
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
CPAP - The choice of the mask does matter
Bordas-Martinez J; Salord N*; Calvo M; Monasterio C
Multidisciplinary Sleep Unit, Pulmonology Department, Bellvitge University Hospital, IDIBELL, Hospitalet de Llobregat (Barcelona), Spain.
*Corresponding Author: Neus Salord
Multidisciplinary Sleep Unit, Pulmonology Department,
Bellvitge University Hospital, IDIBELL, Hospitalet de
Llobregat, 08907, Barcelona, Spain.
Email: nsalord@bellvitgehospital.cat
Received : Aug 23, 2021
Accepted : Sep 21, 2021
Published : Sep 28, 2021
Archived : www.jcimcr.org
Copyright : © Salord N (2021).
Abstract
We present a case of a patient with uncorrected Obstructive Sleep Apnea (OSA) despite good CPAP compliance with an oronasal mask who was referred to our tertiary care multidisciplinary sleep unit. We present here our systematic and comprehensive re-evaluation of the case, accompanied by an image of the polysomnography recordings that exemplify each step in the process, which concludes with a change to nasal CPAP and a transition to BPAP treatment.
Keywords: obstructive sleep apnea; CPAP; BPAP; oronasal mask; nasal mask.
Citation: Bordas-Martinez J, Salord N, Calvo M, Monasterio C. CPAP - The choice of the mask does matter. J Clin Images Med Case Rep. 2021; 2(5): 1329.
Introduction
Continuous Positive Airway Pressure (CPAP) is the gold standard treatment for moderate-severe Obstructive Sleep Apnea (OSA). Nasal CPAP was initially conceived by Sullivan [1], with the aim that the positive pressure transmitted through the nose would keep the upper airway open, pushing the soft palate and the tongue anteriorly, thereby preventing recurrent episodes of obstruction. Nasal obstruction and oral leak are frequent problems in these patients, to prevent them there is an increasing trend towards an oronasal CPAP prescription [2]. Regarding a complex clinical case of severe OSA, we review here the importance of mask selection for the correction of upper airway obstruction.
Case report
A 54-year-old male, former smoker (accumulated dose 15 packs/year), with arterial hypertension, dyslipidemia and type 2 diabetes mellitus, with vascular involvement (diabetic retinopathy and intermittent claudication), who had consulted at his local hospital for daytime hypersomnolence (Epworth Sleepiness Score [ES] 12), unrefreshing sleep, loud snoring, witnessed apneas, and frequent episodes of choking. He was diagnosed with severe OSA by home respiratory polygraphy (Apnea-Hypopnea Index [AHI] 48.6/h, 38% of mixed apneas and the rest obstructive events, cumulative time with a saturation under 90% (CT90) of 38% and a mean night saturation of 87%). Home APAP titration was performed, which determined an optimal pressure of 11 cm H2 O (visual 90% percentile of pressure), it is not known which type of mask was used. An oronasal mask was administered during follow-up. Given the persistence of somnolence, overnight pulse oximetry was performed under CPAP treatment, which showed a ‘saw tooth’ pattern, with an oxygen desaturation index of 3% (ODI 3%) of 46/h, and a CT90 of 31%. The patient was referred to our tertiary care multidisciplinary sleep unit for manual CPAP titration under Polysomnography (PSG), revaluation, and management.
Our initial physical examination revealed a body mass index of 34 kg/m2 and baseline oxygen saturation of 95%, modified Mallampati tonge position class IV, Friedman tonsillar class II and soft tissue enlargement. Despite objective CPAP compliance of 7.7 hours/night, nocturnal apneas and daytime sleepiness persisted (ES 12). Manual CPAP titration was performed under PSG (Figure 1A) with the patient’s usual oronasal mask (Mirage Quattro size M, Resmed). A lack of correction of obstructive events was observed despite progressive CPAP increases until 14 cm H2 O (residual AHI 58/h and CT90 34.5%). There was no evidence of any significant leak.
