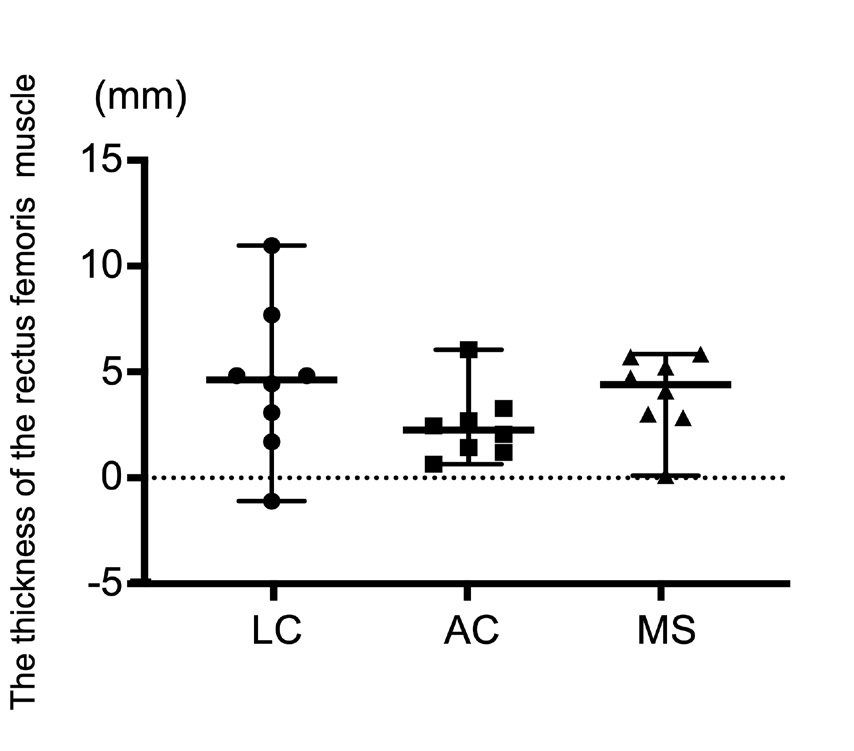
The thickness of RF and VI was measured attained during rest and each stimulation. These thicknesses were measured using an ultrasound image device with 9 MHz linear transducers (EUB-415, HITACHI Medical Co, Tokyo, Japan). The ultrasound image device probe was placed on the center of between the electrodes, meaning the motor point. Briefly, subjects were placed on the isokinetic dynamometer with a knee joint angle of 90° and were measured the thickness at rest (Figure 1A). Next, the RF and VI thickness were recorded using video mode during each stimulation with the current value equivalent to 20% maximum voluntary isometric contraction for 2 seconds. The RF and VI thickness adopted the points with the largest values during the measurement time (Figure 1B,1C,1D). Subjects took 5 minutes of rest to avoid fatigue among each stimulation. The presented data of the measured value during each stimulation minus the rest value is given in Figure 2, 3.
