
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A rare cause of bladder outlet obstruction: Vesical diverticular calculus
Vivek Rajdev
Department of Medicine, No: 9,10, Street-01, Near Columbus Public School, Model Colony, India.
*Corresponding Author: Vivek Rajdev
Department of Medicine, No: 9,10, Street-01, Near
Columbus Public School, Model Colony, India.
Email: vivekrajdev.43@gmail.com
Received : Aug 18, 2021
Accepted : Sep 14, 2021
Published : Sep 21, 2021
Archived : www.jcimcr.org
Copyright : © Rajdev V (2021).
Abstract
Vesical diverticula are herniations of the bladder mucosa and submucosa through the muscular wall of the bladder. A calculus in diverticulum is an unusual finding. It is usually secondary to bladder outlet obstruction [1]. The patient typically presents with lower urinary tract symptoms, lower abdominal pain or abdominal distention. The present case is a 64-year-old male with a giant vesical diverticulum calculus. Cystolithotomy was done with primary closure of bladder, with repair of bladder diverticulum. Post-operatively, he recovered well with improved lower urinary tract function.
Keywords: vesical diverticulum; diverticular calculus; bladder outlet obstruction.
Citation: Rajdev V. A rare cause of bladder outlet obstruction: Vesical diverticular calculus . J Clin Images Med Case Rep. 2021; 2(5): 1320.
Introduction
Vesical diverticula are herniations of the bladder mucosa and submucosa through the muscular propria of the bladder [2]. They are often small and asymptomatic; most are discovered incidentally during an examination for other reasons.
Most bladder diverticula require no treatment, although some may cause significant morbidity. Complications include recurrent infections (13-73%), stone formation (5-16%), tumor development (3-10%), ureteral obstruction (8%) and urinary retention [3].
This is a case report of calculus in bladder diverticulum presenting as bladder outlet obstruction.
Case report
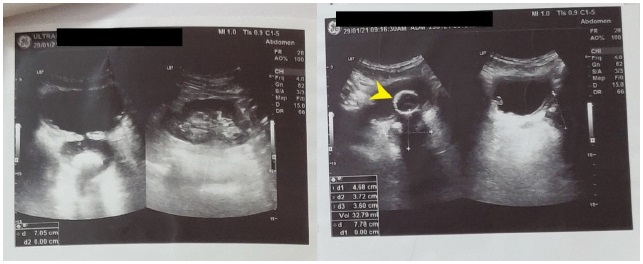
A 64 years old male, with no co-morbidity, presented with complaints of pain in lower abdomen, increased frequency of micturition and poor stream. On examination, patient had palpable urinary bladder. On digital rectal examination, patient had normal perianal sensation, grade 1 prostatomegaly with benign consistency. Patient was catheterized for chronic urinary retention. Ultrasound pelvis suggested urinary bladder stone with posterolateral diverticulum in urinary bladder (Figure 1). On cystoscopy, grade 1 prostate was present with, high bladder neck with urinary bladder diverticulum.
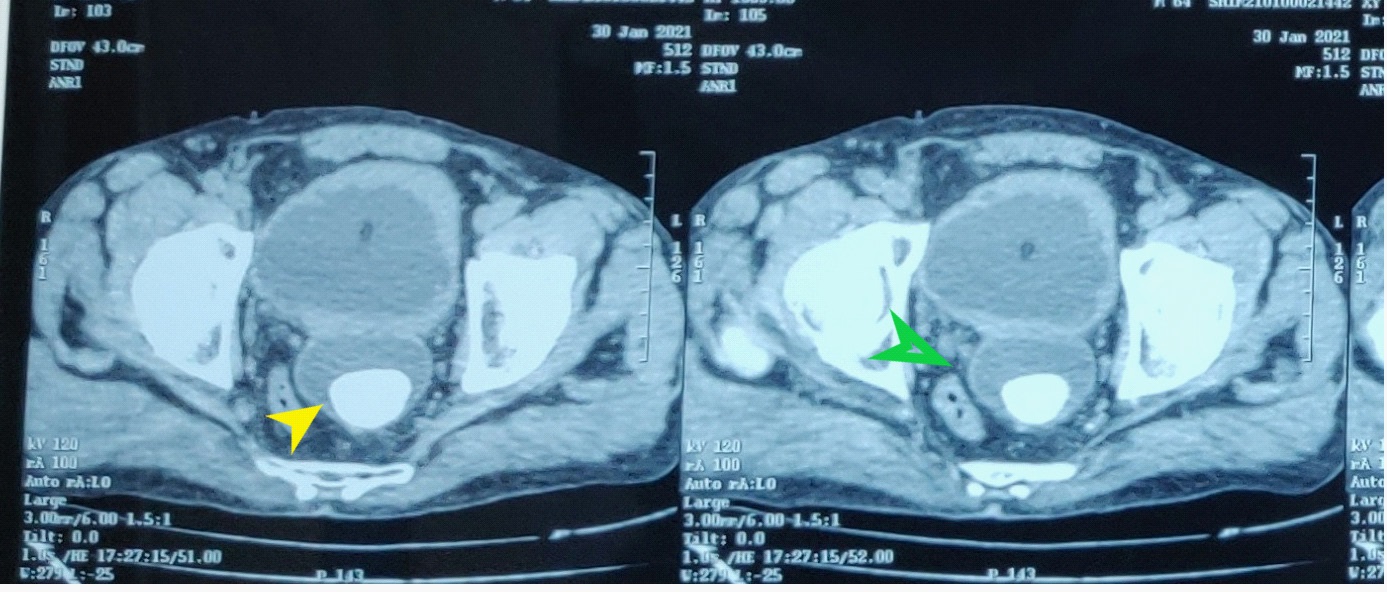
NCCT KUB was done which was suggestive of cystitis with bladder trabeculations with multiple diverticula, with a diverticulum of 6 x 4.5 cm posterior to bladder with 37 x 25 mm calculus present in diverticulum (Figure 2). Patient was planned for TUIP and cystolithotomy.
