
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Dumbness revealing Fahr syndrome
M Ouhamou1*; H Laaraj1; I Bouaroua1; J Doufik3; K Mouhadi1,4; I Rammouz1,2
1 Agadir Psychiatric University Center, Morocco.
2 Health Sciences Research Laboratory, Faculty of Medicine, Ibn Zohr University, Agadir, Morocco.
3 Department of Psychiatry, Inzegane Provincial Hospital, Morocco.
4 Department of Psychiatry, Bensergao Military Hospital, Agadir, Morocco.
*Corresponding Author: Ouhamou Mina
Agadir Psychiatric University Center, Morocco.
Email: ouhamoumina@gmail.com
Received : May 01, 2021
Accepted : Sep 02, 2021
Published : Sep 07, 2021
Archived : www.jcimcr.org
Copyright : © Mina O (2021).
Abstract
Fahr’s syndrome is an anatomoclinical entity, defined by Theodor Fahr in 1930. It is determined by the presence of intracerebral, bilateral and symmetrical calcifications, non-arteriosclerotic, located in the basal ganglia. One of its main aetiologies is Pseudohypoparathyroidism (PHP), which shows resistance to the action of Parathyroid hormone (PTH), with mainly hypocalcemia and normal to high levels of PTH.
The clinical manifestations of the disease do not correspond to any specific picture, but they can be dominated by various neuropsychiatric symptoms. We report the case of a 28-year-old young man who had a first psychotic attack a year ago, treated but without therapeutic observance, and who presented for mutism revealing Fahr syndrome.
The evolution was marked by an improvement under conventional neuroleptics.
Keywords: Fahr syndrome; chronic psychotic disorder; neuroleptic.
Citation: Ouhamou M, Laaraj H, Bouaroua I, Doufik J, Mouhadi K, et al. Dumbness revealing Fahr syndrome. J Clin Images Med Case Rep. 2021; 2(5): 1298.
Introduction
Fahr syndrome is a rare anatomoclinical entity, determined by the presence of intracerebral, bilateral and symmetrical calcifications in the basal ganglia.
The clinical symptomatology of the disease may be dominated by various neuropsychiatric symptoms [1]. We report the case of a 28-year-old youngster who presented with mutism revealing Fahr syndrome.
Observation
28-year-old AS patient, originally from and living in Agadir, with no particular medical history, had presented, a year ago, a first psychotic attack that lasted twenty days, made up of behavioral disorders of the type of agitation and aggression associated with ideas of persecution, bizarre behaviors such as checking for closing doors, exploring your home, hyper-vigilance, anxiety and insomnia. The patient was put on: Amisulpride, taken for only a few days.
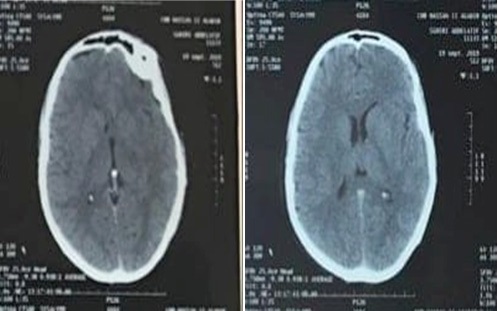
The current episode dates back four months, the patient presented to the emergency room in a picture of mutism associated with vomiting without confusional symptoms, or walking disturbances, or associated infectious syndrome. Hospitalization in neurology was indicated, the neurological examination was without abnormalities. The biological assessment made of PTH, calcemia, magnesium was unremarkable. Brain CT revealed bilateral calcifications of the basal ganglia (Figure 1).
The course was marked by behavioral disturbances in the form of agitation and hetero-aggression, then the patient was referred to a psychiatric consultation.
The psychiatric interview objected to a poorly systematized delusional syndrome with ideas of persecution. The patient’s judgment was impaired, without any awareness of the disturbances.
The evolution after a month on a classic neuroleptic (Haloperidol at a dose of 8 mg/d) was good, the patient reported that he had auditory hallucinations with anxiety, delusions of persecution, and mutism was explained. by the anguish of the persecutors.
During the last consultation on December 31, 2019, the evolution was good under treatment apart from hyper salivation. Halopireridol is replaced by Olanzapine 10 mg/d.
