
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Adjuvant radiotherapy in recurrent pleomorphic leiomyosarcoma of spermatic cord: A case report and literature review
Angela Pia Solazzo1; Rocchina Caivano1*; Ilaria Benevento1; Giovanni Castaldo1; Antonietta Montagna1; Luciana Rago1; Giusy Carmen Imbriani2; Antonella Bianculli1; Chiara Feoli1; Vito Metallo1; Vincenzo Fusco1
1 Radiation Oncology Department, IRCCS CROB – via San Pio, 1 85028 Rionero in Vulture (Pz), Italy.
2 Surgery Department, IRCCS CROB – via San Pio, 1 85028 Rionero in Vulture (Pz), Italy.
*Corresponding Author: Rocchina Caivano
Radiation Oncology Department, IRCCS CROB – via
San Pio, 1 85028 Rionero in Vulture (Pz), Italy.
Email: rocchina.caivano@gmail.com
Received : July 15, 2021
Accepted : Sep 06, 2021
Published : Sep 10, 2021
Archived : www.jcimcr.org
Copyright : © Caivano R (2021).
Abstract
Pleomorphic leiomyosarcoma of spermatic cord is a very rare urologic disease, so there are no clear guidelines.
The mainstay of treatment is surgery with wide excision margins. The role of adjuvant treatments, such as Chemotherapy (CHT) or Radiotherapy (RT), is not clear, due to the few data available in the literature. However, adjuvant treatments could be considered in patients with a high risk of local recurrence: R1 status after surgery and highgrade histology.
We report the case of 68-year old man affected by recurrent pleomorphic leiomyosarcoma of spermatic cord right, who, in five years, underwent many surgical treatments for local recurrence, and also adjuvant CHT. The last surgery shows positive margins. Therefore, the patient receive adjuvant RT on the surgical bed and right inguinal nodes with a dose of 54 Gy in 27 fractions and VMAT technique.
The treatment was well tolerated, the follow-up at 12 months is negative for local recurrence and show absence of toxicity.
However a long-term follow-up is necessary to confirm the efficacy of radiotherapy on outcomes and especially on local control.
Keywords: pleomorphic leiomyosarcoma; recurrence; positive margins; adjuvant radiotherapy
Citation: Solazzo AP, Caivano R, Benevento I, Castaldo G, Montagna A, et al. Adjuvant radiotherapy in recurrent pleomorphic leiomyosarcoma of spermatic cord: A case report and literature review. J Clin Images Med Case Rep. 2021; 2(5): 1305.
Introduction
Pleomorphic leiomyosarcoma of the spermatic cord is a very rare urologic disease. Management of these tumors is difficult because of their rarity. Among genitourinary sarcomas, the most histology subtypes reported are liposarcoma (20-32%), leiomyosarcoma (19-32%), and rabdhomiosarcoma (11-24%)
Liposarcoma is most common, while leiomyosarcoma and histiocytoma histologic subtypes are the most aggressive [1].
Leiomyosarcoma have a higher incidence after the sixth decade of life [2].
The clinical presentation is usually a unilateral solid, firm, slow-growing mass at the level of the inguinal canal and of the scrotum, sometimes difficult to differentiate from benign lesions. The first-line imaging is ultrasound, but CT and MRI are more specific for diagnosis and surgical planning.
The mainstay of treatment is radical surgery with wide excision margins [3,4]. Adjuvant therapies such as RT and CHT are suggested in selected patients, but clear data to demonstrate any improvement in survival are not available [5].
We report the case of a patient who had many local relapses, all surgically removed and also subjected to adjuvant CHT. The last surgery showed positive margins. Therefore we decided to deliver adjuvant RT with VMAT technique.
Case report
Presentation of case
This is a 68 year old man, ECOG Performance status 0, without sons, affected by pleomorphic leiomyosarcoma of the right spermatic cord who underwent many treatments for local recurrences.