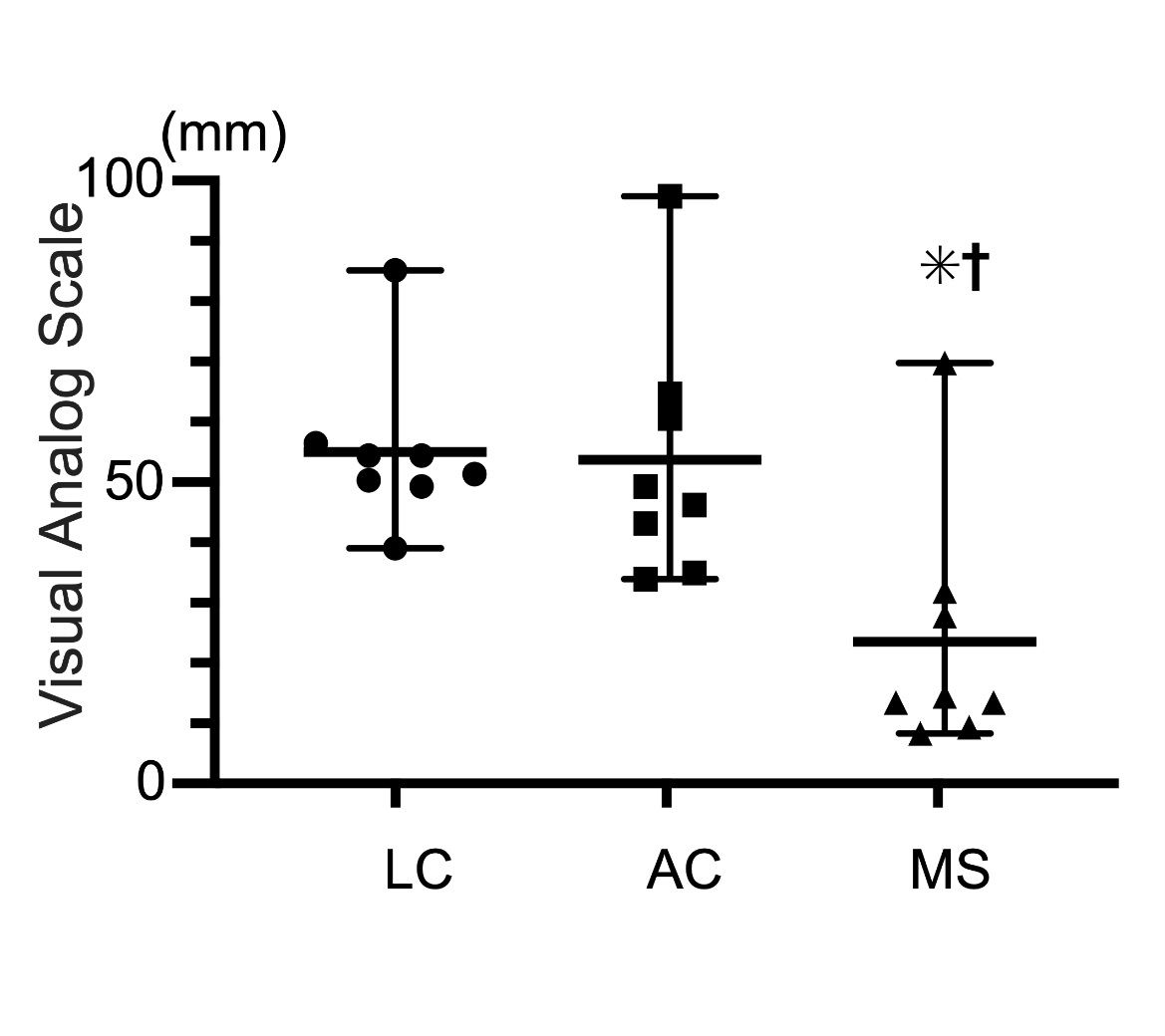
Evaluation of stimulation-induced pain perception was done using the Visual Analog Scale (VAS). Subjects were asked to evaluate stimulation-induced pain perception intensity immediately after each stimulation and indicate levels on a paperbased VAS. The intensity of pain was rated on a numerical scale from 0 mm to 100 mm (0 mm=no pain, 100 mm=worst pain imaginable).
Data analysis
Data were presented as median (min-max). Friedman’s test was used for comparisons by condition, and Tukey’s post-hoc test was used for multiple comparisons. p-values less than 0.05 were considered statistically significant.