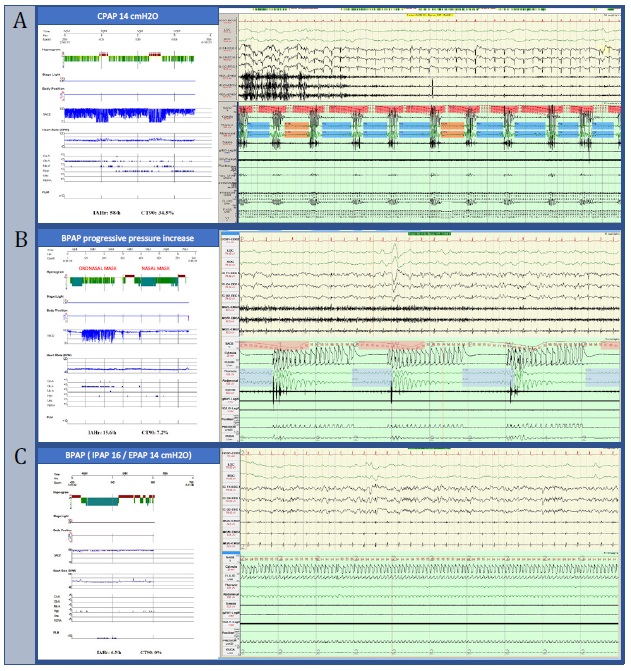
An otorhinolaryngologist evaluation described a mild nasal obstruction and elongated soft palate with hypertrophy of the tonsillar pillars. The patient was not considered tributary to surgical treatment. Due to the absence of correction despite high CPAP pressures, Bi-Level Positive Airway Pressure (BPAP) regulation was performed under PSG (2). Obstructive events persisted despite reaching EPAP [expiratory airway pressure] / IPAP [inspiratory airway pressure] pressures of 16 / 24 cm H2 O (Figure 1B). Therefore, the oronasal mask was changed to a nasal mask and we observed a correction of events with lower pressures: EPAP 14 / IPAP 16 cm H2 O (see PSG image Figure 1.C) (residual AHI 1.4/h; CT90 0.3%). In addition, it was found that nasal CPAP did not correct the obstructive events either with CPAP at 14 cm H2O.
Discussion
Nasal CPAP is considered the "gold standard" treatment for patients with moderate-severe OSA [3]. However, good results of oronasal CPAP were described in the 1990s in patients with severe nasal obstruction [4]. Employed occasionally at the beginning, its use has progressively increased and has been questioned by some authors [2]. However, although there are few published cases, it has been described that the administration of oronasal CPAP can produce a paradoxical induction of apneas and hypopneas [5,6]. Different mechanisms have been proposed to explain this phenomenon. On the one hand, the use of the oronasal mask can cause mandibular retropulsion and posterior displacement of the tongue, leading to obstruction of the upper airway [7]. Furthermore, the oral opening, inherent in the use of oronasal masks, also induces the reduction of the retropalatal and retroglossal space, increasing airway resistance [8]. Finally, the increased contact surface of the oronasal interface increases the risk of perimask leak which may decrease mask pressure. It should be taken into account that, apart from the above-described paradoxical effect, in general, compared to nasal CPAP, oronasal CPAP is associated with higher pressure requirements (+1.5 cm H2O), increased residual events (+2.8/h), lower average CPAP use (-48 minutes), increased leak and lower patient satisfaction [9]. The reason for initiating treatment with oronasal CPAP is very often that the patient reports preferential mouth breathing, despite the fact that many of them potentially could adapt to nasal CPAP [8].
Conclusion
In conclusion, the use of nasal CPAP should be the first choice in the treatment of OSA. The choice of mask type should be individualized for each patient to ensure comfort, which will ultimately determine long-term adherence to treatment [10]. However, although the use of oronasal masks may be useful, the possibility of the described paradoxical increase in obstructive events should be taken into account during follow-up.
References
- Sullivan CE, Berthon-Jones M, Issa FG, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981; 317: 862–5.
- Berry RB. Retrospective: When Were Oronasal Masks First Used to Treat Obstructive Sleep Apnea? J Clin Sleep Med. 2017; 13: 523–4.
- Mediano O, González Mangado N, Montserrat JM, Alonso-Álvarez ML, Almendros I, Alonso-Fernández A, et al. Documento internacional de consenso sobre apnea obstructiva del sueño. Arch Bronconeumol. 2021; 81: e89–92.
- Sanders MH, Kern NB, Stiller RA, Strollo PJ, Martin TJ, Atwood CW. CPAP Therapy via Oronasal Mask for Obstructive Sleep Apnea. Chest. 1994; 106: 774–9.
- Westhoff M, Litterst P. Obstructive sleep apnoea and non-restorative sleep induced by the interface. Sleep Breath. 2015; 19: 1317–25.
- Schorr F, Genta PR, Gregório MG, Danzi-Soares NJ, Lorenzi-Filho G. Continuous positive airway pressure delivered by oronasal mask may not be effective for obstructive sleep apnoea. Eur Respir J. 2012; 40: 503–5.
- Genta PR, Kaminska M, Edwards BA, Ebben MR, Krieger AC, Tamisier R, et al. The importance of mask selection on continuous positive airway pressure outcomes for obstructive sleep apnea an Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2020; 17: 1177–85.
- Madeiro F, Andrade RGS, Piccin VS, Pinheiro G do L, Moriya HT, Genta PR, et al. Transmission of Oral Pressure Compromises Oronasal CPAP Efficacy in the Treatment of OSA. Chest. 2019; 156: 1187–94.
- Andrade RGS, Viana FM, Nascimento JA, Drager LF, Moffa A, Brunoni AR, et al. Nasal vs Oronasal CPAP for OSA Treatment. Chest. 2018; 153: 665–74.
- BaHammam AS, Singh T, George S, Acosta KL, Barataman K, Gacuan DE. Choosing the right interface for positive airway pressure therapy in patients with obstructive sleep apnea. Sleep Breath. 2017; 21: 569–75.