First surgery in 2015, second and third surgery in 2016 and 2017 respectively, after local recurrences. Then, the patient received adjuvant CHT according to the BEP scheme (bleomycin, etoposide, cisplatin).
Neverless, at the beginning of 2020 he presented another local recurrence.
MRI showed solid tumor of 34 x 28 x 38 mm in the right inguinal region, between the right spermatic cord and penis compatible with relapse of the disease.
In March 2020 he undergoes further surgery with excision of the inguinal mass. The histological diagnosis was pleomorphic leiomyosarcoma with positive margins. Therefore, we decided to deliver adjuvant RT.
Treatment
Patient was positioned supine with immobilization systemdevice (VacLock). An abdominopelvic planning CT with 3 mm thickness was performed starting 5 cm above diaphragm and ending 4 cm below the ischial tuberosities. We used the Eclipse Varian Medical System (version 13.6) as treatment planning system and the treatment was delivered using a Varian Trilogy.
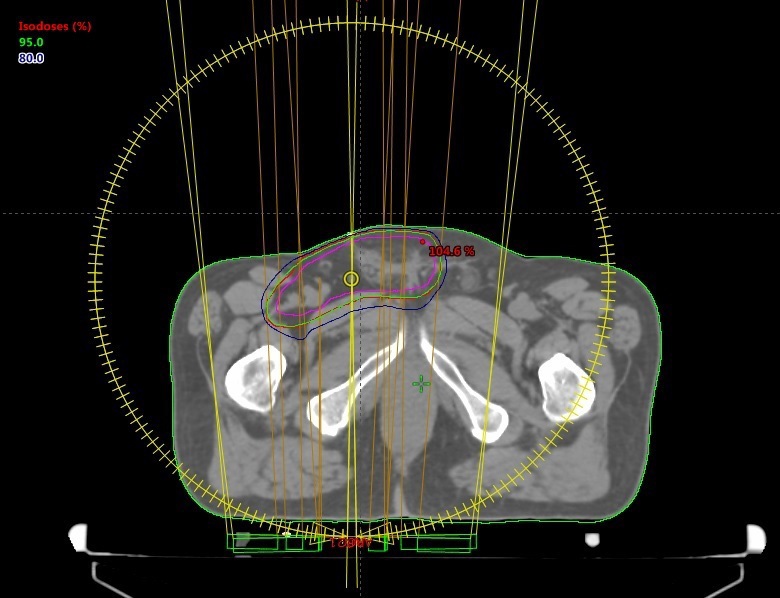
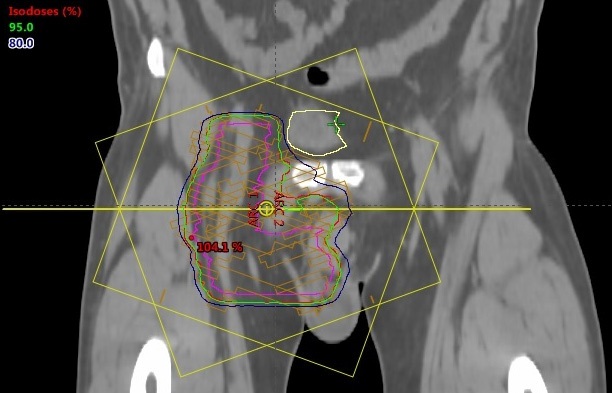
The Clinical Target Volume (CTV) was tumor bed with subclinical extension and right inguinal nodes. The target was delineated in consideration of preoperative MRI. The Planning Target Volume (PTV) was defined with an anisotropic margin of 7 mm around the CTV.
The total dose of 54 Gy in 27 fractions, 5 times a week, was prescribed to PTV. The technique used was VMAT with IGRTdaily CBCT. Organ at risk were the rectum in toto, the bladder in toto, the femoral heads, large bowel (defined as the entire abdominal cavity 2 cm above and below the clinical target volume) and penile bulb. Dose-volume histograms was genereted for all of these organ at risk. According to ICRU 83 [6] recommendation, the Planning Target Volume receive at least 95% of the prescription dose.