Results
The thickness of the rectus femoris muscle (RF) and vastus intermedius muscle (VI) muscle during each stimulation
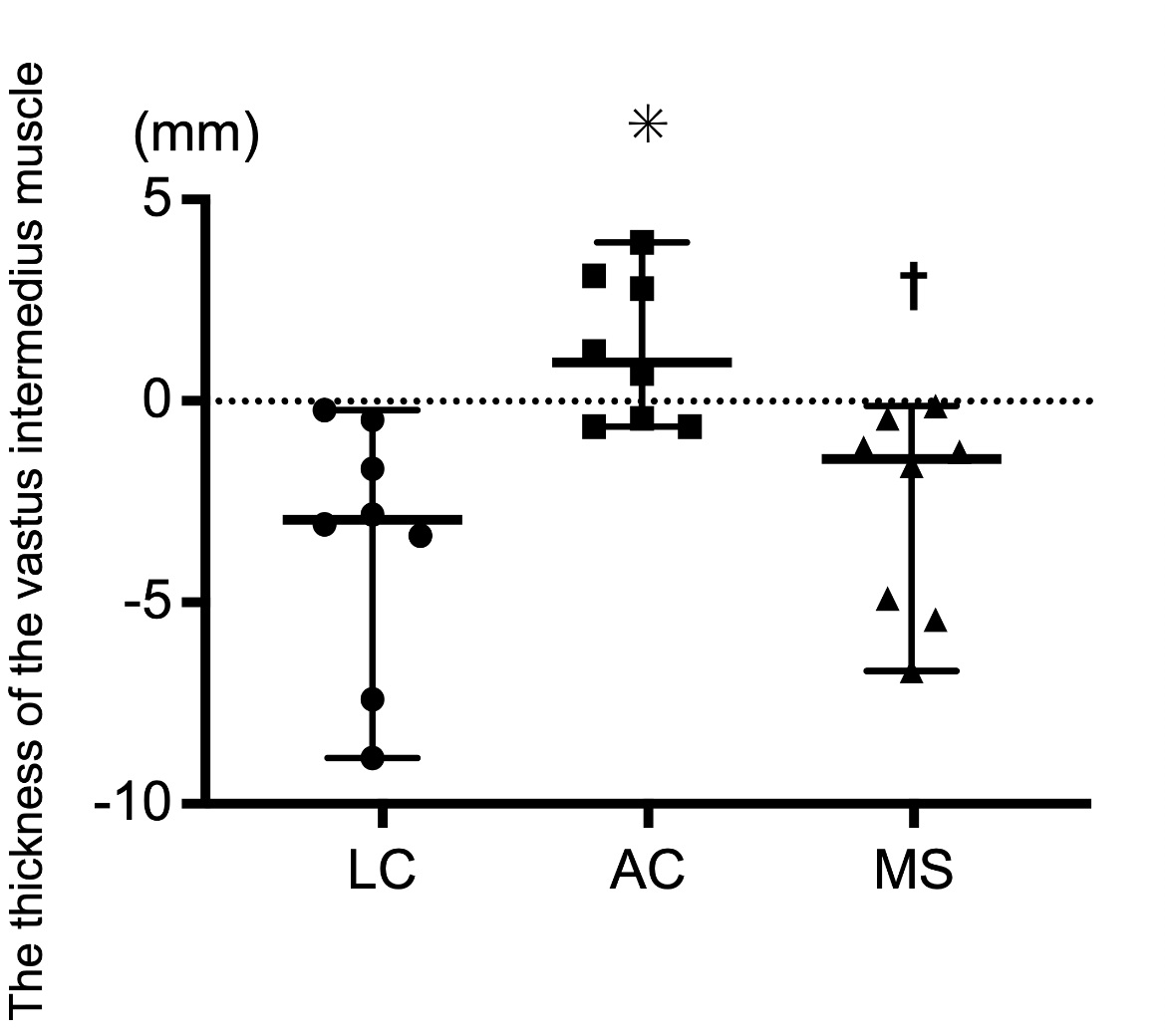
There were no significant differences in the thickness of the RF muscle between the electrical stimulation using a lowfrequency current, a burst-modulated kilohertz-frequency current, and pulsed magnetic stimulation (Figure 2). Meanwhile, the thickness of the VI muscle in the electrical stimulation using a burst-modulated kilohertz-frequency current was significantly thicker than that using a low-frequency current, and in the pulsed magnetic stimulation (Figure 3).
