
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An obstructive tongue neurofibroma
Gama R*; Sousa M; Castro F; Condé A
Department of Otorhinolaryngology and Head and Neck Surgery of Vila Nova de Gaia/Espinho Hospital Center
*Corresponding Author: Rita Gama
Department of Otorhinolaryngology and Head and
Neck Surgery, Hospital Center of Vila Nova de Gaia
and Espinho E.P.E., Rua Conceição Fernandes 1079,
4434-502 Vila Nova de Gaia, Portugal.
Email: ritarocha@campus.ul.pt
Received : July 29, 2021
Accepted : Sep 08, 2021
Published : Sep 14, 2021
Archived : www.jcimcr.org
Copyright : © Gama R (2021).
Abstract
Neurofibromatosis type 1 (NF1) is an autosomal dominant disorder characterized by multiple manifestations, including the presence of neurofibromas. These benign lesions can potentially affect every site of the body; its location in the head and neck region is not uncommon, but the oral cavity, and specially the tongue, are rarely affected.
We aim to present a case of a giant recurrent neurofibroma of the tongue in a NF1 patient, conditiong obstructive symptoms, as well as to ouline its successful treatment with topical mitomycin-C as an adjuvant therapy to surgical ressection.
Keywords: neurofibromatosis; neurofibroma; recurrence; airway obstruction.
Citation: Gama R, Sousa M, Castro F, Condé A. An obstructive tongue neurofibroma. J Clin Images Med Case Rep. 2021; 2(5): 1312.
Introduction
Neurofibromatosis type 1 (NF1), also known as von Recklinghausen’s neurofibromatosis, is an autosomal dominant disorder caused by a defect on chromosome 17. The manifestations of NF1 result from the decreased production of a tumour supressor protein, being the most common: multiple neurofibromas, café-au-lait spots, intertriginous freckles, Lisch nodules, central nervous system tumors, and skeletal abnormalities [1]. Neurofibromas can potentially affect every site of the body; its location in the head and neck region is not uncommon, but the oral cavity, and specially the tongue, are rarely affected [2,3]. There is no treatment for NF1, and the lesions should be activelly controlled, being surgical resection indicated when functional or aesthetic impairment is associated [1]. Neurofibromas may be difficult to approach surgically, often recurring after resection because of residual tumor cell collections deep in soft tissues.
The topical use of Mitomycin-C, an antitumor antibiotic that decreases fibroblast activity, has been successfully implemented in several conditions, such as bladder cancer, conjunctival and corneal squamous cell carcinoma, laryngotracheal stenosis and to prevent keloid scar formation [4]. To the best of our knowelgde, there are no reports describing the use of topical Mitomycin-C for the specific indication we present.
We describe a case of a neurofibroma of the tongue in a NF1 patient, which always recurred after multiple surgical interventions, successfully treated with topical mitomycin-C as an adjuvant therapy to surgical resection.
Case report
A 55-year-old man, previously diagnosed with NF1, presented with complaints of progressive oral discomfort, speech impairment, swallowing and breathing difficulties, associated with night snoring and sleep apnoea.
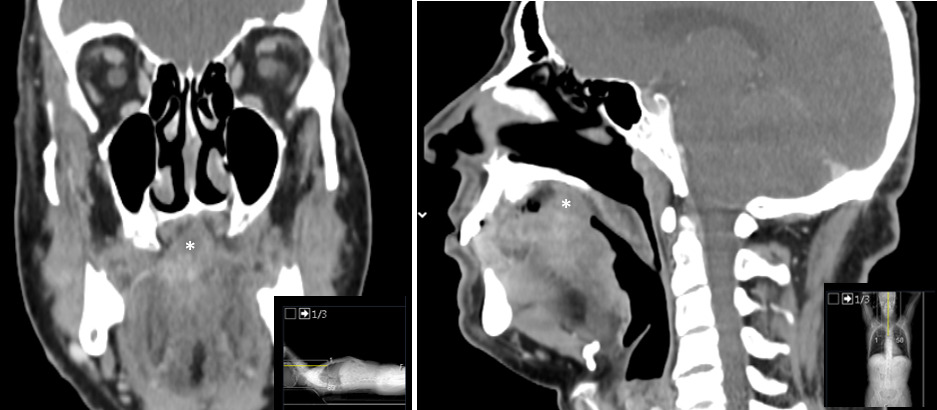
On examination, he had a mucosal-covered, painless and irregular mass located in the transition between the anterior two thirds and the posterior third of the tongue, that had grown gradually over the past 7 months (Figure 1). He had undergone multiple previous surgical resections of this tongue neurofibroma, always with recurrence of the lesion after just a few months, and this time, the lesion was bigger than ever. There were no lesions in the pharynx, larynx or trachea. The Computed Tomography (CT) scan showed an irregular area with heterogeneous uptake of contrast in the location described, measuring approximately 25 x 19 mm (Figure 2).