The patient was seen twice a week during treatment and for follow-up visits four weeks after completion of treatment, then three month’ interval with pelvic MRI and/or PET/TC with FDG. Acute and long-term toxicities were verified according to CTCAE v4.0 staging system. [7]
Results
The patient did not show toxicity in the first part of the treatment, but experienced G2 skin toxicity (dermatitis) towards the end of the treatment without treatment interruption.
First follow-up at 30 days from the end of RT showed complete resolution of acute skin toxicity with topic therapy based on acid ialuronic.
With a follow-up of 12 months we reported no toxicities and no clinical or radiological evidence of disease.
Discussion
Pleomorphic leiomyosarcoma of spermatic cord is a rare disease so there are no clear guidelines [8].
A wide and complete resection with negative microscopic margins is crucial for treatment of this tumor but no always easy to obtain [9]. Therefore, adjuvant therapy such as RT or CHT could be considered. The role of adjuvant treatments is controversial, due to the limited data in the literature: only case-reports and single institution series with few numbers of patients are present.
Unfortunately, due to the rarity of this disease there is no randomized control studies available in the literature. The role of adjuvant CHT is not clear [10,11]. In fact, our patient after adjuvant CHT experiments another local recurrence.
Coleman et al. from Memorial Sloan-Kettering Cancer Center describe their 20 years surgical experience with spermatic cord sarcomas in 47 patients. In their patient cohort, 21 (45%) were treated with adjuvant RT and 9 (19%) received CHT. However, investigators were unable to demonstrate a therapeutic effect with these therapies. Coleman suggests that there is a benefit from adjuvant RT in high-risk patients affected by spermatic cord sarcoma with multiple recurrences, positive margins, and high grade tumor [12]. Positive margin appears to be a strong prognostic factor predicting outcome as demonstrated by some retrospective studies [13,14]. In Harvard Radiation Oncology of Boston, 25 patients with paratesticular liposarcoma between 1987 and 2009 were reviewed: final margins were positive in 8 patients (32%), RT were given to 10 patients. Among patients who received surgery and RT, positive margins remain a significant predictor of local recurrence [15].
A 20 years single institution experience from Padua (Italy) showed in 22 patients affected by spermatic cord sarcoma a good prognosis: 5 years-cancer specific survival was 91.3%. Adjuvant therapy did not improved Cancer Specific Survival, but it is remarkable that all patients died of disease had positive surgical margins. Therefore, wide radical resection remains the mainstay of treatment, but in the contest of multidisciplinary management, RT could have a role for the local control of the disease. Preoperative RT is indicated in patients in whom conservative surgery cannot be performed at the time of diagnosis and postoperative RT is indicated if surgery show R1 or R2 margin [16].
Static or rotational intensity modulated technique improves tolerance, ensuring greater dose homogeneity and saving of organs at risk. A mono institutional experience showed a series of 5 patients treated between 2011 and 2014 with adjuvant intensity modulated radiotherapy (Arc-therapy) and reported no local recurrence and no grade 4 toxicity [17].
Bearing in mind these encouraging data, in consideration of the strong risk factors represented by local recurrences and the positive margins at the last surgery, we decided to deliver adjuvant RT with VMAT technique that improve tolerance and reduce toxicity.
Conclusion
In patients affected by pleomorphic leiomyosarcoma of the spermatic cord with a high risk of local recurrence, adjuvant RT should be considered.
This is a safe and well tolerated treatment especially with modern techniques that reduce acute and late toxicity. However we need a long-term follow-up to assess its efficacy on local control, in order to confirm therapeutic success in a patient who has already experienced many surgical treatments to remove local recurrences and also adjuvant CHT.
Declaration of conflicting interests: The authors declare that there is no conflict of interest.
