
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Sewing machine spool in cervical canal: Case report
AG Radhika1*; Natasha Tyagi1; Shilpa Singh2; Richa Agarwal1
1 Department of Obstetrics and Gynaecology, UCMS and GTB hospital, New Delhi,110095, India.
2 Department of Obstetrics and Gynaecology, KGMU, Lucknow, U.P., India.
*Corresponding Author: AG Radhika
Maternal and Child Health Block, 7th floor, Gynae
Office, GuruTeg Bahadur Hospital, Dilshad Garden,
Delhi, 110095, India.
Email: raradhikaag@gmail.com
Received : July 21, 2021
Accepted : Sep 07, 2021
Published : Sep 13, 2021
Archived : www.jcimcr.org
Copyright : © Radhika AG (2021).
Abstract
Background: Intentional placement or forgotten foreign bodies in the lower female genital tract have been reported. Patients may selfreport or may present with an array of symptoms including pelvic pain, vaginal discharge and vaginal bleeding.
Case: Ms X, 23 years old, presented to antenatal clinic at two months pregnancy with complaints of excessive discharge per vaginum. There was no bleeding or foul smell. She did not reveal any other significant history. On internal examination, uterus was 8 weeks size, and a nodular lesion was felt in the cervical canal. Transvaginal USG confirmed intra-uterine pregnancy but also aroused the suspicion of a foreign body in the cervix. At examination in the operation theatre, the spool of sewing machine was found imbedded in cervical canal. It was gently dislodged and removed. Procedure and post-operative period were uneventful. The history was then reviewed. It came to light that the spool had been inserted in the cervical canal to expedite conception, without her knowledge when the patient was examined by an untrained birth attendant.
Conclusion: Fear of infertility drives women to seek treatment from any source, as illustrated in this report. The spool inserted into the cervix was possibly to function as a “conduit” for the sperms
Keywords: foreign body; cervix; pregnancy; discharge.
Citation: Radhika AG, Tyagi N, Singh S, Agarwal R. Sewing machine spool in cervical canal: Case report. J Clin Images Med Case Rep. 2021; 2(5): 1307.
Introduction
Foreign bodies and chemicals have been frequently reported in the lower female genital tract. The objects may range from toys, tissue paper, household objects in children to tampons, condoms, menstrual cups and items used for sexual gratification in adult women. Elderly patients could be found to have retained medical devices such as pessaries. Patients may selfreport about inserting the foreign body or may present with an array of symptoms including pelvic pain, vaginal discharge, and vaginal bleeding. This interesting report gives details of finding the most unexpected object in cervical canal in a pregnant lady.
Case report
Ms X, 25 year, primigravida, presented at 8 weeks pregnancy to the antenatal clinic for her prenatal registration. Other than increased vaginal discharge, she was at low risk. There was no foul smell or unusual bleeding associated with the discharge. Physical examination was unremarkable. On speculum examination, vagina and cervix were smeared with non–specific discharge. Cervix was irregular, hypertrophied, hyperaemic and bled on touch. At vaginal examination a hard fixed nodular non-tender mass measuring 1x1 cm was felt in the cervical canal just inside the external os. The gravid uterus was retroverted corresponding to 8 weeks size.
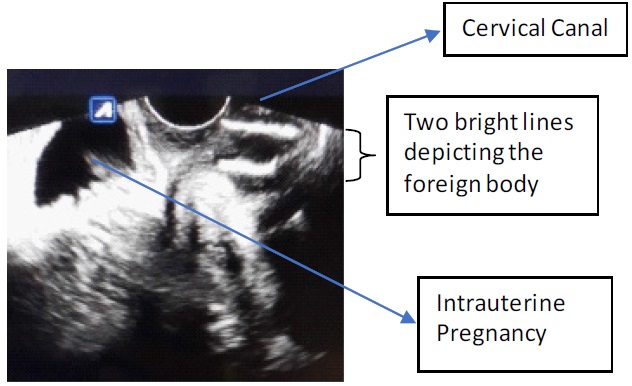
Transvaginal ultrasound revealed 2 hyperechoic parallel lines in the cervical canal (Figure 1). These measured 1.5 and 1 cm respectively, with posterior attenuation shadow, and were placed about 1 cm below internal os. An intrauterine live fetus of 8 wks was also noted. The history was now reviewed but she insisted on not having inserted any foreign body or having undergone any other procedure/instrumentation.
After consent, examination under anaesthesia was undertaken under regional block. On digital palpation, a metallic object was found in the cervical canal. This was extracted with Allis forceps. It was found to be a bobbin (spool) used in sewing machines (Figure 2). There was no bleeding or complication during or post procedure. She was well and devoid of any complaints at her follow up visit a week after discharge from hospital.

The patient later revealed that she had visited a local untrained birth attendant “dai” few months back at the insistence of her mother in law for expediting conception. This Dai had examined her internally though the patient had no recollection of any foreign body being inserted into her vagina.
Discussion
Foreign bodies have been frequently reported in the female genital tract in both low and high income countries alike. Reasons for insertion of foreign body into genitals range from curiosity in children to forgotten pessaries and tampons in adults [1,2]. Sexual abuse, need for sexual gratification, contraception or induction of illegal abortion have been the few reasons identified in women of reproductive age.
