
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A rare case of mobile ball-like mass in right atrium associated with dilated cardiomyopathy
Jing Dong1; Yiqun Gao2; Shunji Liang2; Guorong Deng1; Jian Zhang2; Yunzhi Wang2; Li Liu1,2*
1 Department of Cardiology, The Second Affiliated Hospital of Shaanxi University of Chinese Medicine, Xianyang, Shaanxi Province, China.
2 Department of Cardiology, The Affiliated Zhongshan Hospital of Dalian University, Dalian, Liaoning Province, China.
*Corresponding Author: Li Liu
The Second Affiliated Hospital of Shaanxi University
of Chinese Medicine, Xianyang, Shaanxi Province,
China.
Email: lbeilliun@yahoo.com
Received : July 21, 2021
Accepted : Sep 07, 2021
Published : Sep 13, 2021
Archived : www.jcimcr.org
Copyright : © Liu L (2021).
Abstract
Mobile thrombus in the Right Atrium (RA) is a rare condition. Here, we described a case of a 59-year-old male who presented in emergency room with complaints of progressively worsening dyspnea for 7 years. He was normotensive, had elevated jugular venous pressure and clear lungs. ECG revealed ventricular tachycardia. After successfully electrical defibrillation, an urgent 2D echocardiogram was obtained and revealed the enlargement of all heart chambers and a ball-like, mobile mass in the right atrium. An emergent CT scan revealed no sign of pulmonary embolism. Based on morphological features on echocardiogram, we highly suspected it as RA thrombus. The patient was treated with anticoagulant therapy comprising of low molecular heparin and warfarin since he rejected surgical treatment. Repeat echocardiogram was performed 7 days after anticoagulant therapy and showed disappearance of the RA mass. He was subsequently maintained on warfarin (INR=2.4- 3.0) and other medications for heart failure. The patient was followed up as outpatient and kept in good clinical condition. We concluded that early recognition of this rare situation and prompt management can help in preventing life-threatening complications, and anticoagulant therapy was a therapeutic option for RA thrombus.
Keywords: right atrial mass; thrombus; echocardiogram; anticoagulation.
Citation: Dong J, Gao Y, Liang S, Deng G, Zhang J, et al. A rare case of mobile ball-like mass in right atrium associated with dilated cardiomyopathy. J Clin Images Med Case Rep. 2021; 2(5): 1309.
Introduction
Although intracardiac masses are commonly encountered in clinical setting, a mass in the Right Atrial (RA) cavity is relatively rare. The masses usually include thrombi, vegetations, metastatic tumors, myxomas, inflammatory granuloma, etc [1,2]. It’s very challenging to differentiate the nature of masses therefore provide appropriate management to prevent the possible complications. The definite diagnosis can be only established by surgical resection and pathology, however certain morphological features on imaging studies can help in differential diagnosis. We hereby describe a case of a mobile ball-like RA thrombus diagnosed with Transthoracic Echocardiography (TTE) and the patient was treated successfully with anticoagulation therapy without any complications.