References
- Rodriguez D, Barrisford GW, Sanchez A, Preston MA, Kreydin EI, Olumi AF. Primary spermatic cord tumors: Disease characteristics, prognostic factors, and treatment outcomes. Urol Oncol. 2014; 32: 52. e19-25
- Galosi AB, Scarpelli M, Mazzucchelli R, Lopez-Beltran A, Giustini L. Cheng L. et al. Adult primary paratesticular mesenchymal tumors with emphasis on a case presentation and discussion of spermatic cord leiomyosarcoma. Galosi et al. Diagnostic Pathology. 2014; 9: 90
- Rodriguez D, Olumi AF. Management of spermatic cord tumors: A rare urologic malignancy. Therapeutic Advances in Urology. 2012; 4: 325-334.
- Chalouhy C. Ruck JM, Moukarzel M, Jourdi R, Dagher N, Philosophe B. Current management of liposarcoma of the spermatic cord: A case report and review of the literature. Mol Clin Oncol. 2017; 6: 438-440
- Shaban Y, Elkbuli A, Kim D, Abdulla A, Boneva D, Mckenney M. et al. Dedifferentiated liposarcoma of the spermatic cord: Case Report and review of literature. Int J Surg Case Rep. 2020; 72: 418-422.
- International Commission on Radiation Units Measurement (ICRU). ICRU Report 83: Pres cribing, Recording and reporting photon-beam intensity-modulated radiation therapy (IMRT) N. Hodapp. Strahlentherapie und Onkologie. 2012; 188: 97-100.
- Anon. Common Terminology Criteria for adverse events v.4.0. Bethesda, MD: Us Department of Health and Human Services, National Institutes of Health, National Cancer institute. 2009.
- Moussa M, Chakra MA. Leiomyosarcoma of the spermatic cord: A case report and literature review. Int J Surg Case Rep. 2019; 57: 175-178
- Morozumi K, Kawasaki Y, Kaiho Y, Kawamorita N, Fujishima F, Watanabe M. et al. Dedifferentiated liposarcoma in the spermatic cord finally diagnosed at 7th resection of recurrence: a case report and bibliographic consideration. Case Rep Oncol. 2017; 10: 713-719.
- Frustaci S, Gherlinzoni F, De Paoli A, Bonetti M, Azzarelli A, Comandone A, et al. Adjuvant chemotherapy for adult soft tissue sarcomas of the extremities and girdles: results of the Italian randomized cooperative trial. J Clin Oncol. 2001; 19: 1238-47
- Fagundes MA, Zietman AL, Althausen AF, Coen JJ, Shipley W.U. The management of spermatic cord sarcoma. Cancer. 1996; 77: 1873-6.
- Coleman J, Brennan MF, Alektiar K, Russo P. Adult spermatic cord sarcomas: management and results. J. Annals of Surgical Oncology. 2003; 10: 669-675.
- Bachmann R, Rolinger J, Girotti P, Kopp HG, Heissner K, Amend B, et al. Liposarcoma of the Spermatic Cord: Impact of Final Surgical Intervention—An Institutional Experience. Int J Surg Oncol. 2016; 2016: 4785394.
- Murray KS, Vertosick EA, Spaliviero M, Mashni J.W.Jr, Sjoberg DD, et al. Importance of wide re-resection in adult spermatic cord sarcomas: report on oncologic outcomes at a single institution. J Surg Oncol. 2018; 117: 1464-1468.
- Khandekar MJ, Raut CP, Hornick JL, Wang Q, Alexander BM, Baldini EH. Paratesticular liposarcoma: Unusual patterns of recurrence and importance of margins. Ann Surg Oncol. 2013; 20: 2148-55.
- Lafrate M, Motterle G, Zaborra C, Leone N, Prayer-Galetti T, et al. Spermatic cord sarcoma: A 20 year single Institution experience. Front Surg. 2020; 7: 566408.
- Cerda T, Martin E, Truc G, Crehange G, Maingon P. Safety and efficacy of intensity-modulated radiotherapy in the management of spermatic cord sarcoma. Cancer/Radiotherapie. 2017; 16-20.