Several cases of foreign bodies with pregnancies have been described in literature. Aime Paul Heineck described the case of a 25 year old women who had a self retaining uterine tube introduced into the uterus for the purpose of preventing conception but she, later presented to the emergency with incomplete abortion [3]. In India introduction of foreign bodies in the female genital tract for inducing abortion are known. These could vary from bamboo sticks, crochet hooks, cannula, knitting needle, hair pin, arsenic or lead paste [4]. The interesting point in the present case is that she apparently conceived with the metallic foreign body in cervical canal.
Kevin R. Emge reported a case of a 28 week pregnant lady who presented with an orange in her vagina after a coital act in intoxicated state which had to be removed with Tucker-Mc lane forceps [5]. Another case report is of that of a woman who was an illicit drug user and presented at 23 weeks pregnancy with a sewing needle stuck in her abdominal wall above the fascia. Attempts to remove it under local anaesthesia caused it to penetrate deeper into the myometrium. Second attempt to remove it via a laparotomy also failed. A caesarean section was done at term when the needle was found imbedded in placenta [6]. Chawla et al discussed a case where a full term pregnant lady presented in labour with cervical dystocia. At caesarean section a foreign body was found extending from the cervix upto the lower uterine segment and a plastic cap of 5 × 3 cm was removed surgically. She later gave history of sexual violence by her husband who suspected infidelity [7].
Symptoms due to the foreign body depend on its chemical composition, shape, and time elapsed since insertion in the vagina. The presenting complaints include pelvic pain, foul smelling discharge and bleeding per vaginum. Leakage of urine or faeces per vaginum due to the formation of a vesicovaginal or rectovaginal fistula are rare. Singh et al described the case of a 14 year old girl who came with urine leakage per vaginum and a plastic cap was found in her vagina which was penetrating into the bladder trigone [8]. Non remitting vaginal discharge despite multiple antimicrobials should raise suspicion of a foreign body [9].
Evaluation of a suspected foreign body in lower genital tract includes speculum and vaginal examinations, plain radiography or USG as the basic investigations. The sensitivity and specificity of transabdominal/transperineal ultrasound ranges from 57- 83% and 53-95% for the detection of soft tissue foreign bodies [1,10]. Plain X ray has a poor detection rate of only 23% because it can detect only radio-opaque materials i.e. aluminium, glass, wooden and plastic objects remain undetected [11]. X rays are avoided in pregnancy. MRI can be used to detect those bodies which cannot be detected by other modalities [12]. Vaginoscopy with a 4 mm hysteroscope may be used for the diagnosis and treatment of foreign bodies in children [13].
In the setting of a foreign body found incarcerated in the cervix, anesthesia is recommended for its removal, as was done in the present case. If invasion into surrounding anatomical structures is present, repair procedures in same or next sitting may be necessary [14].
Conflicts of interest: The authors declare that there is no conflicts of interest regarding the publication of this article.
This report did not receive funding.
References
- Yang X, Sun L, Ye J, Li X, Tao R. Ultrasonography in Detection of Vaginal Foreign Bodies in Girls: A Retrospective Study. J Pediatr Adolesc Gynecol. 2017; 30: 620-625.
- Anderson J, Paterek E. StatPearls . StatPearls Publishing; Treasure Island (FL): Aug 10, 2020. Flea Bites.
- Heineck AP. Removal of a foreign body introduced into the cervical canal to prevent conception. JAMA. 1913; 61: 868.
- Bhatnagar PK. Unusual foreign bodies in uterine cavity: A Report On Two Cases. Med J Armed Forces India. 1999; 55: 265-266.
- Emge KR. Vaginal foreign body extraction by forceps: a case report. Am J Obstet Gynecol. 1992; 167: 514-5.
- Glover MM, Neiger R, Sonek JD, Croom CS, McKenna DS, et al. Pregnancy Complicated by an Intrauterine Foreign Body. Journal of Ultrasound in Medicine. 2008; 27: 493-495.
- Chawla S, Singla A, Chandra C, Falodia S. Forgotten Vaginal Foreign Body Presenting as Cervical Dystocia. J Clin Diagn Res. 2016; 10: QD01-2.
- Singh RR, Ghotra HS, Garg R, Kaur R. An unusual foreign body in the vagina producing vesicovaginal fistula. J Dent Med Sci. 2013; 6: 72-73.
- Smith YR, Berman DR, Quint EH. Premenarchal vaginal discharge: findings of procedures to rule out foreign bodies. J PediatrAdolesc Gynecol. 2002; 15: 227-30.
- Davis J, Czerniski B, Au A, et al. Diagnostic Accuracy of Ultrasonography in Retained Soft Tissue Foreign Bodies: A Systematic Review and Meta-analysis. Acad Emerg Med. 2015; 22: 777-87.
- Anderson J, Paterek E. Vaginal Foreign Body Evaluation and Treatment. [Updated 2021 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 202.
- Nwosu EC, Rao S, Igweike C, Hamed H. Foreign objects of long duration in the adult vagina. Journal of Obstetrics and Gynaecology. 2005; 25: 7,737-739.
- Golan A, Lurie S, Sagiv R, Glezerman M. Continuous flow vaginoscopy in children and adolescents. J Am Assoc GynecolLaparosc. 2000; 7: 526-8.
- Chopra S, Singh Y, Magon N. A Case of Intravaginal Foreign Body. Med J Armed Forces India. 2010; 66: 266-8.