Discussion
Fahr's syndrome associates bilateral and symmetrical intracerebral calcifications of the gray nuclei with phosphocalcic metabolic disturbances. The pathophysiological mechanisms that contribute to the occurrence of intracerebral calcifications are poorly understood [2].
Most of the authors suggest a metabolic disorder of oligoglial cells with deposits of mucopolysaccharides and secondary onset of vascular, perivascular and calcareous lesions [2].
In Fahr's disease (without phosphocalcic disorder), some authors suggest an exaggeration of a normal process of calcium or iron deposits in the basal and indented basal ganglia [3]. Fahr syndrome is generally difficult to suspect clinically because the clinical manifestations do not correspond to any specific picture. It can be intellectual retardation or deterioration, character disturbances, sometimes even delusional episodes [4-5].
The age of clinical onset can range from childhood to old age (up to 80 years in some cases), age at which the attribution of cognitive disorders to Fahr's disease can be argued with more common causes. vascular or degenerative in nature. Likewise, the imputability of Fahr's disease is questionable in a young adult with psychiatric symptoms [6].
The clinical manifestations of Fahr syndrome primarily include neuropsychiatric signs: Psychiatric disorders: Behavioral disorders, delirium or delusional syndrome [8,9].
There is no specific treatment for Fahr's disease. No therapeutic trial has been reported. Symptomatic management may be offered, such as physiotherapy and speech therapy rehabilitation [7]. In terms of medication, psychotropic treatments (antipsychotics, antidepressants, etc.) play an important role when psychiatric symptoms are in the foreground and debilitating [6].
Conclusion
Fahr syndrome is a rare entity. Our observation underlines the interest of looking for the existence of biological and radiological abnormalities in the presence of psychiatric disorders even without neurological signs.
Therefore, the judicious choice of psychotropic drugs and the correction of biological disturbances significantly improve the psychiatric symptoms in these patients.
Declaration of links of interest: The authors declare that they have no competing interest.
References
- Otheman Y, Khalloufi H, Benhima I, Ouanass A. Neuropsychiatric manifestations revealing pseudohypoparathyroidism with Fahr syndrome [Neuropsychiatric symptoms revealing pseudohypoparathyroidism with Fahr’s syndrome]. Encephale. 2011; 37: 54-8.
- Khammassi N, Chrifi J, Mohsen D, Abdelhedi H, Tougourti MN, et al. Fahr syndrome: About two cases [Fahr’s syndrome: two case report]. Rev Neurol (Paris). 2010; 166: 446-450.
- Doumbia M, Kouassi L, Kouame-Assouan AE, Douayoua-Sonan TH, Boa-Yapo F. Fahr disease revealed by walking and speech disorders. Rev Int Sci Med. 2006; 8: 32–5.
- Sbai H, Smail L, Hamdani S, Essatara Y, Harrandou M, et al. Fahr syndrome discovered following pneumococcal meningitis [Fahr syndrome discovered following a bacterial meningitis]. Internal Rev Med. 2008; 29: 412-4.
- Noyelle C, Bruet A, Molho M, Veyssier-Belot C. A confusional syndrome [A confusion. Fahr syndrome]. Internal Rev Med. 2008; 29: 500-1.
- Nicolas G, Guillin O, Borden A, Bioux S, Lefaucheur R, et al. Psychosis revealing familial idiopathic basal ganglia calcification. Gen Hosp Psychiatry. 2013; 35: 575.e3-5.
- Doumbia M, Kouassi L, Kouame - Assouan AE, Douayoua - Sonan TH, Boa - Yapo F. Fahr disease revealed by walking and speech disorders. Rev Int Sci Med. 2006; 8: 32-35.
- Rharrabti S, Darouich I, Benbrahim M, Belahsen F, Rammouz I, Alouane R. A confusional syndrome revealing a Fahr syndrome with hyperparathyroidism [A confusional syndrome revealing a Fahr syndrome with hyperparathyroidism]. Pan Afr Med J. 2013; 14: 123.
- Shakibai SV, Johnson JP, Bourgeois JA. Paranoid delusions and cognitive impairment suggesting Fahr’s disease. Psychosomatics. 2005; 46: 569-72.