
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Life-threatening secondary infection in a patient with Covid-19 pneumonia treated with tocilizumab: A picture series
Prabhashini Kumarihamy1*; Ashani Ratnayake2; Hiranya Abeysinghe1; Sahan Perera1; Shirley Ekanayake3
1 Consultant Physician, Specialised COVID-19 Treatment Unit, Base Hospital, Teldeniya, Sri Lanka.
2 Consultant Anaesthetist, Specialised COVID-19 Treatment Unit, Base Hospital, Teldeniya, Sri Lanka.
3 Consultant Radiologist, Specialised COVID-19 Treatment Unit, Base Hospital, Teldeniya, Sri Lanka.
*Corresponding Author: Prabhashini Kumarihamy
Consultant Physician, Specialised COVID-19 Treatment
Unit, Base Hospital, Teldeniya, Sri Lanka.
Email: Prabhashinikumarihamy@yahoo.com
Received : Aug 09, 2021
Accepted : Sep 17, 2021
Published : Sep 24, 2021
Archived : www.jcimcr.org
Copyright : © Kumarihamy P (2021).
Citation: Kumarihamy P, Ratnayake A, Abeysinghe H, Perera S, Ekanayake S. Life-threatening secondary infection in a patient with Covid-19 pneumonia treated with tocilizumab: A picture series. J Clin Images Med Case Rep. 2021; 2(5): 1324.
Clinical image description
As of February 2021, cumulative high-certainty data shows that Tocilizumab decreases the risk of mechanical ventilation in hospitalized patients with Covid-19 [1]. COVID-19 patients receiving tocilizumab may have a theoretical risk of acquiring a secondary infection due to immunosuppression [2]. Here we present a series of chest radiographs of a patient presented with severe Covid pneumonia who improved rapidly with tocilizumab but died of secondary infection later on.
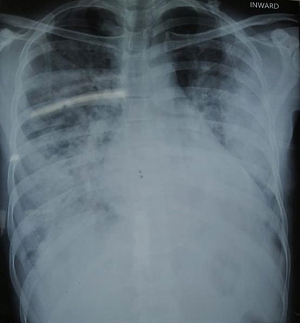
A 33 year old male with a history of type 1 diabetes for 8 years was transferred from a local hospital due to desaturation with a history of fever, cough, difficulty in breathing and positive rapid antigen test for Covid-19. On admission, he was tachypneic, tachycardic with a heart rate of 116/min, blood pressure of 125/70 mmHg and pulse oximetry reading was of 90% on air. He deteriorated rapidly over the next few hours requiring intubation and mechanical ventilation. He was continued with intravenous antibiotics, dexamethasone and prophylactic anticoagulation. The first chest x-ray on the day of admission showed widespread consolidation involving all lobes with both lungs with relative sparing of both apical regions (Figure 1). He was treated with Tocilizumab with his rapid deterioration.
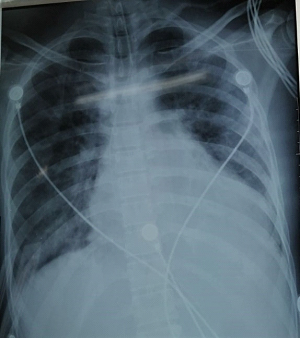
A chest x-ray taken after ten hours of Tocilizumab showed radiological improvement with significant resolution of consolidation in both lungs (Figure 2) with CRP of 125 and procalcitonin of 0.02 ng/ml. He was started to wean off the ventilator and was able to maintain with minimal ventilator support.
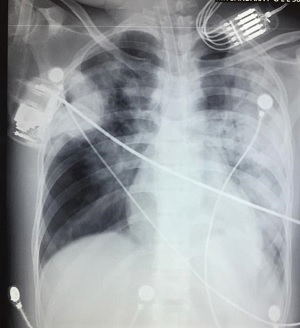
On day six of admission, his condition deteriorated again requiring higher ventilator settings. There was dense consolidation involving most of the left lung with consolidation in mid and upper zones of the right lung in his chest X-ray (Figure 3) with rising CRP and procalcitonin of 1.25 ng/ml. He became haemodynamically unstable requiring ionotropic support. His antibiotic was escalated to meropenem, teicoplanin and colistin. Despite these, he continued to desaturate and died the following day.
References
- Tleyjeh IM, Kashour Z, Riaz ML, Hassett VC Veiga, Kashour T. Efficacy and safety of tocilizumab in COVID-19 patients: A living systematic review and meta-analysis-first update. Clin Microbiol. Infect. 2021.
- Moore JL, Stroever SJ, Rondain PE, Scatena Rn. Incidence of Secondary Bacterial Infections Following Utilization of Tocilizumab for the Treatment of COVID-19 – A Matched Retrospective Cohort Study. J Glob Infect Dis. 2021; 13: 67.