Case presentation
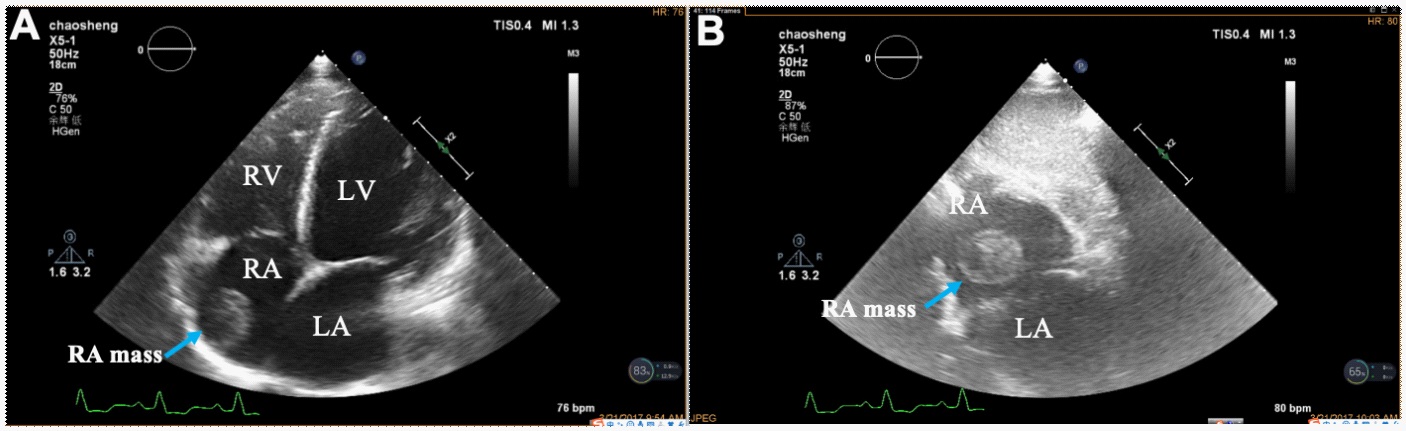
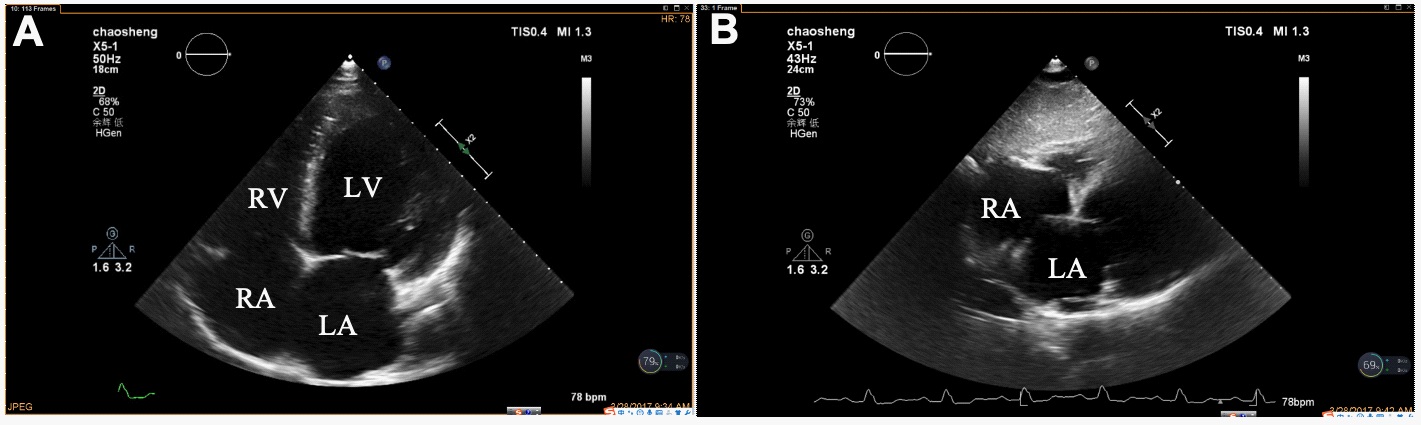
A 59-year-old male presented in emergency room with complaints of progressive dyspnea for 7 years and worsening for 3 days. His medical history was significant for hypertension but well-controlled with anti-hypertensive drugs. Denied any known liver, kidney diseases and diabetes. On physical examination, he was normotensive, had elevated jugular venous pressure and clear lungs. Emergency ECG revealed ventricular tachycardia (HR=135bpm) without ST-T changes. Electrical defibrillation was performed and restored as sinus rhythm (HR=95 bpm). Pitting lower limb edema was noticed. His blood analysis was as follows: hemoglobin 13.5 g/dL, leukocyte count 7.9×109 /uL, platelet count 59,000/uL, high-sensitivity troponin protein I 0.303ng/ ml, CK-MB 7.3ng/ml, Lactate dehydrogenase (LDH) 10750U/L, NT-proBNP 22702pg/ml, serum creatinine 438.1mmol/L, BUN 22.54mmol/L, eGFR=12.12ml/min*1.73m2 . Liver biochemistry tests were as followings: Alanine aminotransferase (ALT) 3518 U/L, aspartate Aminotransferase (AST) 4267 U/L, cholinesterase 3406.7 U/L, HBsAg was negative. Blood gas analysis: PH=7.072, PO2 99.70 mmHg, PCO2 19.60 mmHg, actual bicarbonate 5.6 mmol/L, standard bicarbonate 8.6 mmol/L. Coagulation tests: PT 57.1s, APTT 58.0s, D-Dimer 7.97 ug/ml, FDP 94.5 ug/ml. Serum potassium 6.6 mmol/L, serum sodium 130.7 mmol/L, serum chlorine 89.4 mmol/L. An urgent 2D echocardiogram was obtained and revealed the enlargement of all heart chambers (left ventricular diastolic diameter 75 mm). Left ventricular ejection fraction (LV EF) 25%. A mobile ball-like mass was noticed in the right atrium (Figure 1). An emergent CT scan was ordered and revealed no sign of pulmonary emboli. Ultrasound-Doppler didn’t detect any sign of bilateral lower limb Deep Venous Thrombus (DVT). Patient hospitalized and received treatment for heart failure. Since the high risk of pulmonary embolism, surgical management of RA mass was recommended but rejected by the patient. Given the morphological features of this mobile RA mass, we highly suspected it as RA thrombus. The patient was then treated with anticoagulant therapy comprising of low molecular heparin and warfarin after obtaining written informed consent from the patient. Repeat TTE was performed 7 days later and showed disappearance of the mobile RA mass, suggesting complete thrombus resolution (Figure 2). He was subsequently maintained on warfarin (maintaining INR 2.4~3.0) and other medications for heart failure with significant improvement of symptoms. The patient did well during the follow-up period.
Written consent was obtained from the patient prior to disclose his information and images. The case report was conducted in accordance with the principles of the Declaration of Helsinki.