Visual analog scale (VAS) during each stimulation
There were no significant differences in the VAS pain score between the electrical stimulation using a low-frequency current and using a burst-modulated kilohertz-frequency current. However, the pain score of VAS in the pulsed magnetic stimulation was significantly lower compared to both electrical stimulations (Figure 4).
Discussion
The novel findings of this study were that pulsed magnetic stimulation during generating joint torque was effective for the contraction of superficial layer muscle without stimulation-induced pain perception but failed to contract deep layer muscle.
Pulsed magnetic stimulation, as with electrical stimulations, could increase the thickness of rectus femoris muscle in the present study. Delaney et al. showed that change in quadriceps muscle thickness during voluntary muscle contraction can be assessed using an ultrasound imaging device with 6 MHz linear transducers in healthy subjects. Therefore, the change in muscle thickness on the ultrasound imaging device also represents muscle contraction in the present study.
Pulsed magnetic stimulation and electrical stimulation using a low-frequency current failed to increase the thickness of vastus intermedius muscle. In contrast, electrical stimulation using a burst-modulated kilohertz-frequency current could increase the thickness of vastus intermedius muscle. The previous study has shown that a magnetic field can penetrate high resistance tissues and reach the deep layer central nerve [11,12,15]. However, Baker et al., [16] indicate that the electric field induced by the magnetic field attenuates rapidly with distance from the surface probe. For that reason, the current evoked by pulsed magnetic stimulation most likely was insufficient to depolarize motor neurons in the deep muscle tissue. In addition, it is known that the depth reached when using electrical stimulation depends on the frequency [5]. Ward [3] indicated that electrical stimulation using a burst-modulated kilohertz-frequency current has less electrical energy lost in the skin due to a decrease in skin impedance. Hence, electrical stimulation using a burstmodulated kilohertz-frequency current with high frequency reached the deep tissues and depolarized motor neurons of deep muscles resulting in contraction of the vastus intermedius muscle. Meanwhile, magnetic stimulation as well as electrical stimulation using a low-frequency current has a large energy loss and it did not reach the deep tissues in the skeletal muscle.
The pain score of VAS was increased during muscle contractions with pulsed magnetic stimulation and electrical stimulations. Whereas, the pain score of VAS was lower in the muscle contractions with pulsed magnetic stimulation than the muscle contractions with electrical stimulations. Han et al. showed that the pain score of VAS using 25Hz magnetic stimulation is lower than that using electrical stimulation with the same frequency and intensity in quadriceps femoris of healthy subjects [9]. In addition, Szecsi et al. also indicated that magnetic stimulation caused less pain than electrical stimulation under the same joint torque generation when applying 30 Hz electrical stimulation and magnetic stimulation to the quadriceps femoris of paresis patients [17]. Therefore, even magnetic stimulation with the frequency of 50 Hz induced less pain during muscle contraction using in this study. The cause of electrical stimulationinduced pain is skin nociceptors, but the magnetic fields used in magnetic stimulation can easily penetrate through the skin [11]. In addition, pulsed magnetic stimulation causes an ion flow in the muscle directly, resulting in a contraction of the muscle [16]. On the other hand, electrical stimulation carries electrons and transfer the ions nearby the nociceptors, resulting in a contraction of the muscle [16]. Hence, pulsed magnetic stimulation likely has a lower the VAS pain score than both electrical stimulations. The data also suggest that magnetic stimulation may be an effective superficial muscle contraction method for subjects whose pain is induced by electrical stimulation.
A limitation of this study is that we did not investigate the flowing current levels of each tissue during stimulation. Future studies should be performed to investigate the flowing current effects of each stimulation. In this study, we measured the pain intensity during stimulation at only a subjective pain intensity and do not know what the effects would be at an objective pain intensity using biomarker measurements. Future studies should address these points on a larger number of subjects.