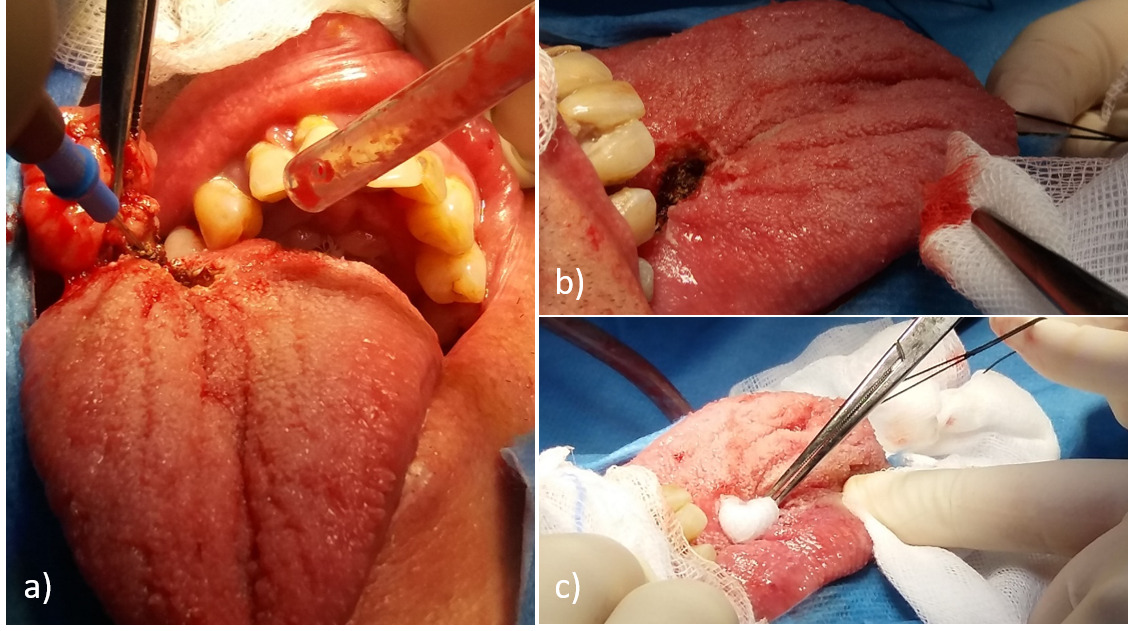
The presence of dysphagia, sleep apnoea and the eminent risk of airway obstruction made another resection necessary. Under general anesthesia, the tumor was approached and completely excised intraorally, this time followed by topical application of mitomycin-C (0,4mg/mL) over the tumor bed, through a gauze soaked in the drug, removed after 5 minutes (Figure 3). The area was then suction-irrigated thoroughly with 30 mL of distilled water, and sutured with vycril 3.0. After surgery, the movements of the tongue were preserved, and the patient immediately improved communication and swallowing. Histological analysis showed features of neurofibroma, including slender spindle cells arranged against a variable collagenous background, alongside small nerve fibers and axons. The patient is free of recurrence after 3 years of follow-up.
Mitomycin-C is an antibiotic isolated from Streptomyces caespitosus. It undergoes metabolic activation to become an alkylating agent that is cytotoxic to both proliferating and nonproliferating cells. It has proven to be an antimetabolic agent which inhibits fibroblasts proliferation by preventing DNA synthesis [4]. Most of the studies reporting the topical use of this drug showed that the benefits outweighed the risks, even in the airway region [5] Thus, under patient consent, we tried the topical application of mitomycin-C in this case of recurrent tongue neurofibroma taking into account the known histological composition of neurofibroma - neoplastic neuronal cells and fibroblasts -, and considerating the antineoplastic and antifibroblastic activity of mitomycin-C. Reported complications of its topical use include local irritation, hyperaemia and allergy. No systemic adverse effects have been described [4,5].
Our successful experience suggests that Mitomycin-C can be a safe and promising adjuvant therapy to surgical resection of difficult-to-remove and/or recurrent neurofibromas, due to its effectiveness in reducing the rate of recurrence.
We aim to alert ENT surgeons and family doctors about the possibility of this diagnosis, as a rare but potentially life-threatening entity, that should be included in the differential diagnosis of an oral mass.
Conclusions
This report describes a potentially life-threatening obstructive neurofibroma lesion which, although very rare, should be included in the differential diagnosis of an oral mass, especially in NF1 patients. We also outline its successful treatment with topical mitomycin-C as an adjuvant therapy to surgical ressection.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Cimino PJ GD. Neurofibromatosis type 1. Handb Clin Neurol. 2018; 148: 799-811.
- MR Bongiorno, G Pistone MA. Manifestations of the tongue in Neurofibromatosis type 1. Oral Dis. 2006: 125-129.
- Alotaiby FM, Fitzpatrick S, Upadhyaya J, Islam MN, Cohen D. Demographic , Clinical and Histopathological Features of Oral Neural Neoplasms : A Retrospective Study. Head Neck Pathol. 2019; 13: 208-214.
- Tomasz M. Mitomycin C: Small, fast and deadly (but very selective). Chem Biol. 1995; 2: 575-579.
- Queiroga TLO, Cataneo DC, Martins RHG, Reis TA. Mitomycin C in the Endoscopic Treatment of Laryngotracheal Stenosis : Systematic Review and Proportional Meta-Analysis. Int Arch Otorhinolaryngol. 2020: 112-123.