
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Breaks, bends and holes
Safeena Ansari Suhara; Sahana KS; Sushma Keshav; Prakash Saldanha; Diksha Shirodkar*
Department of Pediatrics, Yenepoya medical College, University Road, Deralakatte, Mangalore 575018, India.
*Corresponding Author: Diksha Shirodkar
Assistant Professor, Department of Pediatrics, Yenepoya Medical college, Yenepoya University Campus,
University Road, Deralakatte, Mangalore 575018,
India.
Email: diksha_shirodkar@yahoo.co.in
Received : July 17, 2021
Accepted : Sep 06, 2021
Published : Sep 10, 2021
Archived : www.jcimcr.org
Copyright : © Shirodkar D (2021).
Abstract
A 14 year old boy presented with lower limb deformities and bone pain since 8 months. He was severely wasted, stunted with tachypnea, pallor, genu-valgum, widened wrists and rachitic rosary. Workup revealed end-stage-renal-disease with metabolic acidosis, anaemia, hypocalcemia and secondary hyperparathyroidism. Scannogram of both lower limbs showed evidence of rickets, fractures and a lytic lesion in the lower end of the right femur suggestive of osteitis-fibrosa-cystica (OFC). The case depicts how one should evaluate a lytic bony lesion taking into consideration the complete clinical and biochemical picture and that OFC is not uncommon in adolescence in the presence of unchecked hyperparathyroidism. The child was treated with iron therapy, oral bicarbonate, oral vitamin D, erythropoietin and advised renal replacement therapy.
Citation: Suhara SA, Sahana KS, Keshav S, Saldanha P, Shirodkar D. Breaks, bends and holes. J Clin Images Med Case Rep. 2021; 2(5): 1306.
Case report
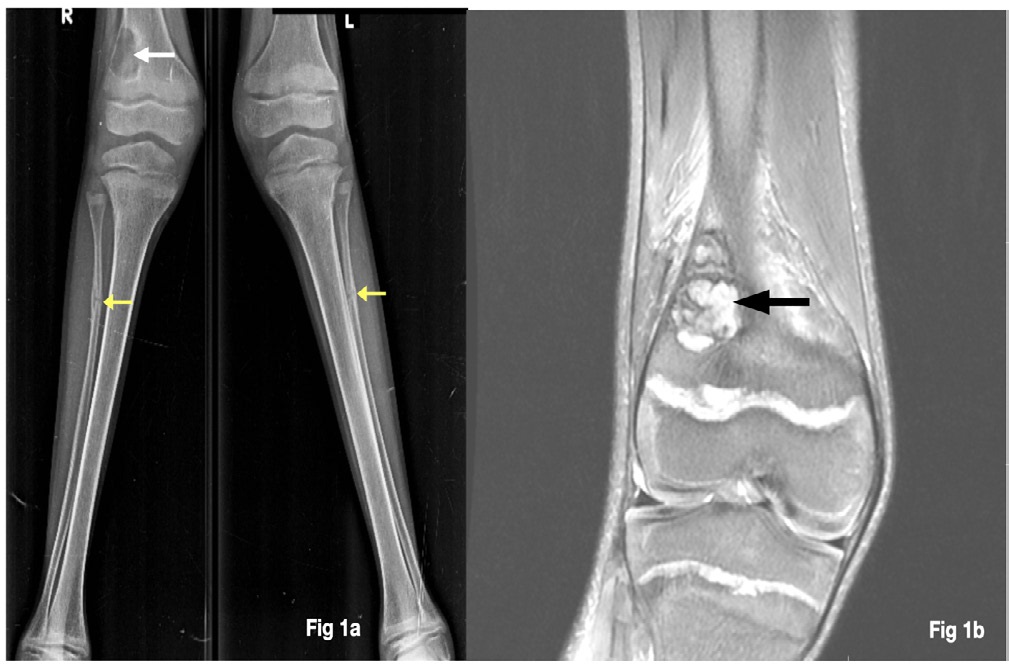
A 14 year old boy presented with lower limb deformities since 8 months. He was wasted (-4.28 z-score), stunted (-4.33 z-score) with tachypnea, pallor, genu-valgum, widened wrists and rachitic rosary. Investigations revealed End-Stage-RenalDisease (ESRD), metabolic acidosis, anaemia, hypocalcemia with secondary hyperparathyroidism and markedly-elevated alkaline phosphatase levels (Table 1). Scannogram of both lower limbs showed evidence of rickets, fractures and a lytic lesion in the lower end of the right femur (Figure 1a). Considering the background history and investigations, the diagnosis of Osteitis-Fibrosa-Cystica (OFC) was made. The MRI of the right knee showed a cystic lesion mostly a Brown tumor (Figure 1b). The child was treated with iron therapy, oral bicarbonate, oral vitamin D, erythropoietin and advised renal replacement therapy.