Conclusions
In conclusion, pulsed magnetic stimulation was effective for the contraction of superficial layer muscle without stimulationinduced pain perception but failed to contract deep layer muscle. The data also suggest that pulsed magnetic stimulation may be an effective rehabilitation regimen as a therapeutic tool for superficial muscles in subjects who cannot continue treatment due to stimulus-induced pain.
Conflicts of interest: The authors declare no conflict of interest.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Ward AR, Shkuratova N. Russian electrical stimulation: the early experiments. Physical therapy. 2002; 82: 1019-30.
- Ward AR, Oliver WG, Buccella D. Wrist extensor torque production and discomfort associated with low-frequency and burstmodulated kilohertz-frequency currents. Physical therapy. 2006; 86: 1360-7.
- Ward AR. Electrical stimulation using kilohertz-frequency alternating current. Physical therapy. 2009; 89: 181-90.
- Monaghan B, Caulfield B, O’Mathuna DP. Surface neuromuscular electrical stimulation for quadriceps strengthening pre and post total knee replacement. The Cochrane database of systematic reviews. 2010: Cd007177.
- Tanaka M, Hirayama Y, Fujita N, Fujino H. Comparison of premodulated interferential and pulsed current electrical stimulation in prevention of deep muscle atrophy in rats. Journal of molecular histology. 2013; 44: 203-11.
- Chae J, Bethoux F, Bohinc T, Dobos L, Davis T, Friedl A. Neuromuscular stimulation for upper extremity motor and functional recovery in acute hemiplegia. Stroke. 1998; 29: 975-9.
- Tanaka M, Nakanishi R, Maeshige N, Fujino H. Effects of Eccentric Contractions Induced Electrical Stimulation Training System on Quadriceps Femoris Muscle. International Journal of Clinical Medicine. 2017; 8: 519-33.
- Polkey MI, Kyroussis D, Hamnegard CH, Mills GH, Green M, Moxham J. Quadriceps strength and fatigue assessed by magnetic stimulation of the femoral nerve in man. Muscle & nerve. 1996; 19: 549-55.
- Han TR, Shin HI, Kim IS. Magnetic stimulation of the quadriceps femoris muscle: comparison of pain with electrical stimulation. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists. 2006; 85: 593-9.
- Ito T, Tsubahara A, Watanabe S. Use of electrical or magnetic stimulation for generating hip flexion torque. American journal of physical medicine & rehabilitation. 2013; 92: 7 55-61.
- Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin Neurophysiol. 2015; 126: 1071-107.
- Beaulieu LD, Schneider C. Repetitive peripheral magnetic stimulation to reduce pain or improve sensorimotor impairments: A literature review on parameters of application and afferents recruitment. Clinical Neurophysiology. 2015; 45: 223-37.
- Hamnegard CH, Sedler M, Polkey MI, Bake B. Quadriceps strength assessed by magnetic stimulation of the femoral nerve in normal subjects. Clinical physiology and functional imaging. 2004; 24: 276-80.
- Williams P, Marketos P, Crowther L, Jiles D. New designs for deep brain transcranial magnetic stimulation. IEEE Transactions on Magnetics. 2011; 48: 1171-8.
- Roth Y, Zangen A, Hallett M. A coil design for transcranial magnetic stimulation of deep brain regions. Journal of Clinical Neurophysiology. 2002; 19: 361-70.
- Barker AT. An introduction to the basic principles of magnetic nerve stimulation. Journal of clinical neurophysiology: Official publication of the American Electroencephalographic Society. 1991; 8: 26-37.
- Szecsi J, Götz S, Pöllmann W, Straube A. Force–pain relationship in functional magnetic and electrical stimulation of subjects with paresis and preserved sensation. Clinical Neurophysiology. 2010; 121: 1589-97.