TUIP with excision of diverticulum was done. On endoscopy 5 and 7 o’clock bladder neck incision were given. Urinary bladder was trabeculated with one large diverticulum with narrow neck. A narrow-mouthed diverticulum was present in the interureteric region posteriorly in trigone of bladder. Open diverticulectomy was done with retrieval of bladder calculus with repair of bladder wall.
Post-operatively, patient underwent successful trail of void on 21th POD.
Discussion
Bladder diverticula are small to large herniation of bladder urothelium through muscularis propria of bladder wall. Its wall is composed of mucosa, lamina propria and adventitia. A fibrous capsule is often present that forms a surgical plane for excision. They may occur in adults or children, but around 90% of diverticula occur in adults. They are more common in males compares to females, with a ratio of 9:1 [4]. They can be congenital or acquired. Congenital occur in <10 years old, more in males, are posterolateral to urethral orifice, solitary, often associated with VUR. Congenital weakness of detrusor muscle is thought to be primary causal factor. They present as acute UTI due to stasis of urine [5]. Rare presentations are enuresis, pyelonephritis, acute retention and stones. They are not associated with malignancy risk.
Acquired or secondary diverticula occur most commonly in the setting of bladder outlet obstruction and neurogenic vesicourethral dysfunction. They are also located mostly at ureterovesical hiatus. Mostly are seen in males after age of 60 years as a result of bladder outlet obstruction due to prostatic enlargement. Around 70% are associated with BPH. They are mostly multiple, associated with bladder trabeculations [6]. If the diverticulum is located superolateral to urethral orifice, in the setting of neuropathic bladder and VUR, it is termed as Hutch diverticulum [7].
Bladder diverticulum may also be iatrogenic, inadequate closure of bladder wall after cystostomy. They are usually asymptomatic and mostly discovered incidentally during investigation of lower urinary tract symptoms, hematuria or infection. The finding of bladder diverticulum in an adult should prompt further evaluation for bladder outlet obstruction or neuropathic bladder dysfunction [8].
5-16 % of bladder diverticula are associated with calculi formation within the diverticula. They may present with hematuria, lower abdominal pain and other symptoms of LUTS.
Diagnostic evaluation include blood and urine tests, ultrasound, cystourethrography, CT urography and cystoscopy.
Indications for surgery are persistent or recurrent urinary infection, presence of stone in the diverticulum or associated malignancy, lower urinary tract symptoms, voiding symptoms or VUR, resulting from diverticulum, stone or ureteral obstruction [9]. Treatment includes endoscopic or open surgery. The cause of obstruction should be treated before or along with diverticulum therapy. Management includes transurethral resection of small prostate and incision of a small diverticulum, or open prostate enucleation and diverticulectomy for a large prostate and diverticulum.
Laparoscopic or open surgery has been recommended for large stones. For small or moderate calculi, endosurgical procedures such as cystolithotripsy have added advantage as they can be combined with treatment of bladder outlet obstruction. Studies have recommended to avoid use of ESWL if stone is in diverticula or stuck to mucosa. In the present case, the small prostate was treated by endoscopic resection followed by open cystolithotomy for diverticular calculus [10].
Conclusion
A vesical diverticulum calculus is a rare entity, that occurs in the setting of bladder outlet obstruction. Treatment is mandatory and includes extraction of calculus with correction of cause of bladder outlet obstruction.
References
- Urotoday Int J. 2010; 3.
- Kumar S, Jayant K, Barapatra Y, Rani J, Agrawal S. Giant Urinary Bladder Diverticula presenting as Epigastric Mass and Dyspepsia. Nephrourol Mon. 2014; 6: e18918.
- Iscaife A, Dos Anjos G, Barbosa C Neto, Nahas WC, Srougi M, et al. The role of bladder diverticula in the prevalence of acute urinary retention in patients with BPH who are candidates to surgery. Int Braz J Urol. 2018; 44: 765-770.
- Shakeri, Saeed & AR, Rasekhi & Yazdani, Melika & Kheradpezhouh, Ehsan. The incidence of diverticula of urinary bladder in patients with benign prostatic hypertrophy and the comparison between cystoscopy and cystography in detecting bladder diverticula. Iranian Red Crescent Medical Journal. 2007; 9.
- Vaddi S, Pogula V, Devraj R, Sreedhar A. Congenital bladder diverticulum - a rare adult presentation. J Surg Case Rep. 2011; 2011: 8.
- Yovchevski P, Kostov K. Acquired nonobstructive urinary bladder diverticulum: a case report. Cases J. 2009; 2: 36.
- JA Hutch. Vesico-ureteral refux in the paraplegic: cause and correction. Te Journal of Urology. 1952; 68: 457–467.
- Senel, Samet & Kizilkan, Yalcin & Bulut, Suleyman & Aktas, Binhan. Giant bladder diverticulum: A case report and review of the literature. 2002.
- Afshar K, Malek R, Bakhshi M, et al. Should the presence of congenital para-ureteral diverticulum affect the management of vesicoureteral reflux? J Urol. 2005; 174: 1590-1593.
- Gu S, You Z, Huang Y, Lu Y, He C, Cai X, Zhou X. Minimally invasive percutaneous cystostomy with ureteroscopic pneumatic lithotripsy for calculus in bladder diverticula. Experimental and Therapeutic Medicine. 2013; 5.