Discussion
Atrial thrombi are more commonly seen in left atrium (including left atrial appendage) and left ventricle, and usually accompanied by structural heart diseases or other predisposing conditions, such as acute myocardial infarction, left ventricular aneurysm, cardiomyopathies and myocarditis, valve disease, atrial fibrillation/atrial flutter [3-5]. Right atrial thrombi are relatively rare but if present, there are significant morbidity and mortality due to massive pulmonary embolism or paradoxical embolism [6,7]. The differential diagnosis of right atrial thrombi includes tumors (most are metastatic tumors), myxoma, vegetations, inflammatory granuloma, et al [1,2,8,9]. 2D echocardiography (TTE or Transesophageal Echocardiogram (TEE)) is the most easy-use and feasible tool for detection of RA masses in clinical setting, which can provide the essential information about the mass including morphology, echogenicity, mobility, with/without stalk. However, sometimes it is difficult to differentiate one mass from another. In our case, the major differentiation is myoma, they usually have similar echocardiographic features. Given the RA mass appears as a mobile, ball-like, medium echogenicity and no stalk in this case, we highly recommended the diagnosis of RA thrombus, taking consideration with the patient’s history.
The early and accurate diagnosis of RA thrombi is very important because of high risk of pulmonary embolism. Study has indicated that it is associated with increased mortality of more than 40% if mobile RA thrombus is present [7]. Current therapeutic options for RA thrombi include thrombolysis, surgical embolectomy or percutaneous embolectomy, but the most effective therapy remains unknown. In our case, we promptly started anticoagulation therapy with low molecular heparin and warfarin since the patient rejected surgical treatment. The patient was monitored during anticoagulation therapy. The RA mass was found to disappear at 7 days after treatment without any complications, which indirectly confirmed our diagnosis. To our knowledge, this is the first report of successful anticoagulation therapy with warfarin for RA thrombus in such short treatment period. Based on the case described in the present report, anticoagulation therapy can be one of reasonable options for the treatment of RA thrombi. Our conclusion is that early recognition of RA thrombus is very important due to extreme instability of mobile thrombus and prompt treatment can prevent life-threatening complications. Anticoagulation therapy is a reasonable therapeutic option.
Acknowledgements: We thank all the doctors and medical staff who were involved in the treatment of this patient.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests: The Authors declare that there is no conflict of interest.
Author contributions: JD wrote the first draft of this manuscript. YG, GD, JZ, SL and YW contributed to data collection, JD and LL contributed to data interpretation and analysis. LL has made critical revisions and all authors reviewed and approved the final manuscript.
Ethical approval: The requirement for ethical approval was waived by the ethical committee of the Second Affiliated Hospital of Shaanxi University of Chinese University.
Informed consent: The patient gave written consent for the publication of this report.
Disclosure and ethics: As a requirement of publication, authors have provided to the publisher signed confirmation of compliance with legal and ethical obligations including, but not limited to, the following:
Authorships, conflicts of interest, privacy and confidentiality, and protection of human research subject. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria.
The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. Written consent was obtained from the patient prior to disclose his information. The case report was conducted in accordance with the principles of the Declaration of Helsinki.
References
- Felner JM, Churchwell AL, Murphy DA. Right atrial thromboemboli: Clinical, echocardiographic and pathophysiologic manifestations. J Am Coll Cardiol. 1984; 2013: 1041–50.
- Lotto AA, Earl UM, Owens WA. Right atrial mass: thrombus, myxoma, or cardiac papillary fibroelastoma? J Thorac Cardiovasc Surg. 2006; 132: 159–60.
- Restrepo CS, Largoza A, Lemos DF, et al. MR imaging findings of benign cardiac tumors. Curr Probl Diagn Radiol. 2005; 34: 12–21.
- Finlayson GA. Right heart thrombi: consider the cause. Can J Cardiol. 2008; 24: 888.
- Farfel Z, Schechter M, Vered Z, Rath S, Goor D, et al. Review of echocardiographically diagnosed right heart entrapment of pulmonary emboli-in-transit with emphasis on management. Am Heart J. 1987; 113: 171–78.
- Basarici I, Yilmaz H, Demir I, et al. Imminent pulmonary embolism: a fatal mobile right atrial thrombus. Int J Cardiovasc Imaging. 2006; 2013: 55–8.
- Chapoutot L, Tassigny C, Nazeyrollas P, et al. Pulmonary embolism and thrombi of the right heart. Arch Mal Coeur Vaiss. 1995; 2013: 1723–8.
- Tomlinson JS, El-Gaaly M, Khan S, Papouchado M. Right atrial mass: a challenging diagnosis. BMJ Case Rep. 2020; 13: e235715.
- Martha Alehli Rangel-Herna´ndez, Alberto Aranda-Fraustro, Gabriela Melendez-Ramirez, Nilda Espı´nola-Zavaleta. Misdiagnosis for right atrial mass: a case report. European Heart Journal - Case Reports. 2018; 2: 1–6.