Table 1: Investigations of the patient.
Investigation |
Values (normal values for age) |
Hemoglobin g/dL |
6.5 (12-17) |
Peripheral smear |
Normocytic normochromic anemia |
Serum Corrected Calcium mg/dL |
6.5 (9-11) |
Serum Phosphate mg/dL |
4.3 (2.5-4.5) |
Serum Bicarbonate mmol/l |
8.3 (22-26) |
Serum potassium mmol/l |
2.7 (8.4-10.2) |
Serum Creatinine mg/dl |
4.4 (0.5-1) |
Blood Urea mg/dl |
65 (5-18) |
Alkaline phosphatase IU/l |
2518 (100-250) |
Vitamin D (25-OH-D) ng/ml |
20.7 (30-100) |
Parathyroid hormone pg/ml |
1550 IU/dL(15-60) |
Renal sonography |
Bilateral contracted kidneys for age |
eGFR ml/min |
12.6 ml/min (CKD stage 5) |
Discussion
The differential diagnosis of a lytic bony lesion would be broadly classified into benign/malignant bone tumors, infections, histiocytosis, aneurysmal/unicameral bone cyst and brown tumor. Investigations in this child revealed End-Stage-Renal-Disease (ESRD), metabolic acidosis, anaemia, hypocalcemia, secondary hyperparathyroidism and high alkaline phosphatase levels (Table 1). The diagnosis of Osteitis-Fibrosa-Cystica (OFC) was made which was confirmed by MRI of right knee (Figure 1a & 1b). The median incidence of ESRD in < 20 years-old is ~9 pmarp (per-million-of-age-related population) worldwide [1]. In pediatric Chronic-Kidney-Disease (CKD) disordered regulation of bone and mineral metabolism, secondary to abnormalities of calcium, phosphate, Parathyroid Hormone (PTH), calcitriol and fibroblast-growth-factor-23 leads to CKD-mineral-and-bone disorder [2] (CKD-MBD). OFC results from excessive PTH attaching to receptors on osteoblasts, resulting in over-expression of RANK-ligand-receptor activator, promoting osteoclast formation [3]. Activated osteoclasts cause bone resorption, corticalbone destruction and fibrous cysts formation. Osteoclast-likegiant-cells and vascularized fibrous tissue replace bone-marrow depositing hemosiderin causing Brown tumors [3]. Common sites include jaws, skull, pelvis, clavicle, ribs, femurs and spine [4] resulting in swelling, pathological fracture and bone pain. CT scan of OFC includes lytic/multilobular cystic changes as seen in our case [5]. This harps the fact that unchecked hyperparathyroidism needs a hawk’s-eye view as it can be seen as early as in adolescence and all bony lytic lesions shouldn’t be considered malignant without a thorough evaluation.
References
- Becherucci F, Roperto RM, Materassi M, Romagnani P. Chronic kidney disease in children. Clin Kidney J. 2016; 9: 583-591
- Hanudel MR, Salusky IB. Treatment of Pediatric Chronic Kidney Disease-Mineral and Bone Disorder. Current Osteoporosis Reports. 2017; 15: 198–206.
- Naji Rad S, Deluxe L. Osteitis Fibrosa Cystica. [Updated 2020 Jun 22]. In: Stat Pearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2021.
- Misiorowski W, Bilezikian JP. Osteitis Fibrosa Cystica. JBMR Plus. 2020; 4: e10403.
- Misiorowski W, Czajka-Oraniec I, Kochman M, Zgliczyński W, Bilezikian JP. Osteitis fibrosa cystica-a forgotten radiological feature of primary hyperparathyroidism. Endocrine. 2017; 58: 380- 385.